Prevalence
study of
sun
protection behaviors / practices
in
several
representative population
samples
in
Indonesia
Masamitsu lchihash i-l, Setyawati B udinin gsih2.
Mochtar
Hamzaha, uKanoko5. Evert Poetiray',
NoUuo Munâiata7, Herman Ciptoa,ll2
Ohnoetalt
Department of Preventive Medicine, Nagoya University School of Medicine, Nagoya 466-8550, Japan2
Department of Community Medicine, Faculty of Medicine, University of Indonesia, Jakarta 10320, Indonesia
3 Department of Dermatology, Kobe University School
of
Medicine, Kobe 650-0017, Japan
a Department of Dermatology, Facuky of Medicine, University of Indonesia, Jakarta 10430, Indonesia
s Department of Anatomic Pathology, Facuby of Medicine,
University
of
Indonesia, Jakarla 10430, Indonesia 6Department of Surgery, Faculty of Medicine, University
of
I ndone s ia, J akarta I 04 3 0, Indone sia7 Rodiobiology Division, National Cancer Center Research I nst itute, Tolcy o I 04 -004 5, J apan
Med J Indones
Non-melanoma
skin
cancer
(NMSC)
is
the
mostcommon
type
of
cancer
in
white population,
and its
incidence
has increasedworldwide over the last
few
decades.r-a Thisincreasing trend
might
be
in
part ascribedto
suchrecently changed
environmental
andsocio-cultural conditions as depletion of the atmospheric ozone layer, increasing aged
population
(in
developed countriesin
particular),
increasingoutdoor
recreationalactivities at
shadelesssites,
increasing concem
aboutNMSC
among
the public at large which
resulted
in
much earlier hospital
visits,
and earlier
diagnosis/recognition
by medical
professionals who
havebecome more aware of
NMSC.-Abstrak
Kanker kulit non-melanoma (KKNM) yang agak sering ditemukan dan tersebar
di
berbagai negaradi
dunia, diperkirakan paling ntungkin dicegah dengan perubahp erilaku./praktek berlindung dari prevalensi adalah penting u,1tuk m attributable risk percentaqe" (PA
ntelakuknn perilaku perlindungan bersama dengan Rasio Odds un
dalam runius perhitut'tgan, sJperti diuraikant secara terperinci dalam bagian kedua
dari
makalahini.
Sebelum kami dapat p,roporsi yangclapat
ntu
n
khas untuk kelompoketnik
dari
KKNM
oLeh tiap ktek'perlindungont"rho
In
i
mengajukan 10 pedoman sederhana untuk membanturisiio
terjadiiyakanker
di
erika Serikat, karena dipandang berguna untuk Indonesia sebagai pedoman sementara untuk pencegahnn KKNM.Abstract
Non-melanoma skin cancer (NMSC), which
is
rather common and worldwide, is considered to be mostly Preventable by simple behavioral change. This ittitiated the authors to propose a prevalence,stu.dy of sutt protection behaviors/ Practices among several representatives population samples in Indonesia.ihii
prruolinre
study is,,essentialfor providing the prerequisite data to calculate .the pieventableproportion' i.e.
p:opulation attibutable ;isk Percentage(PARP)'
be obtained by 'ronconAccording
to
numerous, _investigations
mostly
onCaucasians,
as reviewed,'-' the primary
risk
factorsfor
development
of
NMSC are
excessive
ultraviolet
radiation and personal characteristics
associatedwith
increasedskin
sensitivity
to ultraviolet
radiation
suchas
light
skin color,
easy sunbuming, and
little
or
noability to
tan.
Relevant
epidemiological
evidence
issummarizedT
as follows: NMSC
occur.6
(l)
morefrequently
in
residents
of
areas
with high
ambientsolar irradiance,
(2)
more
frequently
in
sun-sensitivepeople,
(3) mainly on
sun-exposed
body sites,
(4)more frequently
in
people
with
high sun
exposure,and (5) more frequently
in
people
with benign
sun-related
skin
conditions,
andNMSC is (6)
reducedby
protection
of
the skin
against the
sun. In
our
Japan-Indonesia
joint
research
project
on
skin
cancer,
animportance
of
sun exposurein
developing
NMSC
wasalso
suggestedby
thepreliminary
analysisof
the dataobtained
from
ongoing case-control study
on
skin
cancer
in
Jakarta.Based
on
thesescientific
evidence,
themost effective
counter-measure against
NMSC
is
considered
to
besun protection
behaviors/practices
such as
avoiding
sun exposure
especially during midday
hours, wearingprotective clothing and
hat
and wearing
sunscreenlotion with
a
sun protection factor (SPF)
of
15
or
higher.s
It
is
also
important
to
note that
80
Voof
a
person'slifetime
sun exposureis
estimatedto
occur before
the ageof
2le
andthat
useof
a
sunscreenwith
a
SPFof
15 or higher during childhood
and
adolescence mayreduce
the lifetime risk
of
both
basal and
squamouscell
carcinomasof
theskin by
as much as 78%o.t0In
order
to
develop
major
countermeasures
againstNMSC
in
this
country,
we
need
to
know the
pre-valence
of
actual sun protection
behaviors/practicesby
a
deliberate
survey
in
several
representativepopulation
samples
in
Indonesia and odds
ratio
aswell by
each sunprotection behavior,
which
are basicinformation
for
calculating population
attributable
risk
percentage(PARP),
becausePARP
will
tell
us
apreventable
proportion
of
NMSC
by
each
sunprotection
behavior/practice. Odds
ratio by
each
sunprotection behavior
will
be obtainedfrom
our ongoing
case-control study
in
Jakarta,which
will
be describedin
detail
somewherein this
monograph.In
this
communication, therefore,
some
surveysscheme
for
a
prevalence study
on
sun
protection
behaviors/practices
will
be
discussed,
including
sampling method, organizational framework
of
thesurvey and items
to
be
surveyed,
along
with
brief
explanation of
PARP.Defïnition
of
population
attributable
risk
percent
and
attributable risk number
PARP
is a genuineindicator of
preventableproportion
of
a given
diseasein
a total population
by a
given
factor, i.e.
aproportion
(expressedin
percentage)of
agiven
diseaseof
outcomein
atotal population
that can be removedif
the exposurewere avoided completely,
under the
two
assumptions:
(1)
those
with a
given
factor (ex
smokers);
and(2)
other
etiological
factorsare
equally distributed among those exposed
and those not-exposed.PARP is
avery useful index
in
planning
and assessingany
diseasecontrol
programs, since
it
enables healthadministrators
to
estimate
the
extend
to
which
aparticular
diseaseis
due
to a
specific factor and
topredict
the
effectiveness
of
a control program
which
intend
to
reduce
a
specific
disease
by
eliminating
exposure to a specified factor.
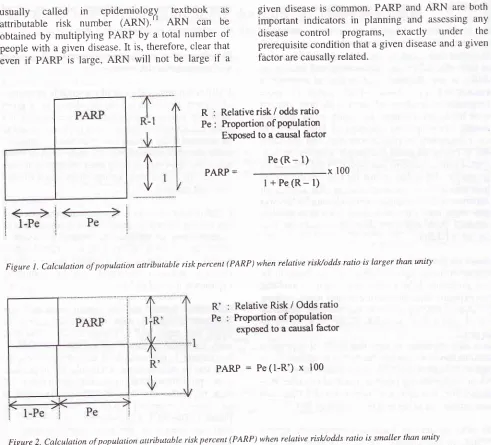
Conceptual figures
and
calculation
formulaet'
areillustrated
in Figure
1,when relative risk/odds
ratio
islarger than
unity
and
in
Figure
2,
when less
thanunity.
Exemplified
calculations
areshown
in
Table
1.In
example
l,
relative risk
of
cigarette
smoking for
lung
cancer
in
rnales
was arbitrarily
set
to
be
4.13with
aproportion (70
Vo)of
current
smokersin
atotal
male population and
then,
PARP was
calculated- as68.7 Vo
by
inserting
4.13
and0.70
into
the
formula
in
Figure
1.This
68.7 Voimplies
that
this
percentageof
total lung
cancer
is
due
to
cigarette smoking;
in
another words,
if
all
male
smokers became
non-smokers,
68.7
Vo
of
total lung
cancer
could
be avoided/prevented.In
example2, relative
risk of daily
intake
of
green-yellow
vegetablesfor
lung
cancer wasset
to
be 0.8 (protective) and daily
eaters
of
green-yellow
vegetableswere
accountedfor
407oin
a total
population
and then,
PARP
was computed as
8.0
7oby inserting 0.8
and0.40
into
theformula in
Figure
2.This
8.0 Vo means thaLO.SVoof total lung
cancercould
be avoided/prevented.
PARP,
thus, indicates
the proportion
(in
percentage)of
contribution
of
a
certain factor
for
developing
agiven
diseasesor
outcome,i.e.
preventableproportion
by
acertain factor.
It
doesnot, however, indicate how
many people
were
attributable
to a
given
factor
usually
called
in
epidemiology
textbook
asattributable
risk
number
(ARN).r' ARN can be
obtained
by multiplying PARP by a total
number
of
people
with a
given disease.
It
is, therefbre, clear
thateven
if
PARP
is large, ARN
will
not be large
if
all4
Ohno et al Med J Indonesgiven disease
is
common.
PARP
and
ARN
are
bothimportant indicators
in
planning and assessing
anydisease
control
programs,
exactly under
theprerequisite condition that
a given disease and a givenfàctor are
causally related.R Pe
Relative risk
/ odds ratio
Proportion of poPulation Exposed to a causal factorPe
(R- 1)
r
PARP =x
100 [image:3.558.55.546.81.526.2]l+Pe(R-l)
Figure t . Calculation of population attributable risk percent ( PARP) when relative risuodds ratio is larger than unity
Relative Risk
/ Odds
ratto Proportion of poPulationexposed to a causal factor
PARP:Pe(l-R')x100
Figure 2. Calculntion of population attributable riskpercent (PARP) when reLative risl<lodds ratio is smaller than unity
Table
l. Exemplifiecl calculation of population attributable risk
percent (PARP) t,,Example
I
(when relative risk / odds ratio>
1 00)R
for lung cancer by smoking..'
4'13 Proportioi of male smokers... 'lO'O VapRip
= {Pe(R-l)
/u+
Pe(R-l) l}x100-..
68'7 voExample
2
(when relative risk / odds ratio < 1.00)R'
Pe
R forlungcancerbydailyintakeofgreen-yellowvegetables
" "
9!0
Proportion of daity eaters of green-yellowvegetables
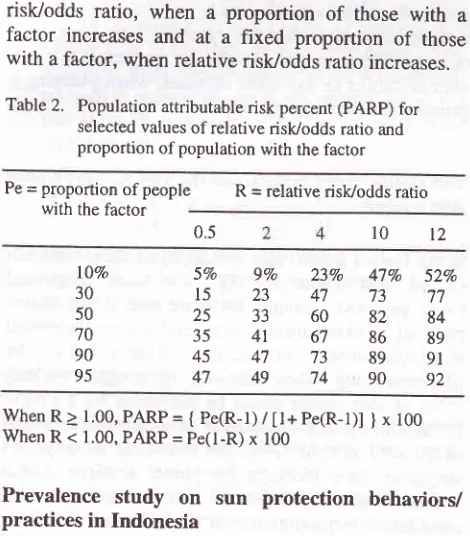
40'0 VoFor
much clearer understanding Table
2 is
presented,that
shows
a
PARP value
for
selected values of
relative risk/odds
ratio
andproportion of
people
with
a factor.
A
PARP value
increasesat a fixed
relative
risk/odds ratio, when
a
proportion
of
those
with
afactor
increases
and
at
a
fixed
proportion
of
thosewith
afactor,
whenrelative risk/odds ratio
increases.Table
2.
Population attributable risk percent (pARp) forselected values of relative risk/odds ratio and
proportion of population with the factor
Pe
-
proportion of people R = relative risk/odds ratiowith the factor
23Vo
47Vo
52Vo47 73
7760 82
8467 86
8973 89
9l
74 90
92condition
of
"representativeness
of
the
sampledpopulation".
When
selecting candidate areas
(villages/tov.vns), severalsampling methods are available, as shown
in
Table
3
and
for this
purpose
a
probability
proportionate sampling may
be adequate and suitable.After
selecting
areasto
be
studied,
we
may
adoptsimple random sampling method
to
select inhabitantsto be
studied. Inhabitants
to be
selectedat this
stageshould
be
thosein childhood
and
in adolescence
andthose aged
old
enoughto
get skin
cancer aswell.
For
those
in
childhood and
adolescence,information
onpresent
sun
protection
behaviors/practices
will
becollected and
for
those
agedold
enough
to
get
skin
cancer,
past
(in
childhood
and
adolescence)
andpresent
(middle
age
and
thereafter)
information
should
be done.The items to
bepossibly collected
in
relation
to
sun
protection behaviors/practices
arelisted
in
Table
4
and other
information ùtrictr
shouldbe
inquired in Table
5.Table
3.
Sampling method for candidate villages or towns andinhabitants to be studied
(l)
Simple random sampling(2)
Systematic random sampling(3)
Probabilityproporrionatesampling(4)
Stratifiedsampling(5)
Cluster sampling(6)
Multi-stagesampling(7)
Multi-phasesampling(8)
Sampling for time seriesTable
4.
Information to be collected by direct interview on sunprotection beh avi or/practices
(1)
Skin sensitivity (Skin type)(2)
Skin reaction after l-hr sun exposure(3)
Skin reaction after long exposure to sun(4)
Use of protective clothing such as wide-brimmed hats/
long-sleeved shirts
(5)
Practices ofStay in shade(6)
Use of sunscreen / sunblock lotion(7)
Exposure to artificial source ofultraviolet light(8)
Other behaviors / practices (regular skin self-exam., etc)Table
5.
Basic information to be collected by direct interviewDemographic information
Ethnic group,
Age,
Sex,
Marital status, Education, Religion, Annual income, etc.Past and
family history
of
skin
cancerand
othercancers
Lifestyles
Cigarette smoking habits, Drinking habits, etc
t2
l0
05
5Vo
9Vo15
2325
3335
4t
45
4747
49lOVo 30
50
70 90
95
When
R>
1.00, PARP = { pe(R-l) /t1+pe(R-l)l
}x
100 When R < 1.00, PARP = Pe(l-R)x
100Prevalence
study
on sun
protection
behaviors/
practices in Indonesia
For
calculating preventable
proportion
of
skin
cancerin
Indonesia,
we
need
to
know
relative
risks/oddsratios
by
each sun protection
behavior/practice
andproportions
of
those
practicing each sun
protection
from
area
to
area
in
Indonesia.
The former
information
will
be
readily
available
from
our
ongoing
case-control
study
on
skin
cancer.
To
our
best
knowledge, the latter
information
arenot
readily
available
at
moment
from any
sourcesin
Indonesia.This essentially
meansfor
usto
haveto
undertakeour
own
prevalence study
in representative population
samples
in
Indonesia.
Then,
we
will,
here,
propose such astudy/survey, i.e.
who
should
investigate what, where,whom, when
andhow.
First,
where,whom
andwhat should
we survey?In
order
to
obtain
representative prevalence figures,
we
need,
first,
to
seleçt
areas
(villages
or
towns)
possibly
throughout Indonesia
as
representative samplesby reliable
sampling method.
V/e
had
betterstart such
a
prevalence study as
a pilot
study
of
investigating
the feasibility
of
the
survey
and,therefore,
we may
select several
areasat
least
at
aninitial
stagewhere the survey
would
be considered to besuccessfully
conducted and increase thenumber
of
areas
to
be
studied aftdrward
in
order
to
satisfy
the(l)
(2)
[image:4.594.307.548.73.734.2] [image:4.594.54.289.128.396.2]1
16
Ohno et alSecond,
who
should
collect all
necessaryinformation
when
and how?
In
order
to
undertake
such
acountrywide
study,
we
needto
otganizecertain study
teamsby whom
an actual surveywill
be done at
eacharea
by
directly
interviewing individuals
who
areselected
as study
subjects
(population
samples)
and such study teams should be, at acentral administrative
office,
co-ordinated
and
integrated'
Responsibleinterviewers should be
sufficiently
trained to maintain
intra- and
inter-viewer variations
as
minimal
aspossible,
by
sftuctured-questionnaire' Sunprotect
iceswill
be different by seasonfrom
areato
areain
Indonesia,
but
a survey atthe
hottest season
at
each area will
be
good enough
for
collecting
all
information.
Information to
be
disclosed
by
analyzing the data
obtained
from
the
proposed prevalence
study in
Indonesia
The major
obtained t
practicing
which
will
goal,
the
lYof
NMSC
ere
disclose
in
Table 6. Ethnic group-specific
analysis
will also
beuseful
in
such
a
country
with
multi-ethnicity
asMiddlè
age and thereafter).Table
6.
Exemplified information to be disclosedby
data analYsisArea/ethnic group-specihc prevalence rates
of
skin sensitivityArea
i
éthnic group-specific prevalence ratesof
sunprotection behaviors/Practices
Factors associated
with
likelinessof
practicing sunprotection (protective clothing,
stay
in
shade, sunscreen/sunblocklotion)
Fâctors associated with skin sensitivity
What
din
this
tYPeof
study
studiedin
eachbe
no
not regarded
asno longer
values
after
obtaining
the
relevant
information. They
should be deliberately
followed
upMed J Indones
for a
certain period
of
time
in
order
to examine
whether they
finally
develop
skin
cancer
or
not. This
follow-up
studywill
be named as a "population-basedcohort
study
on
skin
cancer."
In
this
paper,
\veproposed
a
prevalence
study
on
sum
protection
behaviors/practices,but this type
of
study design
and conceptualframework
will
also be applicableto
other sitesof
canceror
any other
diseases,when planning
aprimary prevention
program.Ten simple
ways
to help cut the
risk of
developing
skin
cancer
In
theUnited
States, skin canceris
the most commoncancer,
with
about 800,000
new
cases
diagnosedeverv
vear
and accounts
for
more than 2,000
deathsp",
y"ur.''
Skin cancers,
in
general, areeasily treated
and
highly
curable when
diagnosedearly,
but
can belife-threatening
when
allowed
to
progress.
Many
casesof
skin
cancercould be
prevented
by a
simplebehavioral change (avoidance
of
excessive exposure
to the
sun) and therefore,
the following
10 ways
aresuggested
as
a
messagefor
public at
large
in the
UniteO
States.12
These
10
simple
tips
are
alsoconsidered,
in part,
asuseful
for
Indonesians,
beforelndonesia-specific
guidelines are to be shownby us'
1) When outside,
alwaY
with
a sunprotection
factor
(SP
on
exPosedparts
of
Your
bodY.
sunscreensmay
allow
you to burn
if
the sunis
strongor your
exposure
is
long.
Higher
SPF levels are
even better.2)
Reapply
sunscreenfrequently (about
2
hours
or
sooner
if
going
swimming
or
perspiring
very
heavily).
Select
a
sunscreenthat blocks
UVA
(ultraviolet
A)
andUVB
(ultraviolet
B) light.
Wear protective clothing such as hats
or
shirtswhen outside
for
any period of time.used.
Avoid
midday
sun
exposure.
Ultraviolet
raysfrom the sun are
strongest
(and are
mostdamaging) between
10
AM
and 3
PM'
If
at all
porribl", t
y to stay indoors during this tirne or day' 3)4)
s)
(l)
(2)
(3)
(4)
7)
Avoid
exposureof artificial
sourcesof
ultraviolet
light
such as lamps and tanning booths.8)
Be careful about protecting your children from
the
sun. Children
who
suffer
severe
sunburnsduring
childhood
aremore
likely to
develop
skincancer
later
in lifè
thanchildren who
neversuffer
sunbums. Sunscreen,
however, is not
recommend-ed
until 6
months
of
age (keepinfants
out of
thesun
asmuch
aspossible),
but
can be safely
usedafter 6
months
on mostchildren.
9)
Perform regular
self-examinations
of
your
skin(every
month
is
recommended
by the
American
Cancer Society).
l0)
Have your
physician
perform regular skin
examinations (every year
is
recommendedby
theAmerican
Cancer Society).
Acknowledgement
We
areindebted
to
theIntemational
Cancer ResearchGrant
system, Monbusho, Japan
and
the
Dean,Faculty
of
Medicine,
University of
Indonesia, Jakarta,for his
approval
of
the Japan-Indonesiacollaborative
study.
This work
has been supportedby
the grant
no.09042004, under
Ministry
of
Education,
Science,Sport and Culture, Government
of
Japan
and
waspartly
supportedby
the Indonesian Cancer Foundation, the JakartaInternational
Cancer ConferenceFund
andthe
Terry Fox
Foundation,
Canada.The collaborative
study was
initjated
with
Dean's
approval no.
845{PT02.H4.FK{E/97
and technical
supporr
by
theDirector
of
Dr.
Cipto
Mangunkusumo
National
Central
GeneralHospital.
REFERENCES
l.
MarksR.
An
overviewof
skin cancers. Incidence andcausation. Cancer 1995: 75:. 6Oi -12.
2.
Corona R. Epidemiology of non-melanoma skin cancer: areview. Annal dell Instituo Superiore di Sanita, 1996:32:
37-42.
3.
Quinn AG, Ultraviolet radiation and skin carcinogenesis. Brit J Hop Med 1997; 58l.261-4.4.
IchihashiM,
NaruseK,
Harada S, et al. Trendsin
non-melanoma skin cancer in Japan. Recent Results in Cancer Res 1995; 139:264-73.5.
Kricker A, Armsrrong BK, English DR. Sun exposure andnon-melanocytic skin cancer. Cancer Causes and Control 1994;5:369-92.
6.
Strom SS, Yamamura Y. Epidemiology of non-melanoma skin cancer. Clinics in Plastic Surgery,1997;24 6Zj-36.7.
EnglishDR,
ArmsrrongBK,
Kricker
A, Fleming
C. Sunlight and cancer. Cancer Causes and Controls,1997:8:271-83.
8.
American Cancer Society. Cancerfacts and
figures. Atlanta (GA): American Cancer Society, 199g.9.
Banks BA, Silverman RA. Schwartz RH, Tunnessen WW. Altitude of teenagers toward sun exposure and sun screenuse. Pediatrics 1992; 89: 40-2.
10.
Stern RS, Weinstein MC, Baker SG. Risk reduction for non-melanoma skin cancer with childhood sunscreen use.Arch Dermatol 1986:122: S3j-45.
11.
Tominaga S, OhnoY.
Introduction to Epidemiology for Clinicians. Nihon-Izi-Shinpo-sya. Tokyo, l9g9: 37-41 (inJapanese).
12.
Page for patients,A
message from preventive Medicine