Data from Small Healthy Islands
IN THIS VOLUME
An application of a Tivaivai Research framework to a quantitative Pacific health research project using New Zealand’s Integrated Data Infrastructure
Understanding Parental education and health of Pacific families: Background and study protocol
Use of Bodily Tissues in Research – Pacific perspectives from Dunedin, New Zealand
Aedes Mosquito Control and Surveillance in the Pacific
Exploring success amongst Pacific families in New Zealand: Findings from the Pacific Islands Families Study
Impact of health messaging in a televised soap opera on diabetes risk knowledge: a longitudinal study conducted in Fiji
Mental health and wellbeing of Pacific students : Protocol of a Prospective cohort study
Building research capacity and capabilities in Fiji:
are we there yet?
Reflections on a Pacific regional event held in New Zealand: exploring best practice for serving Pacific communities
Pasifika Medical Association Conference Proceedings
05 02
ISSN 2422-8656
lata e tama kō ke nofo i Niu Sila, ai lata moe motu nei ha tautolu (Niuean)
that child should stay in New Zealand, she’s not used to our island
Contents
VOLUME 21, ISSUE 5, FEBRUARY 2020 EDITORIAL Page Number Pacific people’s health: migrant populations, in-country populations, and 204-205 appropriating the research to study themDonald WILSON
ORIGINAL RESEARCH
An Application of a Tivaivai Research framework to a quantitative Pacific 206-215 health research project using New Zealand’s Integrated Data Infrastructure
Jesse KOKAUA, Seini JENSEN, Troy RUHE, Justine CAMP, Wilmason JENSEN, Debbie SORENSEN,Albany LUCAS, Rosalina RICHARDS.
Exploring success amongst Pacific families in New Zealand: Findings from 216-225 the Pacific Islands Families Study
El-Shadan TAUTOLO,Julienne FALETAU, Leon IUSITINI, Janis PATE
Aedes mosquito control and surveillance in the Pacific 226-232 Lydia ANDERSON, Faafetai SOPOAGA, Susan JACK
Understanding parental education and health of Pacific families: 233-244 background and study protocol
Jesse KOKAUA, Seini JENSEN, Reremoana THEODORE, Debbie SORENSEN, Wilmason JENSEN, Rick AUDAS, Rosalina RICHARDS
Use of bodily tissues in research – Pacific perspectives from Dunedin, 245-252 New Zealand
Olivia THOMPSON, Jon ANDERSON, Margaret CHEN, Grace HAACK,Robert MANE, Tessa STEWART, James STRICKLAND, Jeremy WALTHERT, Sarah JUTEL,
Talai MAPUSUA,Daryl SCHWENKE, Fa’afetai SOPOAGA,Simon WALKER, Rosalina RICHARDS
Impact of health messaging in a televised soap opera on diabetes risk 253-264 knowledge: a longitudinal study conducted in Fiji
Jyoti MUDALIAR, Anne BECKER, Margaret GERBASI,Judith MCCOOL
Building research capacity and capabilities in Fiji 267-271 Jyotishna MUDALIAR,Bridget KOOL, Janice NATASHA,Judith MCCOOL
SYSTEMATIC REVIEW
Mental health and wellbeing of Pacific students: protocol of a 272-280 prospective cohort study
Faafetai SOPOAGA PERSPECTIVE
Reflections on a Pacific regional event held in New Zealand: exploring 281-287 best practice for serving Pacific communities
Sarah JUTEL, Bradley WATSON, Faafetai SOPOAGA
Pasifika Medical Association 23rd Conference Niue 24 – 26 September 2019 288-301 ORBITUARY
Celebration of a Samoan Odyssey – Papali’i Dr Semisi Maiai 302-303
About the Pacific Health Dialog 304-305
Cover picture: Selected pictures from the Pasifika Medical Association Conference on Niue Island 2019.
204
EDITORIAL OPEN ACCESS Pacific people’s health: migrant populations, in-country populations, and appropriating the research to study them
Donald WILSON
Head of School & Associate Professor Epidemiology & Biostatistics, School of Public Health & Primary Care, College of Medicine, Nursing & Health Sciences, Fiji National University. [email protected]
The 13th Pacific Health Ministers Meeting (PHMM) that was held in Tahiti in August 2019, acknowledged, among several important decisions, that strengthening primary health care should prioritize effective mechanisms for addressing noncommunicable diseases (NCDs) health security, and building climate-resilient health systems, communities and infrastructure.
It also acknowledged the high burden of obesity and the ongoing NCD crisis in the Pacific and the need to ensure that support is available for countries to strengthen NCD-related policy and legislation. 1
For the Pacific region, the millennium ushered in global changes that among other effects, altered its landscape, land, its people, their diet and daily habits. Two decades in, and the Pacific is in a crisis due to Non-Communicable Diseases (NCDs), the leading cause of deaths in the region.
In New Zealand, the life expectancy of Pacific peoples is about four years less than that of the general population. Pacific peoples' health is worse than other New Zealanders’, from childhood through to the later stages of life. New Zealand children have poorer health compared with those in other developed countries such as those of Europe, with higher rates of hospitalization for serious infectious and respiratory diseases, rates of acute rheumatic fever (ARF) and meningococcal disease.
Additionally, many hospital admissions are potentially avoidable, and could be prevented through primary health-care interventions and improvement in household conditions. 2
In order for the health of Pacific peoples to be accurately measured, it would be ideal if the measurement tools or research frameworks could compare populations within the Pacific Island Countries (PIC’s) and relevant migrant populations in “destination countries”, particularly in New Zealand and Australia. Such research undertakings need to be contextual and population-sensitive.
Health issues of migrant populations influence health systems variably, dependent on factors that include the adopted continent or country, its national economic status versus that of the immigrant, and differences in language, climate, and food. While such challenges are largely overcome with time, some migrant populations struggle with the same, or even worse health problems over time. The set-up of national systems in these adopted countries are an important. In Europe, the 35 to 40 million foreign-born people continue to face difficulties in becoming a full part of the economic, cultural, social, and political lives of their adopted societies. The right to health obliges governments to ensure that “health facilities, goods and services are accessible to all, especially the most vulnerable or marginalized sections of the population, in law and in fact, without discrimination on any of the prohibited grounds.” 3
Research papers appearing in this issue of the Pacific Health Dialog importantly focus on a number of health issues, education and health promotion frameworks in Pacific populations in the PIC’s, and in Pacific peoples in New Zealand.
A couple of papers have attempted to address the gap in study designs contextualized for the Pacific and its peoples.
In a study of immigrant populations in Belgium, Lorant et al, 4 investigated the association of contextual factors with disparities in self-rated health between native and immigrant groups.
They found that two particular immigrant groups were more likely to have poorer self-rated health, than native-born Belgians. The presence of various environmental factors in the “original and adopted” countries necessarily need to be adjusted for when in statistical models to measure overall health effects. Contextualizing all our health research in the Pacific is therefore important for the accurate measurement of health status of our Pacific peoples.
205 The Health Research Council of New Zealand
(HRCNZ) published the Guidelines on Pacific Health Research in 2007 to assist researchers to undertake health research with Pacific people. 5 While it describes points of difference between Palangi and Pacific perspectives, it highlights the fundamental role of relationships. To underpin this central theme, ten principles are described as essential to guiding ethical research relationships. These are respect, cultural competency, meaningful engagement, reciprocity, utility, rights, balance, protection, capacity building, and participation.
Research is the scientific undertaking required to appropriately address the health concerns of Pacific Health Ministers for their sovereign populations and peoples, as described in the 2019 PHMM outcomes document, 1 but it is equally important that the scientific community pay due heed to contextual ethical considerations.
REFERENCES:
1. Outcome of the 13th Pacific Health Ministers Meeting, Tahiti, French Polynesia 6-8 August 2019. WHO 2019. CC BY-NC-SA 3.0 IGO licence. Last accessed 11 Nov 2019.
2. Statistics New Zealand and Ministry of Pacific Island Affairs. Health and Pacific peoples in New Zealand. Wellington: Statistics New Zealand and Ministry of Pacific Island Affairs.
2011. Last accessed 11 Nov 2019
3. Rechel B, Mladovsky P, Devillé W, Rijks B, Petrova-Benedict R, McKee M. (eds).
Migration and Health in the European Union, European Commission, Open University Press 2011
4. Lorant V, Van Oven H, Thomas I. Contextual factors and immigrants’ health status: Double jeopardy. Health and Place; 2008; 14(4), 678- 692
5. Guidelines on Pacific Health Research, Health Research Council of New Zealand 2007. ISBN 0-908700-19-9
Original Research OPEN ACCESS An application of a Tivaivai Research framework to a quantitative Pacific health research project using New Zealand’s Integrated Data Infrastructure
Jesse KOKAUA,1 Seini JENSEN,2 Troy RUHE,3 Justine CAMP,4 Wilmason JENSEN,5 Debbie SORENSEN,6 Albany LUCAS,7 Rosalina RICHARDS,8
ABSTRACT
Using the Integrated Data Infrastructure (IDI) to investigate or research various social, cultural, health, or other related outcomes is appealing and has a lot of potential. The IDI offers sufficient numbers for researchers to investigate outcomes in Pacific communities to a level of detail not available in many studies. The overall aim of this paper is discuss the appropriate values for research projects involving Pacific communities using IDI data; issues around ownership of data from Pacific communities; consent;
identification; and other ethical considerations.
Although the IDI has a great deal of potential for Pacific health research, many findings based on research using IDI data have been recognised as deficit-framed and polarising for the communities they describe. Some would argue that such findings highlight discrepancies in health or social equity and point to deficiencies that should be the responsibility of governmental organisations. Most analyses stop short of investigating practical pathways for communities to find solutions that are sympathetic to the values or established infrastructure of those communities.
This paper proposes an extension to the Tivaivai/Tivaevae research framework and shows how it incorporates values that should be reflected in Pacific research using IDI data. With applications in a range of disciplines,the Tivaivai framework, like many Pacific research models, has been applied to qualitative or small mixed-methods projects, and restricted to Cook Islands research. The paper describes an outline of values that will underpin a specific Pacific health research project and presents a framework for how to incorporate those principles into that study. It is hoped, that this paper may provide a starting point for other quantitative Pacific research projects involving administrative or other big data. Further, it also provides a blueprint for any study, Pacific or otherwise, to be explicit about the values principles and connection they wish to uphold for the communities that are the focus of their research
Key words: Pacific, Health, Population data, Integrated data, Research
INTRODUCTION
Pacific community context in NZ
New Zealand is home to a significant Pacific population, now forming 8% of the total population. As a fast-growing and youthful population, they are projected to reach 590,100 (10.2%) by 2038.5 This population is diverse, with the term ‘Pacific peoples’ encompassing more than 20 different nations, each with their own history, languages and customs.6 Migration from Pacific nations to New Zealand was and continues to be underpinned by the desire for expanded opportunities in employment and education. A significant wave of migration took
place in the 1950s-60s to support the strong economic growth present in NZ at the time. 7
Corresponding author: Jesse Kokaua, [email protected];
1. Research Fellow, Centre for Pacific Health, Va’a O Tautai, Division of Health Sciences, University of Otago, Dunedin, New Zealand
2. Director of Performance & Evaluation, Pasifika Futures Limited, Auckland, New Zealand,
3. PHD Student, Division of Sciences, University of Otago, Dunedin, New Zealand.
4. 4. Research Fellow, Centre for Pacific Health, Va’a O Tautai, Division of Health Sciences, University of Otago, Dunedin, New Zealand.
5. Deputy Chief Executive, Pasifika Futures Limited, Auckland, New Zealand,
6. Chief Executive Officer, Pasifika Futures Limited, Auckland, New Zealand,
7. Assistant Research Fellow, Centre for Pacific Health, Va’a O Tautai, Division of Health Sciences, University of Otago, Dunedin, New Zealand.
8. Director, Centre for Pacific Health, Va’a O Tautai, Division of Health Sciences, University of Otago, Dunedin, New Zealand.
Rec: 06.06.2019 Acc: 08.11.2019 Pub: 30.01.2020 Citation: Kokaua J, et al.. Pacific Health Dialog 2020;
21(5):206-215. DOI: 10.26635/phd.2020.621
Copyright: © 2020 Kokaua J, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
However, a subsequent economic downturn in the 1970s increased pressures on Pacific communities, who were negotiating the context of increased unemployment, and other social difficulties.
Settlement in New Zealand accompanied mixed messages of a demand to adopt the anglicised culture and experiences by many recently arrive Pacific peoples of entrenched insidious social racism. Though not made explicit, its intent was to undermine the cultural values and practices of non-English speaking cultures in New Zealand to enable those peoples assimilation to New Zealand society. However, as with many non- Palagi communities, Pacific peoples were an easy social group to target.
The negative political framing of Pacific peoples in the late 1970’s, under the guise of policing illegal immigrants, affected all Pacific communities. In spite of that history, Pacific communities emerged as vibrant contributors to contemporary Aotearoa. However, the residual effects remain from past alienation, with subsequent barriers to health, education, employment and other services intended to meet their needs.
In the present day, the cumulative impact from many negative changes is observable in health inequities between Pacific peoples and other New Zealand communities. This includes lower life expectancy, quality of life, and higher rates of key morbidities. 8,9 The New Zealand health sector is responding to this inequity with efforts to increase the Pacific health professional workforce, 10,11 raise cultural competency among health professionals in mainstream health systems, 12-14 as well as the development of Pacific-specific health services. 15
Integrated Data Infrastructure and Pacific health
The Integrated Data Infrastructure (IDI) is a population dataset for New Zealand that incorporates national data collected from many government agencies, Census, several national surveys, and some non-government organisations.16 Foremost, it allows us to potentially combine data from several government agencies. Additional data can also be uploaded into the IDI to enhance their information capabilities by appending data held by an external agency to data from government agencies. The data made available is limited to the sets of data specifically requested by each project application submitted to utilise IDI data.
There is support material for all tables contained in the IDI available through links from the IDI website. Finally, there are strict protocol and approval processes for IDI data access, analyses, and release.16
For Pacific research purposes the IDI is an immensely useful set of data with a great deal of potential for Pacific health research, but many interpretations of IDI data have been recognised as deficit-framed and polarising. That is, findings that highlight discrepancies in health or social equity and point to deficiencies that should be the responsibility of governmental organisations. Such framing of analyses tend to stop short of investigating practical pathways for communities to find solutions that are sympathetic to the values or established infrastructure of those communities. Instead, most are left with the realisation of deficit and often a feeling of indictment.
Pacific peoples, Pasifika, Tangata O Te Moana Nui a Kiva, are the descendants of expert navigators who explored and populated the vast Pacific Ocean. Experienced way-finders voyaged for adventure and to acquire community resources.
Success rested on their ability to synthesise information from a vast range of complementary sources, including the constellations, weather patterns and ocean currents.17 Developing those skills required experiences from many lifetimes and each voyage was laden with risks that had to be managed. It is with this attitude of innovation, discovery and vigilance that we have to approach the area of integrated administration data, one of many types of resources included in the term ‘Big data’. As will be explained, this is a powerful and influential tool, and it is important to explore how Pacific peoples in Aotearoa New Zealand (NZ) might position ourselves at the forefront of the big data wave and benefit from its momentum.
Aims of this paper
The purpose of this paper is to discuss established Pacific Research values that should underpin any research into Pacific health using data in the IDI. It is hoped that this will provide a useful information base for other Pacific researchers looking to work with the IDI and stimulate discussion about opportunities and challenges in this space.
Pacific research frameworks and values This paper is the result of a review of published New Zealand and Pacific research frameworks. It incorporates the values, data principles and approaches common to Pacific and Maori reseach in New Zealand. The composition of a tivaivai/tivaevae, a trditional quilt, has been chosen as the metaphor for a research framework that has been developed for several modes of Cook Islands research. In this instance a Tivaivai research framework will be adapted to provide a process model of how Pacific values might be adopted in a large quantitative study.
Where referring to the Tivaivai framework and the values incorporated, Cook Islands Māori (Mauke)1 terms have been used wherever possible. Where appropriate, other languages have also been used. Though not exhaustive, lessons and values reported in this paper will provide a platform to support and develop the study protocol for a project that includes the IDI.4 Pacific Health Research values
Within the health research context there has also been an investment in the Pacific workforce, with dedicated Pacific post-graduate scholarships and post-doctoral fellowships.18 Alongside this, guidelines have been developed to support non- Pacific researchers conduct research safely with Pacific communities and encourage partnership and capacity development in research which is of relevance and import to Pacific communities.19,20 Key in this space are guidelines from the Health Research Council, the major funder of NZ health research.19 These guidelines describe key values, themes and processes for Pacific research.
The HRC Pacific research guidelines provide extensive discussion of mechanisms to ensure that research involving Pacific participants is as appropriate and impactful as possible. Given the newness of the IDI space it is useful to reflect on
1 In appreciation of the work contributed by one of the co-authors the Mauke dialect has been adopted.
Where referring to other material often Rarotongan terms may be referred to. Thus, for example, Tivaivai
such issues. The focus in this paper will be the four key themes identified in the HRC guidlines:
uriuri kite (Recipocity), Ora katoatoa’anga (Holism), tu akangateitei (Respect) and tu inangaro (Communal relationships).
Akangateitei (Respect) - Research with Pacific peoples needs to uphold the dignity and aspirations of Pacific communities and acknowledge the significance of Pacific peoples’
traditional and emerging cultural practices, knowledge and experiences. The IDI contains large amounts of highly sensitive information.
Respectful research practice should be:
a. Akaari kite Understanding the communities of interest, which comes about through connectedness and developing a relationship with each community. To increase the likelihood that findings and stories that emerge from the analysis give due regard, and are generous to, their world views. Ensuring sensitivity to what each holds as important messages or as Tapu. The latter does not necessarily equate to forbidden but should be handled with care and discretion.
b. Non-deficit framed,
consultation/governance in absence of consent, research should be Pacific- advised and, if possible, Pacific-led. It must be conceded that much of the IDI data is collected under circumstances that amount to coercion, whether implied or direct, and in many cases is reflective of negative events. It therefore adds to the responsibility of researchers to treat that data and the ensuing findings with respect as it is used outside the purpose for which it was gathered.
c. Administrative data is captured by and reflective of a wider system that does not reflect the customs or values of Pacific. If not blatantly counter to, then ignorant of them. It becomes imperative that any analysis involving Māori or Pacific begin with that consideration.
Inangaro (Collective relationships)- Health is the responsibility of the entire community, with communal relationships needing to be considered alongside individual relationships and rights. The IDI measures are linked at the level of the individual, however, it is possible to link and combine to ascertain the health of family collectives, or of ethnicity-specific communities is from the dialects of many of the Cook Islands is often used interchangeably with Tivaevae, predominantly from Rarotonga.
within NZ, which smaller studies are not able to do.
Uriuri kite (Reciprocity) - Returning to the community that which has been taken out for research purposes. In the IDI, Pacific communities have already contributed, and, often without direct consent for involvement.
This means that within the IDI space the balance is firmly pushed towards researchers needing to reciprocate with thoughtful, high quality research which is aligned with Pacific priorities and aspirations. Ideally, this would include research that supports health gains, building Pacific research capacity, and dissemination and education with a plan of action to mitigate the issues that are important for Pacific communities.
Ora katoatoa’anga (Holism) – Now an established principle, beyond Māori and Pacific communities, health is the result of an interaction between wellbeing in multiple domains. It considers shared relationships between: Kopu tangata/ family and social relationships; Aorangi/environment;
Vaerua/spiritual and cosmology; Kopapa /physical; and Tu manako /mental health.17 The breadth of measures needed to encompass all of these areas are a challenge for research, especially in large scale population studies. One of the strengths of the IDI is its ability to link information from a wide variety of areas, bringing together health, education, justice, and census data, providing as diverse a view of people’s lives as possible. Despite this breadth there remains a significant risk of decontextualisation, with the data being collected for administrative purposes rather than to specifically understand the complexities of particular areas.
Responsiveness to Māori. Relationship via Te Moana nui a kiva.
Given the unique status Māori hold in Aotearoa and our shared heritage and historical relationship via Te Moana nui a kiva, Pacific research in NZ needs to uphold the mana and aspirations of Māori. It is essential that in any research proposal, especially in the application for funding and ethics approval that we as Pacific understand our connection to Maori of Aotearoa and their position in NZ research. These guidelines are framed to ensure that research produced from the use of data about Māori from the IDI is cognisant of the fact that the findings are an extension of Māori who contributed to the data. They represent a taonga as required by article two of the Treaty of Waitangi;21 because they help explain who we are as a people, in terms of behaviour, beliefs and values; because
they highlight our past, present and future;22 and because the outcomes can help us to determine our health and well-being. The language is reo Māori, but the values espoused are analogous to those aspired to by Pacific peoples in Aotearoa.
In all but sovereignty, a right to which Māori have greater access than other citizens in Aotearoa, these are shared by the Pacific principles espoused above.
Pāpahi – It is important that Māori have input into the data collection and use where information about Māori are gathered. Making sure that Māori are participating in all aspects of big data design and collections, and having a say in how can we work in partnership to use big data will complement and improve research outcomes.
Kia whakamana – This is the acknowledgement that the data, even though it is anonymous, remains an extension of who we are as a people.
This acknowledgement dictates that we use the data in a way that enhances and uplifts Māori.
Kia pono - Typically pono is used to mean truth.
In this context, researchers need to understand and disclose the subtle biases that are inherent the system. When presenting findings from the IDI, researchers need to provide the appropriate context around the measures used and any systemic bias in the data collected.
Kia tika – An avoidance of deficit research, so that the research findings, whether positive or negative, are presented with a purpose to promote wellness outcomes and disrupt illness trends. As with Pacific, overall research questions and methodologies should be developed in a way that Māori are not continuously being presented in a negative spotlight.
Ko te reo tika – When undertaking research where Māori are included, it is important to not apportion blame, whether direct or implied, for the predicaments that study participants experience. Wherever possible, this should be done using Māori methods reflected in the research design and at the very least include Māori as a crucial part of any research team.
Kia wero – The potential of the IDI can be further enhanced by including Māori measures of wellness and success to present analyses and a research framework that challenge the status quo. In that context, there are vast opportunities to work with Iwi to better the outcomes for Māori using the data contained in the IDI.
Pacific frameworks for quantitative research Conventional research in the IDI follow an informal process of: pulling together a
multidisciplinary team for the project with a stated aim or thesis; develop a peer reviewed study protocol; submit an application to the Health and Disability Ethics Council (HDEC) for ethical approval; make an application for microdata access; undergo security clearance procedures before using the IDI lab; undertake the numerical analyses inside the datalab; submit those results to SNZ for clearance; complete any analyses and discussion of findings within the team members; write up and make a final submission, report or publication. The ultimate outcome being the peer-reviewed publication.
For Pacific researchers the ultimate goal is to make a contribution to the improvement of Pacific communal wellbeing. One way in which communal wellbeing can be improved is through a clear understanding and privileging of said communities’ worldviews, which is the central component to Pacific research methodologies. To ensure this, studies that undertake Pacific research using IDI data, if not lead by a Pacific researcher, should include a substantial contribution from Pacific researchers at all levels from the studies outset. It is essential, for reasons that will explained subsequently, that those researchers are able to connect with the Pacific communities that are the focus of the research.
In terms of Pacific approaches to research there are several established and validated processes that are established for and by Pacific researchers, to which the above quantitative process is not entirely alien. One well-known Pacific research framework that fits well is the Kakala research framework23 to which the IDI process outlined above shares some similarities.
The latter has some important shortcomings that make it fall very short of fitting comfortably in the Pacific space. These are where IDI and general quantitative research can learn from Pacific models for health research.
For a quantitative analogy of the research process we have chosen to use the existing Tivaivai (or Tivaevae, the Cook Islands patterned quilt) research framework.1-3 The Tivaivai is a popular Cook Islands, therefore Pacific Islands, art-form. The Tivaivai research framework has been adapted to include six steps: Te Oroma (insight or vision; to prepare, plan), Ko’iko’i (gather; the process of data collection), Atuitui (stitch the pieces together; to analyse the data), Mareka’anga (appreciation of the gift; gain feedback) and Ariki’anga, (the acceptance of the workmanship by the community). Orongo‘anga (present as a gift; future implications for the findings).
DISCUSSION - USING THE IDI FOR PACIFIC HEALTH RESEARCH
Translating Pacific values to IDI research The Tivaivai research model includes six steps:
Te Oroma (to prepare and plan from the vision of the outcome); Ko’iko’I (the process of data collection); Atuitui (the analysis stage);
Mareka’anga (verification or feedback loop); and Ariki’anga (the acceptance of the findings); and
‘Orongo ‘anga (dissemination and establishment of tangible application of the findings in a positive solution for Pacific communities).
Importantly, while there are six phases presented in a linear sequence, the concepts of Mareka’anga and Ariki’anga should underpin each of the other stages in the research process.
It is with these two principles that we reinforce our relationships with the Pacific community and ensure their aspirations are realised. By serving as a checkpoint at each of the other stages, we endeavour to obtain consensus with community values before progressing to the next stage.
Te Oroma
Te Oroma is the vision of the outcome and possible pathways to a positive outcome for the entire community. This vision is what provides the scope of preparation for the establishment of core research questions or hypotheses, background research and literature review, which is consistent in qualitative and quantitative research. A traditional Tivaivai design would be designed by ta’unga, a holder of the knowledge or gift for that purpose, both technical and cultural. So the responsibility of the project leader is to be skillful in both knowledge of the topic and the community in focus. A research team, investigating Pacific health, should ideally be led by a person of Pacific descent and/or with strong links to the Pacific community. Otherwise it would be essential to have other sources of strong Pacific community input into Te Oroma. It will often involve pulling together a multidisciplinary team, however, it requires genuine Pacific community engagement that must extend beyond the inclusion of a single Pacific voice on a research team.
It is important that the value of Respect is incorporated from this stage to ensure that the aspirations and values of Pacific communities are considered prior to undertaking the research.
Holism: a part of that respect is to accept a view of health that is holistic, beyond a simple one- dimensional aspect of a persons and families’
wellbeing, and accepts that outcomes of health can be reflected at multiple levels. Thus, it is also important to consider Pacific and Māori measures of wellness (kai wero).
It is at this stage that communal relationships are an important consideration remembering that health is the responsibility of the entire community, with communal relationships needing to be considered alongside individual relationships and rights. Before the ultimate reporting of findings, Pacific researchers will be considered accountable to their communities and a relationship should be established at this stage to reinforce the values that the team will uphold and ultimately reflect.
Ko’iko’i
Ko’iko’i is the process of collecting data and encompasses the various tools and methods of collection such as Talanoa, Uipa’anga (meetings) or iriiri kapua (brainstorming) and other methods that are appropriate to the culture in focus. The data in the IDI is already gathered and while it would appear to be straight-forward, it requires much attention to its detail to be sure that you have captured the appropriate data.
Respect, holism and communal relationships follow through to the collation of the data and consideration of the construction of the indicators used and created for the intended analyses. In the IDI in particular it is important to understand, as much as possible, the caveats around the datasets that are considered for use and the context in which the data is gathered, bearing in mind the data is captured by and reflective of a wider system that does not reflect the customs or values of Pacific. Consideration of the potential implications, negative and positive needs to be given for each community in focus (kia pono). Such is the importance of such values as Kia whakamana, an acknowledgement that the data is an extension of the collective communities and, as such, its use should seek to enhance and uplift those communities.
Ultimately, Reciprocity, returning to the community the gift of knowledge that we as researchers have been afforded, should be the aim even if that goal is not attained for any number of reasons.
Atuitui
The analysis phase which in the IDI requires the use of statistical methods and is less demanding than the unbundling of themes from in depth discussions with the Pacific communities. This stage will establish the evidence to support or refute the initial research hypotheses. Findings should be presented in a way that upholds Respect for those communities. Firstly, researchers owe it to their communities to undertake quantitative research to the highest possible academic standard. This undertaking requires not only understanding academic
processes but how their study will translate to a Pacific community, made easier through connectedness and relationship developed between the team and each community so that findings are utilised with integrity. Thus, being mindful and enabling the opportunity for negotiation of sensitivities that exist between and within communities.
Mareka’anga
Mareka’anga gives key voices within the Pacific community the opportunity to consider and assess the craftsmanship to that point in time.
This step is required to gain feedback about key Pacific findings from Pacific communities and to discuss an appropriate response that is acknowledged by and implementable by those communities. It is made difficult for IDI researchers as conventional dissemination is through academic journal publications, conference proceedings or government reports.
This process provides a useful feedback loop where the researchers are able to acknowledge the response from the communities as a validation of those findings and their implications. This is where a team will be tested in terms of its affording Respect and inclusion of the Pacific communities that are the focus of the study.
Ariki’anga
This is a consequence of gaining input into interpretation from those communities and developing appropriate responses to challenges arising from the findings. At which point any resultant publication is made stronger by carrying with it the voice of the communities that are in focus.
This step represents the ultimate act of Reciprocity - returning to the community that which is given or taken and used for research purposes. Undertaking research that supports health gains, building Pacific research capacity, and dissemination and education around issues which are important for Pacific communities.
Ariki’anga represents findings that have successfully been accepted by Pacific communities and approaches to making positive changes are agreed upon and adopted.
Orongo ‘anga
Orongo’anga is the process of gifting the Tivaivai and represents the future applications of its use.
At this point, traditional IDI research would consist of an internal discussion of findings and if recognised of any novel research value the team may consider publication in a reputable journal.
A process that does not sit easily with the collective values of Pacific communities and one
Models Values Outputs
Tivaivai/
Tivaevae Kakala Description
Collaboration Respect Reciprocity Relationships Shared vision Holism Data integrity Development Context
Conventional Research Community
Te Oroma/
Akapapa Teu Preparation
To prepare and set
up a defined plan ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓
Establish research question and gather specialists
• Background and investigative research
• Clear study protocol
• Sound methodological framework
Gather specialist knowledge
• Team incorporates Pacific community perspectives and
leadership
• Team seeks to build Pacific research capacity
Koikoi /
Akaruru Toli
Cutting the pattern:
To gather necessary resources
✓ ✓ ✓ ✓ ✓ ✓
The data collection
• IDI data is already collated,
• Indicator definitions need to be clear and robust
• Quality needs to be assured
The data collection
• Variables should be included to reflect and support Pacific values as much as possible Pakoti/
Atuitui/
Tuitui Tui Stitch the pattern To bring the
pieces together ✓ ✓ ✓ ✓ ✓
Data analysis
• Ensure that appropriate statistical tools an analysis
techniques employed
Data analysis
• Findings reported with a mind to Pacific values
Mareka’anga Malie Appreciation
(Of a gift) ✓ ✓ Verification of key findings
• Verification of the accuracy of key findings
Considerations of key findings
• Consider key findings mindful of implications of naïve inferences upon Pacific
communities
Ariki’anga Mafana Acceptance (Of fine
workmanship) ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓ Submitted work
• Findings submitted for peer review in appropriate journals
Obtain Community Solutions
• Key findings shared with sectors of the Pacific community to discuss
solutions Orongo’anga/
O’ora te tivaevae/
akairianga
Luva Presentation
To present the gift ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓
Academic dissemination
• Findings published in peer reviewed journals and presented at academic fora
Present final output
• Findings can be presented with Pacific solutions,
asserting our Pacific Community as a priority
that has some learning to take from the Kakala model.The remaining stages could require more resources than many quantitative studies would currently allocate as they involve establishing or having an established relationship with the communities involved, whether Pacific or not.
Note that, by default, there is already an established relationship with the prevailing culture.
‘Orongo ‘anga is where the team, community and researchers, considers the key findings and their implications for the community. In IDI research this is an internal process as there are no participants to feed back to and feeding back to communities is not possible for preliminary findings. Thus, it becomes imperative that the initial research team includes quality input from Pacific researchers to establish connections with Pacific communities at this end of the process.
Firstly, non-deficit framed, Kia tika, the framed deficit does not exclude reporting negative findings, but that those findings are presented in a way that does not apportion blame, ko te reo tika, and goes further to offer a solution to that negative outcome that is consistent with the practices in each community. It must be conceded that much of the IDI data is collected under circumstances that amount to coercion, whether implied or directed and in many cases is reflective of negative events. It therefore adds to the responsibility of researchers to treat that data and the ensuing findings with respect as it is used outside the purpose for which it was gathered.
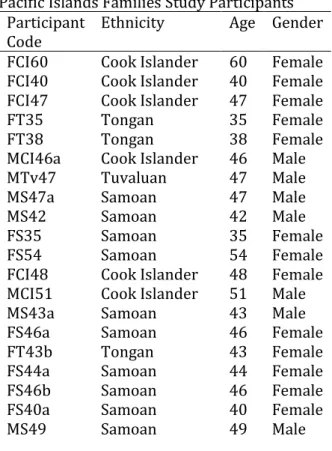
One example of a quantitative study where these phases come close to being practiced, while not formally using this framework, is from the Pacific Islands families(PIF) study.24 Perhaps true of most longitudinal studies, both are able to establish long term relationships with participants that enable practices similar to Orongo’anga, Mareka’anga, and Ariki'anga.
Another common approach in Pacific research, is for the IDI analysis to contribute to a mixed-methods approach, where the quantitative analysis is augmented by a more refined qualitative study to further contextualise the findings and vice versa. As long as that qualitative process employed a Kakala, or similar, methodology then the last two phases would automatically be incorporated.
Shortcomings of the IDI in terms of Pacific values
Very few studies exist that allow for such a granular analysis of Pacific families that allows such ethnic detail in New Zealand, the PIF study is one such example. The IDI allows for that level of granular detail at a population level as well as enabling comparisons with other groups. However, the former has an enormous amount of contextual and cultural detail not available in the IDI.
The nature of the data is predominantly deficit-based, capturing events that are often negative under circumstances that can be perceived as coercion by the recipient. For example, instances of poor health, engagement with justice and social services.
Educational achievement and income are potential exceptions, however, a focus on recidivist truancy at school or a focus upon poverty show that a deficit framing is not the sole fault of the data.
However, there are issues around the need for better data quality, understanding the appropriateness of current measures for Pacific communities and, refining or adding new measures that incorporate a Pacific worldview. The data is not only captured under extenuating circumstances, the indicators are not created to measure positive outcomes let alone reflect positive Pacific values.
Many studies, in spite of the best intentions of the research teams, prioritise academic principles and interests above community values. That means that initial hypotheses are not determined by Pacific interests but by previous published findings to see if those are reflected in the Pacific context. Not a poor idea, however, it reinforces the perceptions inherited from those findings in those studies as often only the worst instances are presented and there are few instances of Pacific communities as examples for good health.
CONCLUSIONS
The IDI is a valuable research platform for Pacific communities to identify many health priorities and plan service responses for their people. Its use can provide Pacific communities with valuable insights into health outcomes that, when framed in an appropriate manner, will add to the growing
pool of health research about Pacific communities. Pacific researchers should not consider the IDI as anything other than another source of potentially useful data that may contribute to the growing the Pacific Health knowledge base. It therefore becomes imperative that we as Pacific health researchers have a greater presence in that research space to ensure Pacific communities get to share their own stories using that data.
This paper has provided an outline of values that will underpin our Pacific health research project and presents a framework for how we aim to incorporate those principles. These are to be applied in a project that will be undertaken by this team and is described in a separate paper.3 It is hoped, that this paper may provide a starting point for other quantitative Pacific research projects involving administrative or other big data.
Further, it also provides a blueprint for any study, Pacific or otherwise, to be explicit about the values principles and connection they wish to uphold for the communities that are the focus of their research.
Statistics New Zealand Disclaimer
The opinions, findings, recommendations, and conclusions expressed in this paper are those of the author(s), not Statistics NZ, or The University of Otago. Access to the anonymised data used in this study was provided by Statistics NZ under the security and confidentiality provisions of the Statistics Act 1975. Only people authorised by the Statistics Act 1975 are allowed to see data about a particular person, household, business, or organisation, and the results in this paper have been confidentialised to protect these groups from identification and to keep their data safe. Careful consideration has been given to the privacy, security, and confidentiality issues associated with using administrative and survey data in the IDI.
Further detail can be found in the Privacy impact assessment for the Integrated Data Infrastructure available from www.stats.govt.nz.
Funding Acknowledgements: JK is supported by a Health Research Council Pacific Post-Doctoral Fellowship (#17/466) and is partly employed by Pasifika Futures Limited. SJ, WJ and DS are employees of Pasifika Medical Association Group. JC and RR were employed by the Better Start Science Challenge: Big Data team during part of this study.
Competing interests: Pasifika Futures is the Whanau Ora Commissioning Agency for Pacific families. It is a Charitable Company as part of the Pasifika Medical Association Group Author contributions: All authors contributed to the concept and design of this study. JK authored the first draft of this paper as and all authors contributed to the revision and final draft of this paper. JC contributed Kaupapa Maori component while TR and JK contributed the Tivaivai model application.
REFERENCES
1. Futter-Puati, D., & Maua-Hodges, T., (2019). Stitching Tivaevae: a Cook Islands research method, AlterNative,
1-10, DOI:
10.1177/1177180119836788
2. Powell, E. E.N., (2013). Stitching to the back-bone: A Cook Islands literary tivaivai, Masters Thesis, The University of Auckland.
3. Ruhe, T. (2018). The Niu Movement- the effectiveness of circuit based exercise in Cook Islands communities, proceedings of the 2018 Cook Islands Health conference, Rarotonga, Cook Islands.
4. Kokaua, J., Jensen, S., Jensen, W., Sorensen, D., Audas, R., Theodore, M., Taumoepeau, M., Poulton, R., &
Richards, R., (2019). Parental Education and health for Pacific Families: background and study protocol, submitted for publication 5. Statistics New Zealand, (2018).
National ethnic population projections, by age and sex, 2013(base)-2038 update. [Retrieved from:
http://nzdotstat.stats.govt.nz/wbos/In dex.aspx?DataSetCode=TABLECODE75 60&_ga=2.58030314.1350823076.152 7556285-907393316.1501027559#
(accessed on 29 May 2018)].
6. Statistics New Zealand (2013). Pacific peoples ethnic group [Retrieved from http://www.stats.govt.nz/Census/201 3-census/profile-and-summary- reports/quickstats-
cultureidentity/pacific-peoples.aspx.
(accessed on 29 May 2018)].
7. Ministry of Health, (2012). Tupu Ola Moui 2012. Wellington, New Zealand:
Ministry of Health.
8. Statistics New Zealand, & Ministry of Pacific Island Affairs, (2011). Health and Pacific peoples in New Zealand.
Wellington, New Zealand.
9. Statistics New Zealand, & Ministry of Pacific Islands Affairs, (2010).
Education and Pacific peoples in New Zealand. Wellington, New Zealand.
10. Ministry of Health, (2014). 'Ala Mo'ui:
Pathways to Pacific Health and Wellbeing 2014–2018. Wellington:
Ministry of Health.
11. Crampton P, Weaver, N., Howard, A.
(2018) Holding a mirror to society?
Progression towards achieving better sociodemographic representation among the University of Otago’s health professional students. New Zealand Medical Journal, 131, 1476.
12. Ministry of Health (2018). Faiva ora – National Pasifika Disability Plan. 2017.
https://www.health.govt.nz/system/fi les/documents/publications/faiva- ora-2016-2021-national-pasifika- disability-plan-aug17_0.pdf (accessed 11 June 2018)
13. PHARMAC (2018). Pacific Responsiveness Strategy. 2017.
https://www.pharmac.govt.nz/assets/
pacific-responsiveness-strategy-2017- 2026.pdf (accessed 11 June 2018).
14. Medical Council of New Zealand (2018).
Best health outcomes for Pacific
Peoples. 2010.
https://www.mcnz.org.nz/assets/New s-and-Publications/Statements/Best- health-outcomes-for-Pacific-
Peoples.pdf (accessed 11 June 2018) 15. Pacific Perspectives. Primary care for
Pacific people: a Pacific and health systems approach. 2012. [retrieved from:
https://www.health.govt.nz/system/fi les/documents/publications/primary- care-pacific-people-pacific-health- systems-approach.pdf (accessed 11 June 2018)].
16. Statistics New Zealand (2017).
Integrated Data Infrastructure.
[retrieved from:
www.stats.govt.nz/browse_for_stats/s napshots-of-nz/integrated-data-
infrastructure.aspx (accessed 6 October 2017)].
17. Howe, K.R., (2006). Vaka moana – voyages of the ancestors, David Bateman Ltd, Auckland, 2006.
18. Health Research Council. (2018) Pacific
Health Research.
http://www.hrc.govt.nz/funding- opportunities/pacific-development (accessed 11 June 2018)
19. Health Research Council. (2014) Pacific Health Research Guidelines. Health Research Council. Auckland.
http://www.hrc.govt.nz/sites/default/
files/Pacific%20Health%20Research%
20Guidelines%202014.pdf (accessed 11 June 2018).
20. Anae, M., Coxon, E., Mara, D., Wendt- Samu, T., Finau, C. (2001) Pasifika education research guidelines. Ministry
of Education.
https://www.educationcounts.govt.nz /__data/assets/pdf_file/0010/7669/pa crsrch--guide.pdf (accessed 11 June 2018)
21. Hudson, M. (2017) Mana Motuhake &
Data: Māori Data Sovereignty - Directions and Challenges
22. Marsden, M. (2003). The woven universe: Selected writings of Rev. Māori Marsden.
23. Fua, S. J. (2014). Kakala research framework: A garland in celebration of a decade of rethinking education: USP Press.
24. Paterson, J., Percival, T., Schluter, P., Sundborn, G., Abbott, M., Carter, S., Cowley-Malcolm, E., Borrows, J., Gao, W., & The PIF Study Group, (2008) Cohort Profile: The Pacific Islands Families (PIF) Study. International Journal of Epidemiology 2008;37:273–
279, doi:10.1093/ije/dy
216
Original Research OPEN ACCESS Exploring success amongst Pacific families in New Zealand: findings from the Pacific Islands Families Study
El-Shadan TAUTOLO,1 Julienne FALETAU,2 Leon IUSITINI,3 Janis PATERSON,4
ABSTRACT
An overarching objective of New Zealand society is to have an equitable educational, economic, and health outcomes for all citizens, including its Pacific population. In response to these ambitions, this study explored success and what elements are necessary for Pacific families to be successful in New Zealand. Focus groups were undertaken with 29 Pacific fathers and 27 Pacific mothers aged between 35-71 years. An inductive thematic analytical approach was used to code and identify themes from the data. Pacific methodologies, including the Talanoa and Kakala frameworks, were integral in the systematic process of data analysis. Four key factors were found to represent and constitute success for Pacific families: a connection with God, practicing and embracing Pacific cultural identity, family connectedness and lastly communication. Incorporating these key facets into social service provision to enable Pacific people to lead successful, productive lives and Pacific families to function successfully.
Key words: Success, Family, Pacific Islands, Culture, Identity, Connectedness
BACKGROUND
‘Pacific people’ is an umbrella term that represents a diverse group of ethnicities, each with their own language, cultural traditions, customs and beliefs.1 They comprise approximately 7.4% of the total New Zealand (NZ) population. The Samoan group (49%) represents almost half of the total NZ Pacific population, followed by Cook Islands Māori (21%), Tongan (20%), Niuean (8%), and smaller populations from Fiji, Tuvalu, and Tokelau.1 The Pacific population is relatively youthful, with a median age of 22 years compared to 41 years for European.1 Almost two-thirds of Pacific people are born in NZ, and 37% identify with two or more ethnic groups, compared to 13% for European people.1,2
Pacific people (93%) are a highly-urbanised population group1 which has flourished in cultural pursuits such as sport and art.3,4 However, they are over-represented in terms of unemployment,5 low income,6 low educational attainment,7,8 child poverty,9 poor child health10 and inadequate housing and poor living standards.11-13 Over time, Pacific families have experienced incremental improvements in some areas including their educational status;
however it is relatively low compared to their European counterparts 8,14 nevertheless research
is needed to describe what constitutes success in their eyes for their families living in New Zealand.
Corresponding author: El-Shadan Tautolo, [email protected]
1. Assoc Prof, Auckland University of Technology (AUT) Centre for Pacific Health Research, Auckland, NZ
2. Research Assistant, AUT Pacific Islands Family Study, Auckland, NZ
3. Senior Research Officer, AUT Pacific Islands Family Study, Auckland, NZ
4. Professor, Assoc Dean, AUT South Campus, Auckland. NZ.
Rec: 23.04.2019 Acc 17.09.2019 Pub: 30.01.2020 Citation: Tautolo E, et al. Exploring success amongst Pacific families in New Zealand: Findings from the Pacific Islands Families Study. Pacific Health Dialog 2020; 21(5):216-225.
DOI: 10.26635/phd.2020.627
Copyright: © 2020 Tautolo E, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Concept of Pacific Families
Families can be based upon various foundations, such as legal relationships, biological and ethnic
217 ties and household composition.15-17 Statistics
New Zealand defines a ‘nuclear family’ as a couple, with or without child(ren) or one parent and their child(ren) who reside in the same dwelling.18 This definition has been criticised as too narrow to capture the nature of Pacific families since Pacific notions of family extend further than the nuclear family unit common in Western societies.11,19 Common Pacific concepts of the family include, ‘api (meaning ‘home’) in the Tongan language, and the Samoan notion of aiga (meaning nuclear and extended family).
Koloto and Katoanga19 define a Pacific family as one that is inclusive of at least one person of Pacific descent living in the family home and also considers the important notion of ‘proximity of contact’, meaning the physical location and closeness of immediate and extended family households as integral to Pacific ideologies of family.19,20
Wellbeing of Families
The wellbeing of families has been prioritised by various NZ government agencies.21 Family wellbeing has been pragmatically described as the ability of families to function effectively within diverse, complex, transience environments of society and can be measured holistically.22 Moreover, family wellbeing is perceived to encompass socio-economic indicators such as income, education, employment, housing, living standards and health outcomes of the family as a whole. 14,22-24 Several studies have examined wellbeing for all types of families in NZ, including Pacific households.14,22-25 Cotterell et al. 14 described differences in family wellbeing in terms of income, employment and homeownership between Samoan, Cook Islands, Tongan and Niuean households between 1981 and 2006.
The findings indicated that median equivalised income increased for all Pacific households over this period, particularly for Samoan households, but single-parent Niuean and Tongan households were worse off economically than the other Island groups.14
Moreover, an increasing proportion of Pacific households worked more than 48 hours per week with parents working multiple jobs. In effect, Pacific households are more likely to have insecure economic positions.26 There is evidence that homeownership is declining across all Pacific families, with approximately 56.8% of Europeans owning a home in NZ compared to only 18.5% of Pacific people.27
Issues with measuring family wellbeing Family wellbeing is a complex phenomenon to measure particularly with evolving family types, size and cultural understandings. The Families and Whānau wellbeing conceptual framework (FWWCF) 21,22,28,29 was developed in an attempt to understand and measure the wellbeing of families in NZ. Grounded upon the ecological systems theory,30 resource theory17 and family systems theory,31 this framework posits that for families to execute their function successfully, identifying and understanding the wider contextual influences such as economic, social, cultural, environmental and demographic forces surrounding families is important. The framework considers physical, material, emotional and social wellbeing factors that are vital and directly linked to how families effectively function.21 In addition, the FWWCF is contingent on four ‘domains of influence’. They include the safety and health of families, supportive family relationships, economic security and social connections to the community in which they live. It is understood that these factors interrelate and contribute to the wellbeing and successful functioning of families in NZ.
The FWWCF measure is to some extent, similar to Pacific notions of holistic wellbeing as captured in the Pacific Identity and Wellbeing Scale-Revised (PIWBS-R)32 and the Fonofale Model of Health.33 The Fonofale model and PIWBS-R are ‘individualised’ measures and do not measure family wellbeing. However, they are still valuable for our understanding of the wellbeing of Pacific families. The PIWBS-R measures a Pacific individuals’ identity and wellbeing 32,34 and is based on six constructs informed by both the Pacific and international literature on wellbeing and identity. These constructs include, perceived familial wellbeing;
perceived societal wellbeing; group membership evaluation; Pacific connectedness and belonging;
religious centrality and embeddedness; and cultural efficacy. 32,34
Similarly, the Fonofale model of health is informed by Pacific notions of health and wellbeing and is represented metaphorically by a fale (Samoan house).33 The structures that form the fale encompass the different factors necessary for the health and wellbeing of Pacific individuals. The foundation of the fale symbolises the aiga (family). The roof represents an individual’s beliefs and cultural values that are emblematically speaking, provide shelter and guidance to life. The four posts of the house depict spiritual, physical, mental and other aspects of an individual’s life such as gender and