Libraries and Learning Services
University of Auckland Research Repository, ResearchSpace
Copyright Statement
The digital copy of this thesis is protected by the Copyright Act 1994 (New Zealand).
This thesis may be consulted by you, provided you comply with the provisions of the Act and the following conditions of use:
• Any use you make of these documents or images must be for research or private study purposes only, and you may not make them available to any other person.
• Authors control the copyright of their thesis. You will recognize the author's right to be identified as the author of this thesis, and due acknowledgement will be made to the author where appropriate.
• You will obtain the author's permission before publishing any material from their thesis.
General copyright and disclaimer
In addition to the above conditions, authors give their consent for the digital copy of their work to be used subject to the conditions specified on the Library Thesis Consent Form and Deposit Licence.
IN CLOSED HEAD INJURED CHILDREN
A thesis presented in fulfilment of the requirements for the degree of Doctor of Philosophy in Psychology
at Auckland University
GERALD ALEXANDER 1990
11• •
Dedications
This research is dedicated to all who will or have
suffered the debilitating effects of a head injury. May this research contribute something of value to their rehabilitation of attentional functions.
Abstract
This thesis investigates a model first introduced in the applied setting for improving I.Q. scores, but this time used for rehabilitation of attention deficits in closed head
injured children. The dynamic assessment model follows very closely an already well established methodology, that used in single subject designs. Five subjects were recruited, who had suffered a closed head injury at least two years prior to this study. They were reported as having concentration and/or
impulse control problems. They were trained on two tasks
typically used to assess deficits in concentration and impulse control; the Continuous Performance Test (CPT) and the Same- Different Test (SDT), respectively. A multilayered design, comprising primarily of a multiple baseline design across
subjects with probes was used. Each of these were superimposed with an alternating treatments design with continuous
baseline. This complex design was used to evaluate training effects, maintenance effects, and generalization of treatment effects. The results showed that although the majority of
subjects did not show an initial attention or academic problem in the classroom as reflected by the Conners Teacher Rating Scale and the arithmetic subtest of the WRAT, all did show positive changes in academic achievement, in terms of the WRAT scores, following the cognitive retraining programme. Varying stimulus probability, coupled with feedback and reinforcement, increased discriminability in four subjects and efficiency, in
IV
terms of reduced inter-response times, in two subjects on the Continuous Performance Test; and discriminability in three subjects, and detectability in all subjects on the Same- Different Test. The results show indications of the treatment effects being maintained and generalized, in some subjects, not only to directly related tasks, requiring concentration, selective attention, impulse control and information
processing; but also to other distant tasks like classroom attention, academic achievement and, to a lesser degree, spatial attention. Alternative explanations for these
generalization effects are possible and further research needs to look at this in more detail. Such an assessment paradigm could be useful for rehabilitation purposes.
Acknowledgements
I am greatly indebted to Associate Professor Ivan Leslie Beale for taking me on as his PhD student. He has not only been a good guide in my acquisition of knowledge, but also he has been a good friend who cares for my general well being.
Special thanks to Dr. Dorothy Gronwall who helped in
recruiting some of the subjects. She also taught me many good clinical skills.
I would like to thank each of the subjects who
participated in this study, without who's help this research would not have been possible. Thanks are also due to the administrators of the QUICKCAT, MOTAT, the ZOO, KERRIDGE
ODEON, and RAINBOW'S END FUN PARK, for providing sponsorship for this research, in the form of free tickets to their
facilities. Many thanks to Mr. Ian Twentymn for helping me
write and/or edit some of the computer programmes used in this study. Thanks to Ms. Lynette Tippett for doing the
neuropsychological assessments. Special thanks to Dr. Denis Moore and Mr. Bradley Bridges for all their help as well.
I am grateful to the Medical Research Council and the Head Injury Society (Auckland Branch) for their financial support of this study.
I am also grateful to my dear and loving parents for being patient and supportive of all my academic endeavours.
Finally, I would like to publicly acknowledge the total support offered to me by God.
Table of Contents
vi
1.Dedications...ii 2.Abstract...iii 3.Acknowledgements... v 4. List of Tables... vili 5.List of Figures...
6. Chapter 1: Overview...1 7.Chapter 2: Dynamic Assessment...3 8.Chapter 3: Remediation of Attention Deficits Following
Concussion...H- ' S' -Attention...13- ; ? -Remediation of Attention... 14ii 9.Chapter 4: Concentration and Impulse Control... 30 3 (>
-The Continuous Performance Test...31 -The Same-Different Test... -35- 9 1
-Generalization of Treatment Effects...38-<7 -Aim of Study... .-41 y 10. Chapter 5: Method...43 5 o
-Subj ects...43 so -Settings...43 ^0
-Equipment and Software...44si -Design...44:~{
-Procedure:
*CPT...45^?
*SDT... 48- 5S- -Generalization Probes:
♦Rating Scales...58-^^
«WRAT... 5±-£ <?
«SAT... 52-S~
«Mesulam... S3— (
«Children' s PASAT... 54- ,
«Cancelling Test (d2)... 55- 11. Chapter 6: Results... 5S t
-CTRS... 5S-6 Q -RBPC... 57 -WRAT... 58 6 A, -Computer Training:
«Performance on the CPT... 62-"7 o
«Performance on the SDT... 8S- ^3 -Generalization Probes:
«Maintenance effects... 56 io*t
«Train to generalize... 93.10-7
«Train common processes
and/or Train and hope...102 >10
«Train common processes... 104* 'l'x- 12.Chapter 7. Discussion... H6
-Generalization of Treatment... H®- 12.»
13.Appendix 1.Neuropsychological data for main study...126 14.Appendix 2.Pilot Study... 155 15.Appendix 3.Neuropsychological data for pilot study....189 16.Chapter 8. References... 207
Vlll
List of Tables
Table 1. Z scores on the Conners Teacher Rating Scale....^59-
6 7
Table 2. Normalized T-Scores on the Revised Behavior Problem Checklist...SO (,%
Table 3. Standard scores on the arithmetic subtest of the Wide Range Achievement Test...
Table 4. Summary of statistical analyses on the CPT across
subjects... -ST- 15
Table 5. Summary of results of the cognitive strategies
employed... TT %
Table 6. Summary of results showing declines in
discriminability... T8-gG
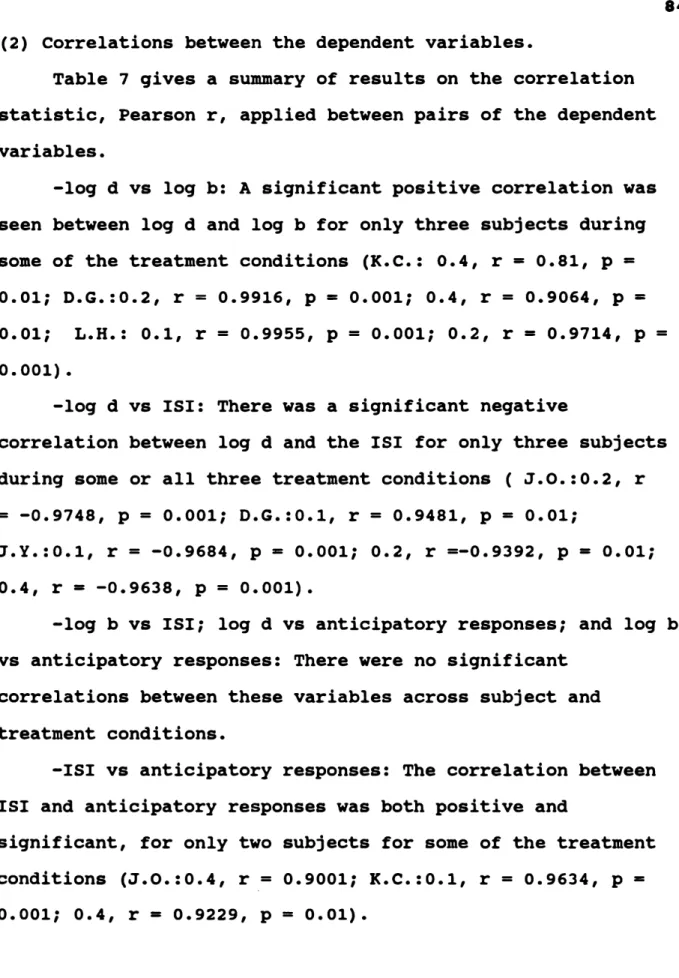
Table 7. Summary of results on the correlation (Pearson's r;
one tailed test) between the different dependent
variables presented separately for the CPT and the SDT ...-T9«?7
Table 8. Summary of the statistical analyses on the
SDT...8T-9'
List of Figures
Figure 1. Discriminability (log d) on the CPT... 69* "7 7
Figure 2. Response bias (log b)on the CPT... 70/9
Figure 3. Proportion of anticipatory responses on the CPT .74
Figure 4. Final inter-stimulus interval (ISI) on the CPT ..75-^3
Figure 5. Discriminability (log d) on the SDT... 8S-
Figure 6. Response bias (log b)on the SDT... 90 8
Figure 7. Proportion of anticipatory responses on the SDT..93-io|
Figure 8. Proportion of correct detections on the SDT....94-a
Figure 9. Proportion of correct observing responses on the
SAT... ...t&Oios
Figure 10. Proportion of correct instrumental responses on the SAT... iei-
/O Of
Figure 11. Results of the error index of spatial attention on the Cancelling Test (Mesulam) ... 103-
"1
X
Figure 12. Proportion of correct responses on the Children's PASAT •••••••••••••••••••••••••••••••••••••••••••••«••lvO<x*
g»-
11
Figure 13. Average speed of correct responses on the
Children's PASAT ... 196 lily
Figure 14. Scaled results on the Cancelling Test
(d2)... 199 H7
CHAPTER 1 OVERVIEW
Some of the general problems faced by concussion patients are the deficits in the ability to concentrate and control
their impulses. These are a few basic processes, among others, needed for use in the acquisition of new knowledge and skills, and in the use of old ones as well.
Varied computer tasks commonly have been used to help such people regain a certain proportion of their premorbid cognitive abilities. Most of the studies using such tasks, as cited in the rehabilitation literature, have lacked scientific rigour in assessing the strengths and weaknesses in such
cognitive retraining in the recovery process.
This thesis hopes to remedy this situation by adopting a particular paradigm that fits in well with an already
established methodology. Rather than assessing what has
already been learnt and present in the client's repertoire, as static assessment does, the focus is on the process of
learning or the response to treatment, as in dynamic
assessment. This will be examined in the next chapter. Chapter 3 looks at the consequences of concussion and the literature is briefly reviewed to see what has already been done in the area of cognitive rehabilitation especially of attention deficits in this population. Chapter 4 explores two commonly used tasks, the Continuous Performance Test and the Matching to Familiar Figures Test, used typically in static assessment
2 of concentration and impulse control respectively. It is
suggested that fitting similar tasks into a dynamic assessment paradigm will increase their usefulness as rehabilitation
tools. This thesis sets out to empirically investigate the use of the dynamic assessment framework as a basis of evaluation of a treatment method.
CHAPTER 2 DYNAMIC ASSESSMENT
The more traditional form of assessment, static
assessment, which is commonly used, does not test the capacity to learn but rather what has been learned (i.e. assets or
deficits measurement). On the other hand, Dynamic Assessment is the measurement of learning potential requiring a
continuous assessment of the client with a test-teach-retest format (Badad & Budoff,1974; Campione & Brown,1979;
Feuerstein,1979; Lidz,1981,1987). Dynamic assessment was developed for use with culturally disadvantaged, low- performing Israeli adolescents (Feuerstein, Rand, &
Hoffman,1979). Since that first study this paradigm has been used with those with environmental and\or developmental
handicaps. (A review of this can be found in the article by Saveli, Twohig, & Rachford (1986)).
The term '’potential" in this definition of Dynamic assessment may carry an unwarranted implication that the ability in question was always present and needed only to be uncovered. In effect however, the child is taught by various means to perform a task that she/he was initially unable to carry out. This definition implies a continuous charting of recovery as opposed to a single assessment. Further, it
implies that the subject acts as its own control as opposed to comparing against a normal population to evaluate deficits or assets.
4 From its early beginning, dynamic assessment has focused on the degree of change in learning possible with respect to I.Q., with the measure for educability based on a test-teach- retest philosophy. The issues explored in this type of
assessment include learning potential, the underlying processes to be trained, and transfer of training to
dissimilar tasks. The basic idea is that cognitive development is shaped by interactions with adults. This is also termed mediated experiences, and is said to be the basis of dynamic
assessment. Therefore by definition dynamic assessment is an interaction between an examiner-as-intervener and a learner- as-active participant, which seeks to estimate the degree of modifiability of the learner and the means by which positive changes in cognitive functioning can be induced and maintained
(Lidz,1987).
So, in summary, the differences between dynamic
assessment and static assessment can be stated as follows. The <
subject acts as its own control (dynamic) as compared to the subject being evaluated with respect to the so called normal population (static). The response to a particular treatment is being evaluated using the subject's own personal baseline index (dynamic) as compared to no sole focus on such a
response to treatment (static). There is a great emphasis on transfer of training to related and unrelated tasks (dynamic) as compared to a less direct concern for external validity '
(static). The underlying principle is process evaluation i.e.
examining how things are learnt (dynamic) as compared to
product evaluation i.e. determining how much already has been
learnt (static).
Severson (1976) advocates modifying the teaching
environment until the client is learning as efficiently as possible. Reinforcement (Severson,1976; Kratochwill &
Severson,1977) and feedback (Ozer & Richardson,1974) are examples of interventions suggested to enhance learning or to create an enriched environment. The Dynamic assessment
paradigm has not been widely adopted as compared to the Static assessment paradigm. Hamilton (1983) attributed this to
factors such as additional time requirements, perception by professionals of the procedures as yielding information that is too different from traditional procedures, lack of adequate development of the procedures, and an inadequate dissemination of information.
Two types of dynamic assessment have been identified, functional and structural (Lidz,1987). The former refers to enhancement of performance on specific tests. Training on
particular tests which require underlying cognitive processes for their successful execution may be improved through
repeated practise and/or feedback and reinforcement. The latter points to structural changes in the client (e.g., the use of Learning Potential Assessment Device by Feuerstein, et al. (1979) and Feuerstein (1980). The logic of structural dynamic assessment is that the training of a fundamental
cognitive process will cause a transfer of training to related processes. Such a transfer would promote the formation of new cognitive structures. The major focus of this thesis is on both functional and structural dynamic assessments. Functional
6 dynamic assessment will be explored since the emphasis will be on improving performances on specific computerized tests with predefined interventions. On the other hand, structural
dynamic assessment will be indirectly explored by periodically sampling performances on untrained tasks that require related and/or unrelated processes for their successful execution. The treatment plans help test and generate hypotheses with respect to rehabilitation thus maximizing the use of expensive
professional time. The key indices to record when
administrating dynamic assessment are how much improvement is achieved (metric of learning efficiency), and, how much aid is required (Campione & Brown,1987).
Tracing the history of this sort of assessment needs to begin with the concept of the zone of proximal development which is the distance between the actual developmental level as determined by independent problem solving (baseline
measurements) and the level of potential development as determined by problem solving under adult supervision or in collaboration with more capable peers (measurement after intervention) (Vygotsky, 1935, 1978). As Lidz (1987) puts it, if the gardener decides only to evaluate the matured or
harvested fruits, he cannot determine the state of his orchard. The maturing trees must also be taken into consideration. Correspondingly, it is claimed that
psychologists should not limit their analysis to functions that have matured, but must consider those that are in the process of maturation. If they are to fully evaluate the state of the child's development, psychologists must consider not
only the actual level of the development but the zone of
proximal development as well (Vygotsky,1935,1986). There is ay need to identify the processes which have not matured but are maturing (Vygotsky,1984a).
The dissatisfaction with traditional assessment tools, especially standard I.Q. tests is most often grounded in one or more of three arguments:
1. Traditional assessment deals only with the products of ? learning, disregarding learning processes;
2. Traditional assessment does not provide prescriptive
information regarding potentially effective interventions;x 3. Traditional assessment do not address the responsiveness of a child to instruction (Anastasi,1988).
In traditional assessment it is assumed that a subject's
current score on some psychological tests (a measure of prior learning) have quite a good predictive validity about future behaviours (a measure of future learning). This argument is based on the assumption of the equality of prior learning experiences.
Dynamic assessment (see Babad & Budoff,1974; Carlson &
Wiedl,1979; Feuerstein, et al., 1979, Feuerstein, 1980;
Campione & Brown,1987) has been viewed as a viable alternative to traditional testing, but not without some criticisms. For example, interventions like coaching will lead to decreased test validity with the related problem of score comparability.
The concept of the learning potential is not as clear as one would like it to be. The measurement of change is riddled with
internal validity problems (Cronbach & Furby,1970).
8 Most of the criticisms levelled against dynamic
Assessment can be overcome by a strict adherence to a single subject design methodology (see Kazdin,1982). Such problems as those related to internal and external validity have been
adequately handled in single subject research. This sort of methodology had its roots in the well established area of the experimental analysis of behaviour, where causal relationships between target behaviours and introduced interventions could be validly established depending on the experimental designs used. From this grew another related and dominant field,
applied behaviour analysis. In this area, the principles and methodologies learnt from the experimental laboratories were utilized for human situations and problems. The underlying
principles in both these areas of single-subject research were that once stable baseline behaviour was established an
intervention could be said to have caused behaviour change if the target behaviour alters and remains stable at that level during or after intervention. From this basic AB design
emerged more valid, complex, and above all, proven single subject designs (see Kazdin,1982). Further, the principles of applied behaviour analysis have been employed in Neuro-
behavioural Rehabilitation (Horton, Wedding, & Phay, 1981).
Neuro-behavioural Rehabilitation, is applied to patients after neurological insult, and focuses on the antecedents of
behaviour, the target response and it's consequences, to deal with remedial training for memory, concentration, reasoning, and orientation (Gloag,1985). This new methodology has
established good internal and external validities (Horton et
al.,1981). Evaluation of change has been adequately covered in Kazdin (1982). This model fits in well with the philosophy of dynamic assessment where rather than measuring the client's deficits in cognitive functions the goal was to evaluate the modifiability of these impaired functions, but by using the behavioural paradigm.
In summary it is seen that dynamic assessment focuses on <
the processes of learning with suggestions for teaching
whereas static assessment deals with the products of learning, y Further, dynamic assessment has many characteristics in common with the already established methodology in behavioural
assessment which helps overcome both internal and external validity problems. Therefore, making use of the philosophy of dynamic assessment and the already well established
methodology of neuro-behavioural assessment could be advantegeous for empirical research in this area.
The seeming weakness of the process training approach (see Beale & Tippett, in press) has typically not been from bad theory so much as from inadequate models for evaluating the effectiveness of treatment. This would imply that if an adequate model could be found and applied for assessing the effectiveness of process training, it would help explore the validity of such training. Adequate research in this area requires a model that incorporates both assessment and
treatment considerations. As the next chapter would highlight (see Remediation of Attention in Chapter 3) most of the
studies of process training used either, a between groups design that is insensitive to individual variations in
10 response to training, or poor single-subject designs or
variations of it, that makes evaluation of training difficult.
What is needed is a generalization training or testing model to provide convincing evidence that, training on a task that supposedly needs a psychological process for it's successful execution, results in more than just improvements in the process-training task. Generalization effects of training to untrained tasks that require similar or different processes needs to be shown to have occurred as well. It is felt that using the dynamic assessment framework as a basis of
evaluation of a treatment method, may enhance the validity of process training.
So far, most of the research in this area of dynamic assessment has focused on populations who are either
culturally, socio-economically or developmentally handicapped in some way. The application of such an assessment model has yet to be applied to people with acquired cognitive
disabilities. This thesis will explore the application of this dynamic assessment paradigm (i.e. functional and structural dynamic assessments) for the measurement, treatment and evaluation of attention deficits following closed head injuries.
SU, *4
Q 4 '
(a- rvv. ’ •> ’ <• 1
r
(4 • i
I
\
I vt.
4
CHAPTER 3
REMEDIATION OP ATTENTION DEFICITS FOLLOWING CONCUSSION
The present research set out to explore the utility of the dynamic assessment paradigm in children who had suffered the debilitating effects of concussion. Before proceeding further it needs to be made explicit what is meant by
concussion and what are the ensuing consequences of it. A closed head injury is defined as a nonmissile, blunt or diffused insult associated with acceleration/deceleration forces applied to the head. Concussion is a brief loss of consciousness followed by prompt recovery more often without any localizing neurological signs (Bakay & Glasauer, 1980). In other words concussion may also occur with open head injuries where neurological signs are more focal or localized.
There are some general neural consequences of closed head injuries. This can be primary damage directly related to the instantaneous blow or hit, generating either acceleration or deceleration forces like translational and/ or angular forces
(Denney-Brown & Russell,1941). It also could be caused by nonacceleration dependent forces such as impression trauma, ellipsoidal deformation, or skull vibrations. Further, such primary brain damage may lead to secondary brain injuries due to forces generated by haematomas, edemas and/or increases in intercranial pressure.
The actual damage to the brain occurs when such forces, especially the acceleration or deceleration forces, lead to
12 the shearing and stretching of nerve fibres causing wide
spread injury to the cerebral white matter or axons (Ewing- Cobbs, Fletcher, & Levin,1985). This has been termed diffuse axonal injury. Contusions at the skull brain interface,
ischemia or hypoxia and haemorrhages may add to the list of injuries to the brain.
The typical brain systems affected by a concussion include: the arousal or alertness system consisting of structures in the brain stem particularly the ascending reticular activating system; the frontal and the temporal
lobes. The frontal lobe handles among other functions, impulse control (Oas,1985) while one key function of the temporal lobe is memory storage. These are areas susceptible to among other injuries, diffuse axonal injuries, and contusions (Adams, Graham, & Gennarelli,1985). Therefore it is no wonder that very often the major sequelae to concussion include poor concentration and poor impulse control (Chadwick,1985).
It has been suggested that for some closed head injured clients a partial neurophysiological recovery may take place soon after the injury. This recovery includes axonal
regeneration (Burgess & Horch,1973); collateral sprouting (Cotman, Gentry & Steward,1977); unmasking of formerly
inefficient synapses (Wall,1980); and increased sensitivity of synapses (Laurence & Stein,1978). Pharmacological techniques used to aid recovery include the use of cholinergic agents like amphetamines. Behavioural techniques have also been
utilized to assist in the rehabilitation of the head injured.
These include the retraining of lost skills, the use of
different behavioural strategies, compensation through the use of remaining intact brain areas, substitution, and cognitive retraining by directly addressing specific skills deficit areas and promoting the process of learning with repeated practice on that task. Finally, providing an enriched
environment that can compensation for certain deficits also aids in the rehabilitation process.
Before proceeding to review the literature on remediation of attention following a closed head injury it is necessary to consider definitions and classifications of attention.
Attention
There is a lack of universal acceptance or clarity in the definitions of attention (Stuss & Benson,1986). Posner and Rafal (1987) have proposed a three tier model of attention comprising alertness (tonic as well as phasic), selective attention, and effort. Luria (1980) conceptualized attention ,
z
as a hierarchical function consisting of three functional
units. The first functional unit deals with arousal, alertness and cortical tone which has been attributed to the subcortical regions including the brain stem, the diencephalon and medial regions of the cortex. Functional unit two is concerned with the obtaining, the processing and the storing of information which have been attributed to the lateral regions of the neocortex on the convex surface of the hemispheres including the occipital, temporal and parietal regions. Functional unit three covers the programming, regulation and verifying of both
14 covert and overt behaviours. This typically has been
attributed to the prefrontal divisions of the frontal lobes.
As stated above, the typical sequelae to a closed head injury includes reduced attention. This covers a shortened attention span, reduced arousal, slower reaction times, poor concentration, decreased information processing abilities
(Gronwall & Wrightson,1981), impaired selective attention, and poor impulse control. So, in behavioral terms, this reflects a deficit in both stimulus control and response control.
Remediation of attention
Remediation of attention can take many forms. Typically clinicians and researchers in this area work from a particular model of cognitive rehabilation.
There has been a heavy bias towards Diller's model of cognitive retraining. Unlike Luria's strengths approach which uses the intact islands of cognitive strength to compensate for damaged areas, Diller's model focuses on remediating deficient areas. Essentially the "rehabilitation task” is a controlled task during which a specific impaired skill can be isolated and hopefully retrained (Horton, et al., 1981).
The literature will now be briefly reviewed to examine some of the research done in this area of cognitive retraining of attention. Although most of the studies have many positive points to their credit the prevalent criticisms against the majority are their poor displays of both internal and external validities. Further, there appears to be a general lack of
emphasis on the rationale for using a particular training task and methodology.
To treat reduced arousal and poor attention following head injury Miller gave his patients sufficient training to improve their simple reaction times to levels comparable with those of non impaired patients (see Miller,1980). The task used was the Minesota Spatial Relations Test requiring the fitting of fifty-eight shapes into their corresponding holes.
The study looked at the performance of two groups, a head
injured group and a control group, with the only intervention mentioned that of practice on task. The results showed that with practice performance (in terms of mean reaction times)
for both the brain injured as well as the control group
improved (i.e. reaction times decreased) with good transfer of training from one board to another. Nevertheless, the head injured group had a lower rate of learning as compared to the control group when they were matched for initial performance levels. The implication here was that practice itself was not sufficient for improvements to occur. Further the test used had the possible disadvantage of having a ceiling effect on performance. Other criticisms that can be levelled against this study include the following. The author presented group data, in the form of mean scores, in a serial fashion, to chart progress on the task as if they were single-subject data. There was no mention of inter-subject variability in these data. The selection of the control group was not made clear, and the change of test boards when the data had not stabilized, especially in the head injured group was not
16 clearly justified. Therefore, the results should be accepted with caution.
Three perceptual and four memory computer programmes were presented in the handbook by Gianutsos and Klitzner (1981) all of which required the use of substantial components of both attention and concentration. Unfortunately little empirical data were presented to justify the use of these programmes for attention retraining although conceptually they seemed
appealing (apparently good face validity).
Lynch (1981) provided a guide list of a variety of Atari video games with suggestions for the use of these for
cognitive rehabilitation. Once again hard empirical evidence was lacking to support their use for rehabilitation purposes.
Ten different computer programmes for training both visual and auditory reaction times were presented by Bracy
(1982). Training included performances on multimodality
reaction tasks which required the client to alternate between initiating and inhibiting responses cued by auditory and
visual stimuli. Once these were mastered, more complex and demanding computerized activities were introduced. Very little empirical evidence on the success of this training programme was presented.
G
Gross,Ben-Nahum and Munk (1982) outlined intervention strategies that were needed to enhance training on cognitive training tasks. These include the use of reinforcement and feedback. They presented a number of studies that were used to train attention. In one study the clients were presented with a linear array of numbers, letters, or symbols. Half of these
consecutive symbols were masked and the mask was moved along the array so that the client was required to name the next
symbol that was to be uncovered. Successful performance on the task required attention, concentration and memory. The results of this training programme showed that, with practice,
performance on the task improved. Unfortunately, details of the design used or the intervention strategies utilized in this particular experiment were not provided. Therefore,
conclusive statements about the usefulness of the programme or the essential components that facilitate change in attention cannot be made. In another study, two sets of cue lights (ten in each set) formed the basis for training divided attention and effort. The task required the matching of one of the lighted top sets of bulbs with the switching on of a
corresponding light in the bottom set according to a
predefined rule. A group design comprising of four subjects was used with a baseline phase, a control training phase and an experimental phase. However, it was unclear how baseline was different from the control training phase, with subjects having to switch on the similar positioned light in the bottom set as in the top set during both phases. For the experimental training phase it was stated that the subject was required to follow different rules on the bottom set. For example when light 1 was on in the top set, the subject was required to switch on light 3 in the bottom set (i.e. skip every other light). No details of the training data were presented but probes were taken across the three phases and averaged across subjects. These probes included the Matching Familiar Figures
18 Test (a measure of impulsivity) and the subtests of an
intelligence test (WAIS). The results showed that experimental training effected the greatest improvements in the probes as compared to baseline or control training. Nevertheless, the study was weak in terms of both internal and external
validities. Firstly, the design used was an A-B-C design, with no clear mention of what the two interventions were. According to Kazdin (1982) such a design lacks validity since firm
conclusions can not be drawn about the effectiveness of either intervention in changing target behaviours. Further, averaged results obscure individual variability especially when it is presented in a single-subject design format. Just recording probe data in the results section do not give any indication of how performance changed on the training task itself.
Therefore, the conclusions that may be drawn from this study are suspect due to the poor internal validity. It also
prevents any sort of future experimental replication and validation of the findings due to the lack of clarity of certain procedures used.
Newcombe (1982) refers to two rehabilitation centre programs that purportedly give systematic training on
attentional tasks, like the PASAT, to increase attention span.
Feedback for correct responses, in the form of auditory tones, was used to improve and maintain increased attention spans.
Nevertheless, as stated by the author, no objective evidence of the effectiveness of these techniques was available, either due to an insufficient amount of data that was available
and/or due to the uncertainty of the experimental designs
used.
Gummow, Miller and Dustman (1983) reviewed the literature on cognitive rehabilitation of attention following head
injury. They showed that the typical strategies used for this particular purpose included the use of simple repetitive
tasks, and teaching the clients to use alternative information to solve problems, thus promoting neural compensation. As
stated by the authors, there are two alternative definitions for this concept of neural compensation or compensatory neural reorganization. The first definition had been put forward by Luria in 1963, in which he speculated that such a neural
phenomenon may imply the transfer of the damaged function into another brain region. An alternative view was stated by Bach- y-Rita in 1981, in which she viewed it as the unmasking of pathways that either subserve or have a similar role to those damaged by lesion. Based on the reviewed literature, Gummow et al. suggested that tasks could be simplified and the clients encouraged to succeed in their own rehabilitation programme as a means of achieving greater success in the cognitive
retraining process. Unfortunately, no detailed analyses of these studies, like the experimental designs used, were
presented to support any of these suggestions or claims. The authors tried to justify the use of the computer for
rehabilitation purposes by expounding on its various
advantages. Among these were it's patience in the training process, it's inherent motivating capacity due to the novelty of such a machine, and the overall economics of it in terms of the efficient involvement of many patients with limited number
20 of therapists. In conclusion they called for more scientific rigour in the use of computers in some rehabilitation tasks, like reaction time tasks, to bring more credence for such therapies.
Using a method of self instruction modeled after
Meichenbaum's procedure Webster and Scott (1983) trained a head injured patient on an attention task. The client had
suffered a closed head injury resulting in attention deficits.
The task required the client to be prepared to listen for signals using self-statements and then to repeat each word spoken, subvocally. Using an A-B design, this strategy was taught to the client after baseline measurements. They found that both attention and memory improved in the client. The probes used to assess change were based on self-report statements by the client in relation to his general well being, his sexual functioning and his job performance. No mention was made of any sort of intervention to motivate the already highly motivated client except that continued exposure on task was used. Once again, the looseness of the design
(i.e. just an AB design) prevents the extraction of any firm conclusions. It was obvious that the experimenter could not use a reversal design due to the nature of the task and
intervention, but a multiple baseline design across subjects, with probes, could have added more weight to the claim that self statements were an effective means of improving attention and memory. Further, the task itself charts changes in two cognitive functions intertwined in a confounding fashion.
Wood (1984) stated that in rehabilitation attentional
processes needed to be attended to before other processes like memory. The author stated that it was essential to chart
improvements in attention scientifically. This meant that among other things, baseline measurements should be taken into consideration to help detect ceiling or floor effects and
trends in data. To make the analysis as objective as possible the behaviourial manifestations of this function (i.e.
attention) should be focused on. Further, it was stated that to motivate the client in the retraining programme the use of reinforcement and feedback were needed. It was also suggested that an adaptive rate ( i.e. one that changes it's criteria to prevent ceiling or floor effects) built into the training task will help clients reach optimal levels of performance. Wood outlined a number of tasks that could be successful in
retraining attention in head injured clients. These include an auditory vigilance task, a visual vigilance task, a visual
scanning task, a perceptual matching task, and a few other tasks requiring decision making, quick motor reaction and a maze learning task. The author stated that reinforcement could be used as an effective technique for improving attention
these particular tasks. Empirical evidence was minimal and little attention was paid to experimental designs. Therefore, there needs to be caution on the conclusions that can be
drawn.
Wilson and Moffat (1984) very briefly reviewed the
literature on attention training programmes for head injured patients. They reported that the most common task used for this purpose was the reaction time task. They focused on one
22 particular example, in which Blackburn, in 1958, found that feedback and reinforcement, used together, helped improve responding on a two-choice reaction time task for both the
control group and the brain injured group. They criticized the study because no baseline measurements were taken, no adequate charting of performances during intervention were presented, and there was a lack in emphasis on generalization beyond the training task. It was unclear whether the intervention alone, or the intervention combined with practice effects, brought about the improvements in reaction times on the task.
Adamovich, Henderson and Auerbach (1985) recommended the following techniques based on past research for treating
attention deficits following head injury. These include using a three stage treatment hierarchy of arousal and alerting, operative retraining (structured goal-oriented programs), and self reliant functioning in home and community environments.
Nevertheless, no empirical data were provided to support their
worth. Gx
b
Ben-Yishay, Piasetsky and Rattok (1987) utilized the orientation remedial module (ORM), a treatment package, to ameliorate attention deficits in their clients. One procedure called the 'attention reaction conditioner* was purported to increase arousal, alertness and responsiveness; while the
'zeroing accuracy conditioner' was supposed to improve
scanning, timing of response and anticipation. A third, the 'visual discrimination conditioner* was said to improve active scanning, processing, sustained attention; whereas 'time
estimation' helped to improve concentration and the focusing
on internal cues. The final task of this treatment package, 'the rhythm synchronous conditioner', aided in the sequencing of responses and improving all other functions mentioned
previously. Using a general group deign, with data averaged across subjects, and with pre and post test generalization probes, they found that with systematic exposure to the ORM treatment package improvements were noticeable on all tasks of the package. Although it was stated that feedback and social reinforcement were delivered to increase the number of correct responses, no data were presented to show this change in
accuracy, across time, on the training tasks. Generalization of treatment effects were seen on four untrained tasks
including Visual Reaction Time, the auditory 'Digits' subtest of the WAIS test, Picture Completion, and picture description test. Nevertheless, the experimental design used to explore these generalization effects lacks a strong framework as those advocated by single-subject design supporters (see Nutter &
Reid,1978) (i.e. it was just an A-B design). Only mean scores across subjects, comparing pre and post test generalization results were presented. Such analyses makes it difficult to determine whether the exposure on the ORM brought about the change in these probes or were these due to just a practice effect.
Sohlberg and Mateer (1987) experimented with a variety of both commercially available and original computer programs.
These were meant to train five levels of attention including sustained, focused, selective, alternating, and divided
attention. So this training package consisted of computer
24 tasks, with probes used to chart changes in target behaviour.
Using a multiple baseline design across behaviours replicated across four subjects, it was suggested that training on these computer tasks generalized to improvements in attention as measured by the limited multiple administrations of the Paced Auditory Serial Addition Test (PASAT) and the Spatial
Relations Subtest (SR) from the Woodcock-Johnson
Psychoeducational Battery. Performance on the attention
training tasks were not described. One main problem with this study was that too few probe data points were used and the design was not strictly adhered to. They were presented
inappropriately, in the results section, supposedly following a multiple baseline design. For example, movement from one phase to another was not sequentially done, as is required in a multiple baseline design. It does not really tell
conclusively that the training programmes brought about change in the dependent variables across subjects. Further, the
probes used, chart more than just changes in attention. They also help detect changes in short-term memory, and spatial attention. So it is not certain which particular cognitive process improved due to treatment. Once again the results have to be looked upon with caution.
Wood (1987) outlined certain problems with some cognitive training programmes in use today. These include their labour intensive nature and thus related high costs in running them.
Further, they seem so far drawn from the problems of daily
life with little emphasis on generalization from training task to related tasks in the everyday environment. The author
specifically stated that training should be organized around observable behaviours rather than on hypothetical processes to help the client to benefit from the programme in a concrete goal-directed fashion. He elaborated on three particular training programmes to ameliorate attention problems in
severely head injured clients. In the first study, following an ABAB design, the head injured adult was trained to sustain attention during therapy sessions. The intervention used was token reinforcement administered on a fixed interval schedule.
It was shown that contingent reinforcement did improve attentive behaviour. The second experiment showed the same pattern on two clients except that the design used was less convincing (AB design). In the third experiment, Wood tried to show that contingent reinforcement was instrumental at
improving attention on two tasks, an auditory vigilance task and a computer task (Possum basic skills teaching machine). Using four severely head injured clients, training was held in parallel on these two tasks. In the auditory vigilance task they were required to respond when a target series of three odd digits were presented verbally. Although it was stated that reinforcement tokens were given for correct responding and taken away for incorrect ones, it was not clear what type of experimental design was in force to evaluate the
effectiveness of such treatment. In the computer task, the subjects were required to move a light beam to the column in which the illuminated target symbol was found, by pressing a key on the Possum machine. In baseline condition, feedback in the form of two different tones were given depending on
26 whether the response was correct or not. During intervention, on top of the feedback, reinforcement tokens were delivered in the same format as in the auditory vigilance task. The design used here was just an AB design. The results for both tasks were presented as means scores across the four subjects at
fixed time intervals throughout the experiment. It showed that performances on the tasks improved for all subjects with
generalization effects recorded for attentive behaviour during therapy, and only marginal improvements in memory, like in the Rey learning task. This third experiment can be criticized on the grounds of poor designs being used (i.e. unclear for the first task; and just an AB design for the second task), the use of mean values that obscures individual variability, and the use of insufficient probe sessions that failed to
adequately sample changes in related behaviours.
. Wood and Fussey (1987) used computers for training
information processing. When a target stimulus passes a visual gate at the same time that the same stimulus passes below this visual band, an appropriate response was required that was not too fast/slow. A group design comprising of two groups who had suffered head injury and were already undergoing a general
rehabilitation programme was used. On top of this, one of
these groups was targeted as the experimental group to receive the attention training. The third group was a normal control group. Each of the groups underwent a baseline phase, a
treatment or no treatment phase, and a return to baseline (A- B-A design). Feedback was given for both correct and wrong responses. Further, probe data were collected following the
phases: baseline (A) and treatment/no treatment (B) (probe 1);
return to baseline (probe 2); and follow-up (probe 3).
Improvements in performance were seen on training task but no evidence were noticeable of generalization effects to
untrained tasks e.g., reaction time task, vigilance task, and attention rating scale. Once again this research had
noticeable limitations calling for caution on the conclusions reached. The training tasks data and the probe data were
averaged across subjects and presented as mean scores.
Therefore important individual data were lost in this statistical manipulation. The comparisons made between the three administrations of the probe package across the three groups leaves much to be desired about conclusions that can be drawn from this study to evaluate the training programme's efficacy. There was no initial probe at the start of the study for all groups so that at least practice effects could have been examined more carefully and hopefully ruled out as a possible explanation for improvement. There was also some doubt as to the use of a valid comparison group to evaluate change.
In summary, most of the attention related remediation programmes relied heavily on Diller's model of extended
practise (or overlearning) on computer tasks that require the use of attention for their successful execution. Over and above this, some studies showed that reinforcement and/or feedback for correct performance could improve attention on those tasks themselves or on the generalization probes.
Some of the main criticisms that may be levelled at most
28 of these studies dealing with the remediation of attentional problems caused by closed head injuries include the lack of a valid conceptual framework to justify certain training tasks or interventions used. There apparently was little
justification for some of the dependent and independent measures used and a very poor attempt made at measuring any clinically significant generalization of treatment or training effects. Many studies failed to take into consideration the fact that individuals manifest attentional problems in varying degrees or recover the use of some of these functions at
different rates so that finding the average performance level would lose essential individual data. Most of the research designs used did not measure up to the standards as advocated by applied behaviour analysis (Kazdin,1982), so that any
conclusions about treatment and/or generalization effects need to be made with caution.
Future research is obviously needed in this crucial area of rehabilitation and it is recommended that a better
experimental design (e.g., a variety of proven single subject designs) be used to study such a heterogeneous population. It should be borne in mind that this is a diverse population because, as stated in the paragraph above, not everyone who suffers concussion manifest the same level of deficit at any particular time. There also needs to be more emphasis on
internal, external and construct validities. It is suggested ' that the dynamic assessment paradigm could adequately tackle all these fundamental issues in rehabilitation. The next
chapter attempts to apply solutions to most of these issues in
the form of the dynamic assessment model and put forward a new proposal to ameliorate attention deficits in closed head
injured patients using computerized tasks.
Drawing from the wealth of knowledge gained from past intervention techniques a case can be made for training on tasks requiring various types of attention, while measuring generalization on other tasks introduced as probes. It should be borne in mind that generalization of treatment effects to untrained tasks have been explored in other studies as well.
What is unique in the present study is that the boundaries of generalization are explored to see to what extent distant untrained tasks or processes are affected by the direct training of two processes.
CHAPTER 4
CONCENTRATION AND IMPULSE CONTROL
Chapter 3 has clarified that the typical sequelae to a closed head injury are poor concentration and poor impulse control, fundamental processes for the acquisition of new
knowledge and the use of current or old ones. It is not to say that other processes like memory, perceptual, etc. are not
important or are not affected as well. Like everybody else, school-aged children or adolescents require all these
processes for daily functioning. The main reason for focusing on the application of the dynamic assessment model on just two of the affected processes, i.e. concentration and impulse control, is to explore the utility of such an assessment model in the rehabilitation field. Two psychological tests which have been used to measure concentration and impulse control (i.e. The Continuous Performance Test, and the Matching to Familiar Figures Test) have most often been used within a static assessment framework. Within this framework, these two tests have been used to assess the amount of attentional deficits in the client. It needs to be explored whether by applying a different assessment model, like the dynamic assessment model, another use may be derived from these
tests. Such a model purports to train target processes, and as the theory suggests, deliberately promotes transfer of
training to related processes. Therefore, such a model may be of value for rehabilitation purposes.
Each test will now be briefly reviewed to show how they were developed and used for their specific, basically static assessment aims.
The Continuous Performance Test fCPT)
Typically alertness (tonic) refers to a state of
sustained attention or vigilance (Davis & Parasuraman,1982).
The Continuous Performance Test (CPT) has been used typically to measure sustained attention, having its beginnings in EEG research on alertness or sustained attention (Rosvold, Mirsky, Sarason, Bransome & Beck,1956).
It is a short duration cognitive task involving the presentation of a quasi-random series of visual or auditory stimuli at a fixed and rapid pace. The subject is required to detect infrequent target stimuli amongst frequently occurring stimuli (e.g.,the letter A followed by an X). Rosvold et al.
(1956) found that brain damaged clients had difficulty detecting the target stimuli, thus implying a lapse in concentration or attention.
The CPT has been used extensively for assessment of cognitive deficits in children suffering from learning
disabilities, hyperactivity, and schizophrenia. It has been found that learning disabled children display lower accuracy on the CPT (Aman,1979; Anderson,Halcomb & Doyle,1973; Keogh &
Margolis,1976) and that they make more errors of omission and commission than normal children (Dainer,Klorman, Salzman,Hess,
& Davidson,1981). Swanson (1981) examined children with
32 learning disabilities and found that there was impairment in overall perceptual sensitivity level (a signal detection
index) but found no difference in decision criterion (another signal detection index) or in perceptual sensitivity decrement over time in comparison to normal children.
The CPT has been used to differentiate hyperactive
children from normal children (Douglas,1972). Impulsive errors on this test (responding prematurely) have been found to occur at substantially higher rates among hyperactive children than controls (Sykes,1969; Sykes,Douglas & Morganstern, 1972,
1973;Sykes,Douglas,Weiss, & Minde,1971).
Nuechterlein (1983) compared children of schizophrenic mothers with hyperactive children and with children of non- psychotic, psychiatrically disordered mothers. It was found that a disproportionately large sub-group of children at risk for schizophrenia displayed a deficit in perceptual
sensitivity.
Further, the CPT has been used in a variety of settings and with a variety of subject populations. It has been shown to be useful in assessing a wide range of behavioural,
pharmacological, developmental and psychiatric problems.
In one study, employing 12 hyperactive boys, performance on the CPT showed significant improvements during amphetamine treatment. Fewer commission and omission errors were made on