Keep it at the bedside for a quick refresher on ICU nursing implementations and to help troubleshoot mechanical devices used in the ICU. I am happy to share the knowledge I have gained as a travel nurse in collaboration with some of the best nurses, doctors and support staff in the country.
INTRODUCTION
QUALIFICATIONS
During unit orientation, a nurse is assigned a preceptor, who begins learning critical care techniques. Education and training must be continuous throughout critical care nursing to ensure up-to-date skills and competence.
CERTIFICATIONS
TYPES OF CRITICAL CARE UNITS
The critical care units mentioned above are explored in the following chapters, which explain the specific instructions, equipment and skills used. A facility may include any available rooms when critical care areas are near capacity.
SELF-CARE FOR THE CRITICAL CARE NURSE
While each specialty unit attempts to use open beds for patients who meet their specialty, ICU nurses must be prepared to care for any type of critically ill or injured patient who may require an ICU bed. By actively providing self-care, nurses improve the quality of care they provide to their patients and relatives.
NURSING STANDARDS OF PRACTICE
THE NURSING PROCESS
Involving patients, families, caregivers and other members of the health care team as far as their abilities and patient safety permit. Evaluation: The process of evaluating the patient's condition and the effectiveness of the treatment.
DOCUMENTATION
The patient tolerated the procedure well and acknowledged the understanding of the procedure, IV education, and care. After completing and evaluating the procedure, the nurse accessed the patient's EHR to document the changes, implementations, and results.
MALPRACTICE
The nurse added details about the appearance of the site and how the IV was removed to ensure adequate documentation. To avoid negligence as well as malpractice issues, nurses must practice under the Nursing Practice Act (NPA) of the state where the care is provided.
ADVANCE DIRECTIVES
Both a living will and a durable medical power of attorney are written documents completed by a person while he or she is competent. If the person is unable to sign, someone other than witnesses or the health care provider can do so.
EYE AND ORGAN DONATION
It is important to provide emotional support and education to the family while trying to honor the patient's wishes, both for and against donation. Once it is clear that a patient wishes to be a donor or if there is no indication of the patient's wishes in this area, medical suitability for eye and/or organ donation should be considered before approaching the family to avoid unnecessary emotional distress.
WITHDRAWAL OF MEDICAL TREATMENT
TERMINAL WEAN
Be immediately available to address family needs and/or provide measures and medications for patient comfort. Then decrease positive end-expiratory pressure (PEEP) and pressure support (PS) until the patient begins to breathe spontaneously.
PALLIATIVE CARE
Deceased loved ones can appear to the patient and "speak". Other visions may also occur. NDA differs from terminal delirium primarily because the patient is not distressed or afraid of the visions.
EMOTIONAL SUPPORT OF THE FAMILY
Explain to them and the patient that this type of experience is normal (Foreman et al., 2010).
HEALTH CARE TEAM EMOTIONAL SUPPORT
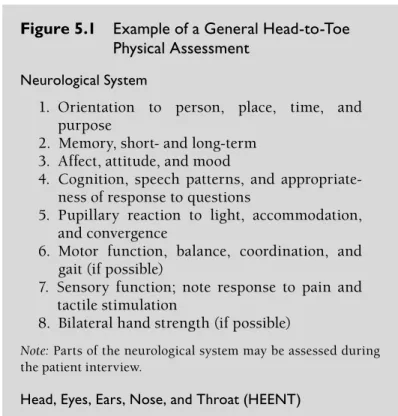
The first step in the physical assessment is to explain to the patient what to expect. Place an additional used pad on the outside of the patient's leg, away from where the sterile field will be.
ASEPTIC TECHNIQUE
Scrub the site and surrounding area in a circular motion with a facility-approved antimicrobial soap, usually chlorhexidine or iodophor. Use sterile gloves, sponges, and forceps unless otherwise instructed and/or equipped. Members of the healthcare team who will participate in a sterile procedure must perform surgical debridement before donning sterile gloves or sterile personal protective equipment (PPE).
This is a vigorous forearm-to-fingertip wash performed for 3-5 minutes with facility-approved antimicrobial soap. After surgical peeling, don a sterile gown and sterile gloves in a clean and/or sterile area away from the actual sterile field to reduce the risk of contamination.
THE STERILE FIELD
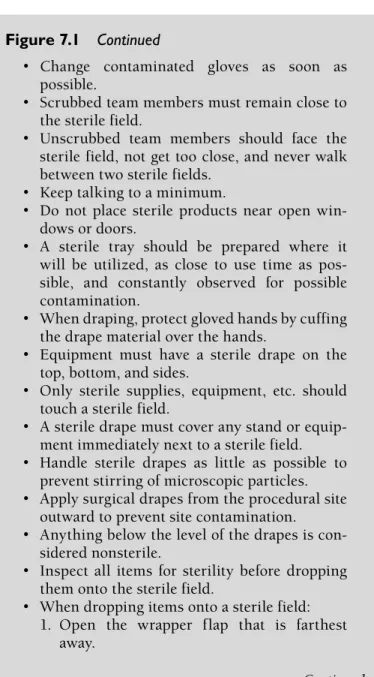
Unscrubbed team members should face the sterile field, not get too close, and never walk between two sterile fields. A sterile tray should be prepared where it is to be used, as close as possible to the time of use, and constantly observed for possible contamination. Hand off items to scrubbed team members in a manner that prevents a non-sterile person or object from reaching across the sterile field.
Pour the solutions into sterile, labeled cups, which the cleaning person places near the edge of the field, not on the "contaminated" part of the field. Any violation of sterility should be corrected immediately, unless contraindicated for patient safety.
INFORMED CONSENT
Afterwards, when all the patient's questions have been answered, an informed consent form is signed. The form verifies that the conversation between the doctor and patient took place and that both agreed on the procedure. If the patient cannot give consent due to physical and/or mental incapacity, a legal guardian, healthcare proxy or the next of kin can give consent.
If no family member or guardian is available, two doctors may indicate that the procedure must be completed due to a serious risk to the patient's health.
PRE-PROCEDURAL PATIENT PREPARATION Patient Education
Transmission-based precautions should be taken at the time the patient presents with symptoms indicative of possible infection, as laboratory identification and/or confirmation of microorganisms may take several days. A mask, eye protection and/or face shield should be worn during tasks where there is a possibility of splashes and sprays of blood, body fluids and/or secretions. Signs indicating the type of transmission-based precautions required to enter the patient's room should be prominently posted outside the patient's room, along with instructions on how to properly apply personal protective equipment.
Necessary equipment and supplies should be available near the entrance to the patient's room. The starting glove should be inside the second glove, which will be facing out.
SUPPLEMENTAL OXYGENATION
INTUBATION Endotracheal Tube
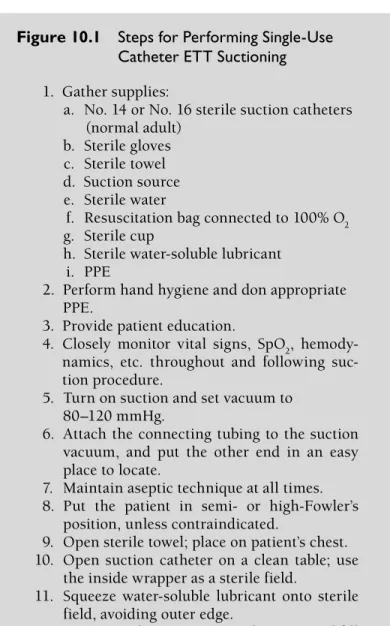
Reposition the ETT from one side of the mouth to the other to prevent mouth/lip pressure sores, at facility-approved intervals. Attach the connecting tube to the vacuum cleaner and place the other end in an easy-to-find location. Easily insert suction catheter into the ETT, without applying suction, until minimal resistance is achieved.
Clean the suction catheter between passes by dipping the tip into sterile water and aspirating a small amount. The health care team is responsible for providing emotional support and education to the patient and family.
MECHANICAL VENTILATION
Continuous positive airway pressure (CPAP): positive pressure is applied and continued during spontaneous breathing; it is often used for weaning and is contraindicated in ICP. This is the inspiratory volume delivered at a predetermined time to allow adequate expiration. This is the level at which the ventilator detects that the patient is breathing and provides support.
Minute volume (MV; usually 6–10 L/min and defined as the amount of air the patient inhales or exhales), RR and VT are examples. Supplemental oxygenation is their area of expertise, and it is very helpful to have their additional knowledge at the bedside.
EXTUBATION
Before starting a weaning trial, confirm that the patient has received medications that may improve lung tolerance and function, such as albuterol (AccuNeb, Proventil HFA), beclomethasone (Beconase AQ, Qvar), cromolyn (Nasalcrom, Intal), fluticasone (Flonase, Veramyst), formoterol (Foradil Aerolizer, Perforomist), hydrocortisone (Solu-Cortef, Cortef), ipratropium (Atrovent), methylprednisolone (Solu-Medrol), montelukast (Singulair), prednisone (Sterapred), salmeterol (Sereventus), terbutaline (Brethine), theophylline (Theo-24, Theolair), or tiotropium (Spiriva). After weaning trials have been successful, either a doctor or a respiratory therapist will extubate the patient. When extubation is complete, the patient should be closely monitored to ensure compliance and adequate ventilation.
Surgical interventions, interventions, nursing interventions, drug administration and treatment are performed with the aim of improving the patient's condition. Arterial lines and pulmonary artery (PA) catheters provide valuable information to the healthcare team regarding the patient's respiratory status, hydration, and hemodynamic status.
ARTERIAL BLOOD GASES
LINE
A pressure bag is applied to the outside of the bag, applying 300 mmHg force to the fluid, maintaining a flush of approximately 3 cc/hour to ensure line patency. A "box" connected to the monitor, a transducer cable, the transducer, and an air-fluid interface (stopcock) are parts of the system. The stopcock must be flush with the phlebostatic axis to zero the monitoring system after the A line is inserted.
If this type of device is not available, a blood collection port can be used to access the line. Follow aseptic technique and ensure that adequate flushing follows blood withdrawal regardless of the method used.

PULMONARY ARTERY CATHETER
Aided by a pump, the dialysate flows in the opposite direction to the blood, allowing diffusion and convection to occur. It requires double-lumen venous access, a blood pump and dialysis, which flows in the opposite direction of the blood. It requires a double-lumen venous access site, blood pump, and dialysis, which flows in the opposite direction of the blood.
With a properly functioning device, the ECG in demand mode should be at or above the pacemaker's set rate. If loss of capture, inability to detect, or changes in patient condition occur, settings can be adjusted. Changes in the ECG examination, hemodynamics or overall assessment should be reported to the physician immediately.
A Thoratec VAD is used in the hospital and can provide right, left or biventricular support.