Endocrine, Diabetes and Hypertension Division, Department of Medicine, Brigham and Women's Hospital, Harvard Medical School, Boston, MA, ZDA. Catherine Logan, MD, MBA, MSPT Department of Orthopedic Surgery, Brigham and Women’s Hospital, Boston, MA, ZDA.
About the Editors
Definition and Epidemiology of the Female Athlete Triad
Introduction
These three components of the Triad are conceptualized as continuous to reinforce the idea that graded negative health outcomes may occur at different levels of each component; these continua range from optimal health at one end to pathology and disease at the other. This syndrome emphasizes the role of energy deficiency in disrupting multiple dimensions of physiological functioning (including but not limited to menstrual function and bone health) and is an extension of the concept of the Female Athlete Triad.
Energy Availability
Assessment of eating pathology using a validated measurement tool is an additional component in understanding whether an individual may be in energy imbalance, but should not be considered sufficient in isolation given the expanded conceptual definition of this component of the triad [5].
Menstrual Function
Bone Mineral Density
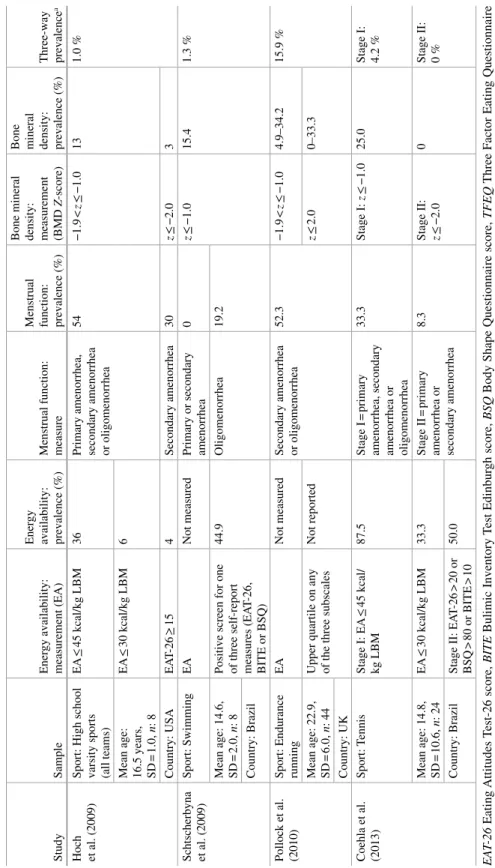
Prevalence
The updated review includes studies reporting the prevalence of at least one clinical and/or subclinical condition of the Triad. In summary, 35 studies examining the prevalence of clinical or subclinical eating disorders or eating disorders were included in the review by Gibbs et al.
Males
Conclusions
By following the criteria described above, the validity and accuracy of the Triad prevalence estimates will be strengthened. Accurately estimating the prevalence of the Female Athlete Triad and its counterpart in male athletes will be critical for informing prevention efforts and monitoring population-level risk changes over time.
Chapter 2
Sports Nutrition
Medicine states that “the basic differences between an athlete's diet and that of the general population are that athletes need extra fluid to replace sweat losses and extra energy to stimulate physical activity” [1. Whether adjusting an athlete's diet is necessary to address an issue such as the female athlete triad or if this is the focus of a performance improvement plan, it is essential to ensure that adequate energy is expended consistently .
Dietary Assessment
If you need more detailed information about an athlete's body composition, body fat percentage can be estimated with a caliper to measure the thickness of subcutaneous fat in several places on the body, including the abdomen, subscapular areas, arms, buttocks and thighs. Once the data is collected, it is important to know what goals the athlete has.
Energy Requirements
However, BMI assessment is a useful tool when included as part of a complete assessment of an athlete's health, especially for those who are underweight or at risk for an eating disorder. The easiest method for determining an athlete's total daily energy needs is to use the Harris Benedict equation (see below), because all that needs to be known is the athlete's weight, height, and age.
The theory behind carb loading is that athletes can maximize their glycogen stores by eating the low recommended amount of carbohydrates starting 6 days before the race or event. The blood sugar response to a particular food depends on the composition of the food, as well as what is eaten together.
Popular products such as gels and chews can provide the necessary fuel and are quickly digested and absorbed by the body. A number of different 'ideal' ratios of carbohydrates to protein have been reported for post-workout, such as 3–1 or 4–1.
Dietary sources of vitamin D can be difficult to find because it does not occur naturally in many forms, except in certain fish and mushrooms grown under special UV lights (see Table 2.3. Sunlight is the body's best source of vitamin D, so during the winter months (or if you use sunscreen during the summer months) it's important to get enough from food sources or take a supplement if you feel medically necessary.
Supplements and Ergogenic Aids
Hydration
This can be done at home by measuring your pre-exercise and post-exercise weight using the equation below [ 5. If you are dehydrated, post-exercise rehydration can be accomplished by consuming 16-24 oz of fluid per pound of body weight lost during exercise. , as determined by the sweat rate test [ 1.
Special Populations
Chapter 3
The Menstrual Cycle
The Normal Menstrual Cycle
Once menarche has occurred, cycles may take up to 2 years to become regular ovulatory cycles; they can be "regularly irregular". Although cycles may not occur every month, they tend to vary between 21 and 45 days [1. Within the first year, approximately 50% of cycles may be anovulatory although 80% will fall within the 21-45 day range.
Defi nitions of Common Menstrual Disorders in Athletes
After ovulation, a corpus luteum is formed which produces progesterone to support the endometrium in anticipation of a fertilized egg. If implantation does not occur after approximately 14 days, the corpus luteum regresses and progesterone levels drop.
Epidemiology of Menstrual Disorders in Athletes
Etiology of Menstrual Dysfunction
The disorder was once thought to be caused by stress associated with the physiological demands of intense exercise. Low leptin levels and high ghrelin levels were associated with lower LH secretion in amenorrhoeic athletes compared to eumenorrhoeic athletes [27].
Evaluation of Menstrual Abnormalities
It is important to remember that any cause of secondary amenorrhea can be a cause of primary amenorrhea (see Table 3.2). In addition, one should focus on possible anatomical or chromosomal abnormalities as a cause of primary amenorrhea.
Treatment of Menstrual Disorders
In secondary amenorrhea, we are not so concerned about primary anatomical abnormalities, since the outflow tract is assumed to be open, given that menstruation has occurred previously. These hormonal abnormalities are generally thought to be due to hypothalamic suppression, hyperandrogenism such as PCOS, elevated prolactin levels, or thyroid dysfunction.
Conclusion
Chapter 4
Exercise and the Female Skeleton
We then discuss the impact of exercise on bone strength during childhood, adolescence, and early adulthood, with a particular focus on studies in girls, including the athlete triad population. We acknowledge that DXA studies have significantly improved our understanding of bone adaptations to physical activity and refer the reader to several excellent reviews of DXA-based studies.
How Bone Adapts to Exercise
Our understanding of bone adaptation to loading has been greatly enhanced by experimental evidence from animal models. The feedback loop between bone deformation (tissue strain) and bone strength is central to the regulation of bone adaptation.
How to Measure Bone Adaptation to Exercise
Thus, when investigating bone adaptation to exercise, important whole bone strength properties such as structure and microarchitecture must be considered. Thus, we should consider 3D imaging techniques such as pQCT, HR-pQCT, and MRI to more accurately measure bone structure and microarchitecture and assess bone strength.
How Exercise Infl uences Bone Development in Children and Adolescents
BC trial (AS!BC), which included brief periods of classroom-based exercise (including ~3 min/day of dancing), girls in intervention schools who reported high compliance (≥80 %) demonstrated 5% greater gains in femoral neck bone strength (section modulus, HSA) compared to girls in control schools [77. Furthermore, while eumenorrheic athletes demonstrated a significant bone strength advantage in the weight-bearing tibia compared with nonathletic controls, amenorrheic athletes did not obtain such benefits (Fig.
Do the Benefi ts Achieved During Growth Persist into Adulthood?
Subsequent analyzes using finite element analysis found lower estimated bone strength (load and stiffness) in amenorrheic female athletes compared to nonathletic controls at the distal radius. Bone strength adjustments in exercisers were associated with 15–28% greater total CSA and BMC (total, cortical, and trabecular) at the radius and 9–15% greater BMC (total, cortical, and trabecular) and trabecular BMD at the tibia compared with non-exercisers .
The Infl uence of Exercise on Bone Strength in Young Adult Women
This contributed to a 36–38% greater estimated bone strength (SSI p ) at the radius and humeral parts (by pQCT) in former gymnasts compared to never gymnasts [121. Women randomized to the exercise group had significant increases in femoral neck bone area (2.8%, CSA) and estimated bone strength (3.2%, section modulus) compared with controls [130.
Summary and Future Directions
Chapter 5
Assessment of Bone Health in the Young Athlete
When the American College of Sports Medicine (ACSM) first described the female athlete triad in 1992, the term “osteoporosis” was used to describe the effects of the triad on bone health [1, 2]. This change in terminology better refl. it affects the spectrum from optimal bone health at one end to osteoporosis at the other extreme.
Normal Bone Acquisition in Children and Adolescents
Mechanical loading during sporting activities increases bone formation and causes site-specific increases in BMD, depending on the sport. For example, gymnasts and figure skaters have increased BMD of the hip rowers, while rowers have increased BMD of the spine [10], and tennis players have increased BMD of the dominant forearm compared to the non-dominant side [11.
Assessment of Bone Health in Children and Adolescents
Areal BMD (aBMD) is calculated from BMC by dividing BMC by the projected area in the coronal plane of the scanned region. In adolescents, HR-pQCT has been successfully used to assess bone microstructure while avoiding irradiation of the active growth plate [38.
Summary
Chapter 6
Neuroendocrine Abnormalities in Female Athletes
Menstrual Variability
Characteristic findings in adolescent and young women with hypothalamic amenorrhea include hypothalamic-pituitary overactivity. It is especially essential for the vascularization and maintenance of the endometrial lining during the luteal phase of the menstrual cycle and throughout pregnancy.
Growth Hormone: Insulin-Like Growth Factor-I Axis
Amenorrheic athletes had more erratic patterns of GH secretion, which paralleled high concentrations. Both dysregulated and elevated GH release correlate with the blunted GH secretory response to acute exercise seen in amenorrheic athletes.
Hypothalamic–Pituitary–Thyroid Axis
Certainly, more studies are needed to better understand the secretory patterns of GH and IGF-I in female athletes along the spectrum of menstruation and energy availability. In other studies, exercise and energy restriction showed increases, decreases, and no changes in T4 levels.
Hypothalamic–Pituitary–Adrenal Axis
Therefore, further understanding of the interplay between energy and exercise and the hypothalamic-pituitary-thyroid axis is needed. Acute intense exercise at or above the anaerobic threshold as well as chronic endurance training have consistently shown HPA axis activation and elevated cortisol levels.
Chapter 7
Eating Disorders
Classifi cation and Diagnosis
Binge eating disorder was officially recognized in DSM-5 as its own diagnostic category of eating disorder. People with binge eating disorder may eat their fill quickly and uncomfortably, even when they are not physically hungry.
Epidemiology
For example, some young people may avoid eating solid food after a gastrointestinal illness and develop significant feeding problems [2. Further research on the reliability, validity and clinical utility is needed for all diagnostic categories [8.
Pathogenesis and Etiology
Assessment
Additional tests (urine pregnancy, luteinizing and follicle-stimulating hormone, prolactin, and estradiol) should be considered in patients who are amenorrheic or have delayed puberty. A broad differential diagnosis should always be considered for the adolescent with symptoms of an eating disorder (Table 7.5.
Medical Complications
At least one-third of all deaths in adults with anorexia nervosa are due to cardiac complications. Sinus bradycardia is present in 35-95% of adolescents with anorexia nervosa and is believed to be due to increased reported vagal tone and decreased metabolic rate.
Treatment
The use of atypical antipsychotics in adolescents with anorexia nervosa is encouraging; however, it is limited to case series and case reports. These medications have been shown to be effective in reducing anxiety and obsessive thinking in adolescents with anorexia nervosa.
Prognosis
Chapter 8
Stress Fracture
Defi nition
Although the clinical presentation is practically always pain in the affected bone, the spectrum of damage in radiographic studies can vary, depending on the modality and classification scheme, from stress reaction to stress injury, culminating in stress fracture (see table. A large study of intercollegiate athletes noted twice the incidence of stress fractures in females compared to males [7.
Risk Factors
Menstrual history has been a less consistent predictor of stress fracture in studies examining this factor. In female soldiers, the lowest adult weight is associated with stress fracture risk (but not current weight) [35.
Clinical Applicability
Chapter 9
Female Athlete Triad: Rehabilitation and Psychological Implications
Introduction to the Triad
From talking with the athlete and her parents to the doctor involved, the physical therapist is often the first line of defense when identifying athletes at risk. Armed with knowledge of risk behaviors, a coach can be the first line of defense in the development or progression of the triad.
Implication of Disordered Eating
Training
Nutrition
Nutrition and Its Effect on Bone Mineral Density
In the case of already damaged bones, bone stimulators may be provided to potentially aid in bone remodeling and healing. Although high-quality evidence does not exist for the efficacy of bone stimulators for fracture healing, there are some mixed data suggesting that an increase in healing activity may occur with the use of stimulators in slow-healing fractures [9.
Implication of Amenorrhea and Abnormal Menses
Menstruation
Further research is required to draw conclusions and make definitive recommendations of its use. Despite the increase in bone mass found with weight-bearing exercise, the consistent underexposure to estrogen outweighs any possible benefits.
Implications of Low Bone Density
Complicating matters are endurance cyclist athletes; who, according to longitudinal studies, lose bone mass during their training season [14.
Physical Therapy and Its Role in Managing Triad Related Injuries
Other modifiable risk factors include implementing appropriate training protocols according to sport requirements, using the most compatible training surfaces available, and using the most appropriate footwear for the sport. The inclusion of a nutritional counseling and a sports performance-specific education component in these prevention programs helps to identify and manage women who are at an increased risk of developing any of the components of the woman.
Psychology of Injury: The Importance of the Psychologist
Psychologist’s Role in the Management of the Triad Athlete
Pre-screening Psychosocial Questions
While these patients may experience real physical pain, psychological problems can cause or exacerbate it. In other cases, it may be undiagnosed depression or anxiety expressed somatically.
Treating Disordered Eating
Treatment Techniques for Injured Athletes
Chapter 10
Strategies to Promote Bone Health in Female Athletes
However, many athletes remained undiagnosed according to the 1992 Triad definition because they did not meet the classic Triad criteria. Such contrasting numbers suggest that the prevalence of the Triad, as defined as a spectrum disorder, is likely to be much higher than previously reported in the literature.
The most important thing to consider when seeing an athlete with a stress fracture is to make sure there is no underlying cause or any other component of the Athlete Triad. This study was limited by sample size and did not assess familiarity with the new definition of the triad of female athletes [22.
Strategies to Promote Identifi cation of Patients with Female Athlete Triad
This initial study demonstrated that there is a need to educate physicians about the triad spectrum so that they can diagnose those at risk for this disorder, discuss treatment interventions, and/or refer affected patients to the appropriate health care professionals. While the methods used to raise awareness of the triad have common themes, an individualized approach with each athlete, noting that each sport also has its own intricacies, should be used.
Developing a Multidisciplinary Team
Even more troubling, 22% of athletes participating in lean sports would not seek treatment for amenorrhea [29.
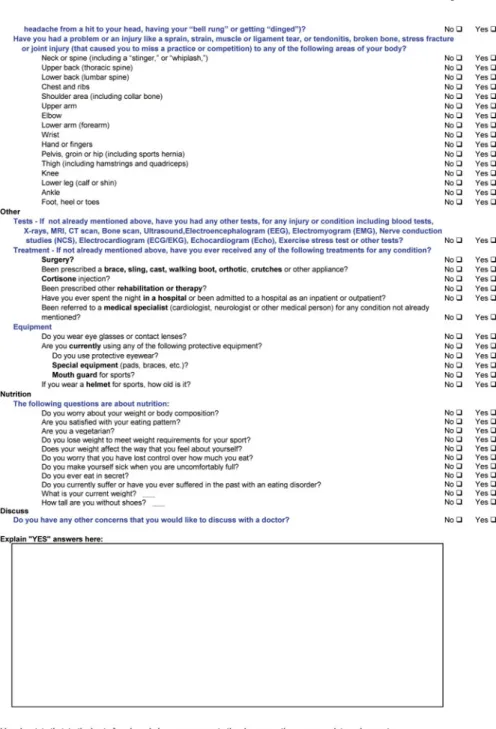
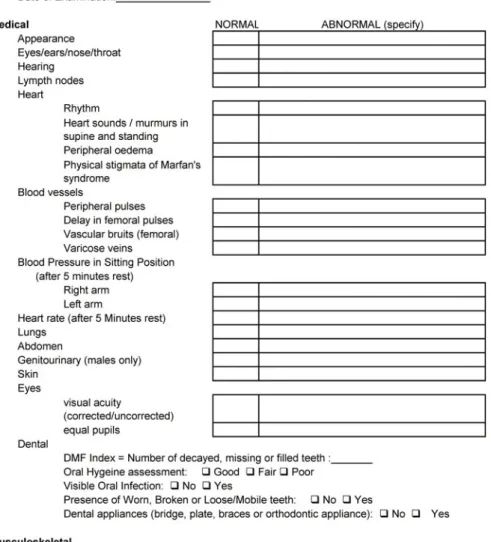
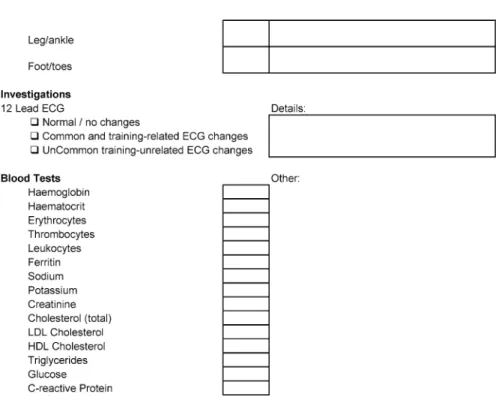
Female Athlete Triad Screening and Pre-participation Evaluation
Educate the Athletic Community
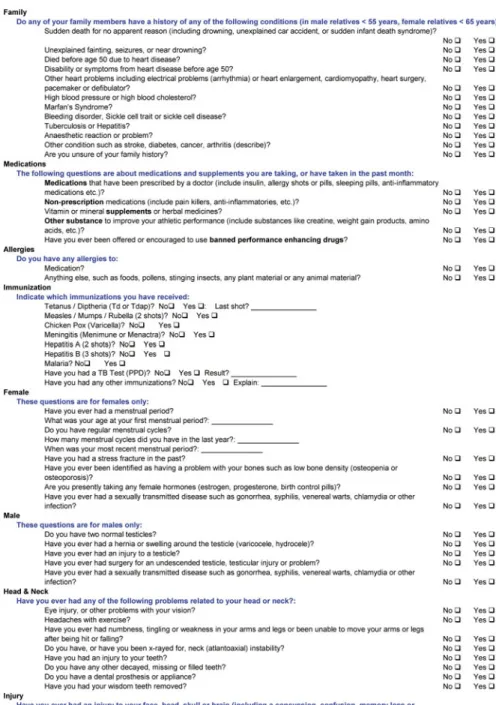
10.5 (a – e) Pre-participation assessment form recommended by the International Olympic Committee (IOC) from the 2009 IOC Consensus Statement.
Participate in Female Athlete Triad Research and Medical Education
Resources
Chapter 11
Future Directions and Research Agenda
Research will be needed to define the prevalence/incidence of RED-S compared to the traditional components of the more familiar term Triad of Athletes. Prevalence reports should include age, sport, and competitive level of the population, with the sport or group of sports classified as weight-sensitive or weight-insensitive, as appropriate.
Long-term outcome data are needed for young women and men with binge eating disorders, including the consequences of hormonal abnormalities/bone loss and adolescents with AN, and implications for peak bone mass and future risk of osteoporosis. Long-term follow-up of athletes with the Triad would help to clarify the most effective remedial approach to bone health; Long-term health outcomes including fracture data are critically needed.
Index