Increasing interest in the use of telerehabilitation (Brochard 2010) has prompted professional organizations to issue positions on its use (American Speech-Language-Hearing Association 2005; Wakeford 2005). Changes in the demographic composition of the population mean that the burden of stroke is expected to increase (Feigin 2003). Therefore, it is important to determine whether telerehabilitation services, once established, can lead to the desired outcomes.
Interventions were offered by one or more health disciplines (e.g., we planned to include studies involving only physiotherapy). Our intention was to perform sensitivity analyzes based on the methodological quality of the studies (allocation concealment, blinding of the outcome assessor, intention-to-treat analysis) to assess the impact of the risk of bias in the included studies. judge. Two studies recruited participants in the acute stages after stroke (Boter 2004;Mayo 2008), while the remainder of the studies involved participants in the subacute and chronic stages.
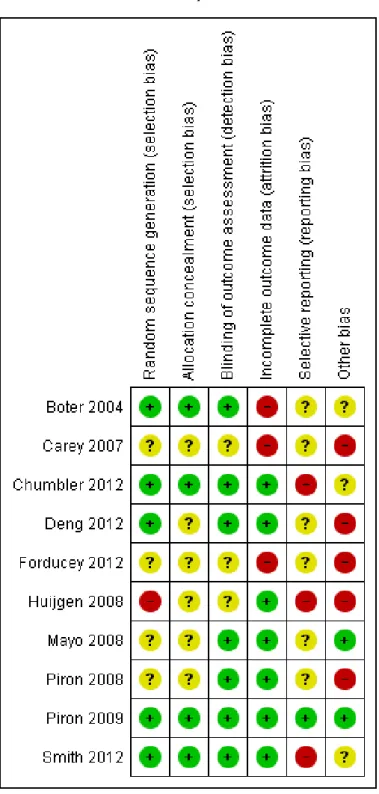
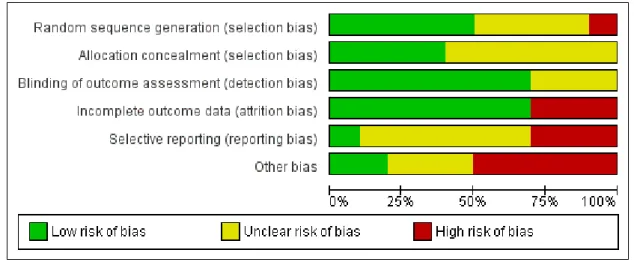
Regarding the comparative interventions used in the studies, two studies compared different models of telerehabilitation (Carey 2007; Deng 2012), five studies compared telerehabilitation with an alternative intervention (Forducey 2012; Huijgen 2008; Piron 2008; Piron 2009; Smith 2009) and the remaining studies ( Boter 2004 ; Chumbler 2012 ; Mayo 2008 ) compared telerehabilitation with usual care, when no specific intervention was provided by the testers. Allocation concealment was adequate in four studies (Boter 2004; Chumbler 2012; Piron 2009; Smith 2012) but was unclear in the reports of the remaining studies. One of the studies, which provided a case management intervention (Boter 2004), reported that participants in the intervention group had better scores in the domain of 'role limitations due to emotional health' on the Short Form (SF). -36; however, no other significant differences were observed between groups.
Another study, which also offered a case management intervention (Mayo 2008), reported that people in the intervention group were more likely to respond to one or more of the outcomes within the SF-36 subscales (odds.
Upper limb function
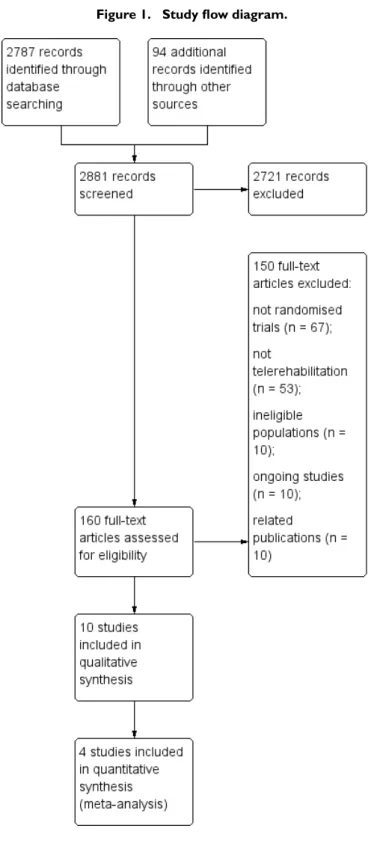
However, our review of 10 trials provides information about the current state of telerehabilitation research; we also identified 10 ongoing studies, suggesting that research in this area is growing. These studies appear to have been designed to assess the effectiveness of the case management intervention rather than telerehabilitation per se. Furthermore, although telerehabilitation is supposed to reduce the cost of administering an intervention, none of the studies included in this review reported on cost-effectiveness.
For example, the health care professional may make mistakes in the assessment of the patient, or the patient may misunderstand advice or instructions from the health care staff. Although a growing body of pilot and feasibility studies has been identified, additional RCTs are needed to determine the effectiveness of the intervention. Initially, it is important to understand whether differences have been identified in the delivery of the same therapy program in person or via information and communication technologies.
An exploration of the role of the nurse coordinator in a telemedicine-based stroke secondary prevention model.International Journal of Stroke2010;5(1):1. Joubert J, Reid C, Barton D, Cumming T, McLean A, Joubert L, et al. Integrated care improves risk factor modification after stroke: initial results from the Integrated Care for the Reduction of Secondary Stroke model. Journal of Neurology, Neurosurgery and Psychiatry. Assessment of a virtual teacher feedback for upper extremity rehabilitation after stroke.Neurorehabilitation and Neural Repair2012;26:4.
Rochette A, Korner Bitensky N, Bishop D, Teasell R, White C, Bravo G, et al. Study protocol for the YOU CALL-WE CALL trial: the impact of a multimodal support intervention after a "mild" stroke. Recommendations on the prevention, diagnosis and treatment of stroke: report of the WHO Task Force on stroke and other cerebrovascular disorders. Time after stroke: intervention group median 26 days, control group median 74 days Interventions Telerehabilitation intervention: the aim of the intervention was to improve par-.
Inclusion criteria: mild to intermediate arm motor impairment due to ischemic stroke in the area of the middle cerebral artery; without cognitive problems that can interfere with understanding. Interventions Telerehabilitation intervention: the goal of the intervention was to improve upper limb function using a virtual reality program. Selective reporting (reporting bias) High risk Additional outcomes assessed that were not reported in the paper.
Name or title of study Evaluation of the Gertner Tele-Motion Rehabilitation System for stroke rehabilitation. Interventions Intervention group: a 6-month intervention consisting of 4 face-to-face physiotherapy sessions (consisting of exercises aimed at a specific goal), 5 telephone calls and 1 to 2 text messages per week, to encourage continuation of the prescribed exercise plan.
Independence in activities of daily living: postintervention
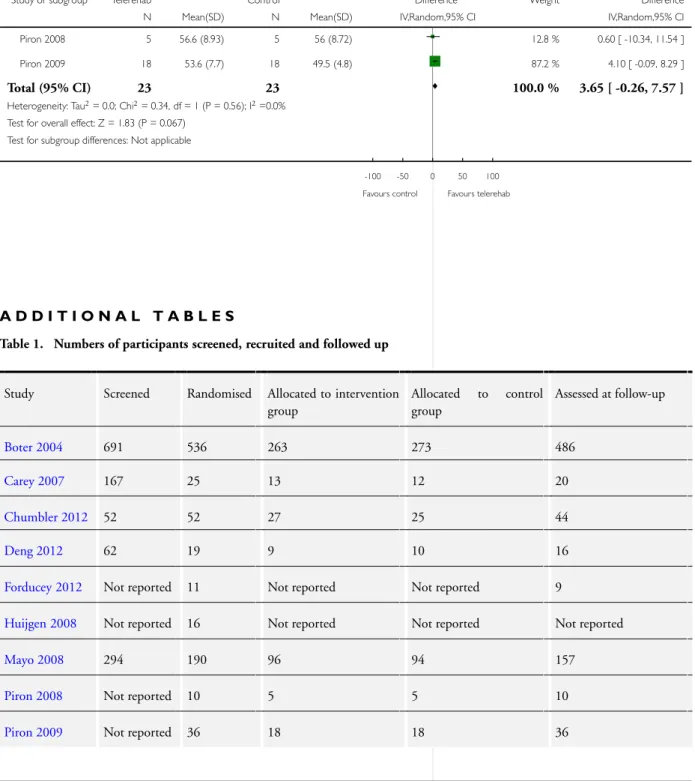
Upper limb function: postintervention
Comparison 1 Independence in activities of daily living: postintervention, Outcome 1 Independence in activities of daily living
Comparison 2 Upper limb function: postintervention, Outcome 1 Upper limb function
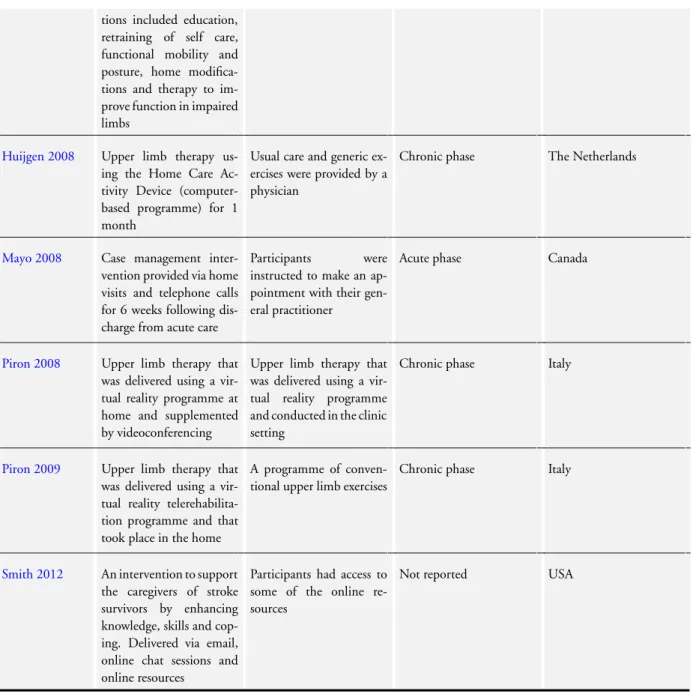
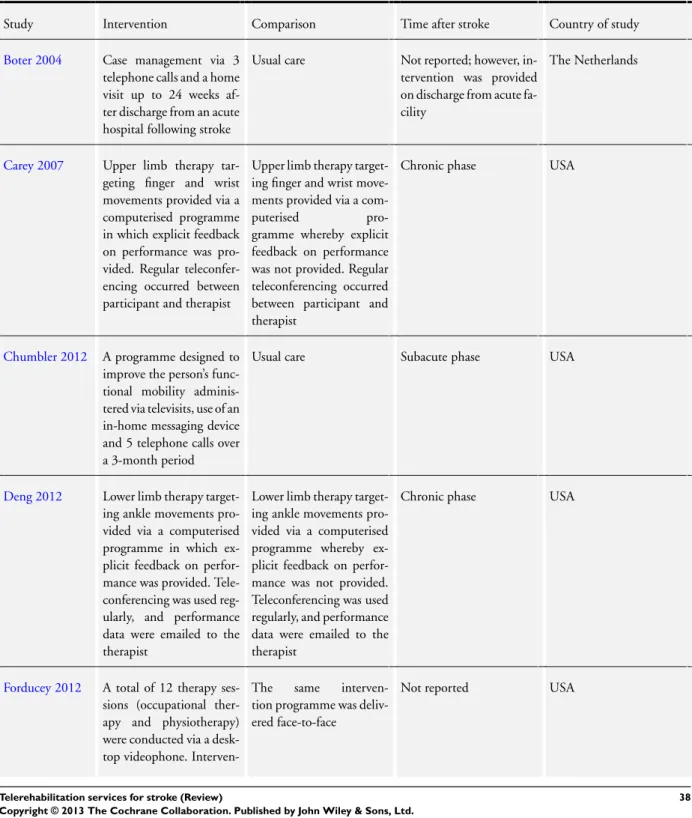
Boter 2004 Case management via 3 telephone calls and one home visit up to 24 weeks after discharge from acute hospital after stroke. Usual care Not reported; however, the intervention was performed upon discharge from the acute hospital. Carey 2007 Upper limb therapy targeting finger and wrist movements delivered via a computerized program in which clear feedback on performance was provided.
Chumbler 2012 A program designed to improve a person's functional mobility, administered via televisions, use of a home messaging device and 5 phone calls over a 3-month period. Deng 2012 Lower extremity therapy targeting ankle range of motion was delivered via a computerized program in which clear feedback on performance was provided. Lower extremity therapy targeting ankle movements was delivered via a computerized program, where no clear feedback on performance was provided.
Huijgen 2008 Upper extremity therapy using the home care activity device (computer-based program) for 1 month. Mayo 2008 Case management intervention delivered via home visits and telephone calls for 6 weeks after discharge from acute care. Piron 2008 Upper extremity therapy that was delivered using a virtual reality program at home and supplemented by videoconferencing.
Upper extremity therapy that was delivered using a virtual reality program and performed in a clinic setting. Piron 2009 Upper extremity therapy delivered using a virtual reality telerehabilitation program that took place at home.
MEDLINE (Ovid) search strategy
EMBASE (Ovid) search strategy
AMED search strategy
CINAHL search strategy 1. MH Cerebrovascular disorders
TX hemipar$ OR TX hemipleg$ OR TX paresis OR TX paretic AND TX brain injury$. TX telemedicine OR TX telerehabilitation OR TX telerehabilitation OR TX telerehabilitation OR TX telehealth OR TX telehealth 31. TX teletalk OR TX teletalk OR TX teleOT OR TX tele-OT OR TX telepractice OR TX teletherapy$.
PsycINFO search strategy
14 ((remote$ or distance$ or far) adj5 (rehabilitation or therapy$ or treatment or physio$ or occupational therapy$ or communication or consultation or care or specialist$ or monitor$ or virtual reality or virtual environment$ or technology$)) . tw. Contributions included coordinating the review, drafting the protocol, developing the search strategy, searching for trials, obtaining copies of the trials, selecting trials for inclusion, extracting data from the trials, entering data, performing the analysis, interpreting the analysis and drafting the final review. Daniel Schoene was involved in drafting the protocol, searching for trials, selecting which trials to include, extracting data from trials, interpreting the analysis and drafting the final review.
Maria Crotty was involved in the design of the protocol, the selection of the trials to be included (referee), the interpretation of the analysis and the design of the final review. Stacey George was involved in designing the protocol, choosing which trials to include (referee), interpreting the analysis and drafting the final review. Natasha A Lannin was involved in designing the protocol, performing the analysis, interpreting the analysis and drafting the final review.
Catherine Sherrington was involved in drafting the protocol, supervising and interpreting the analysis and drafting the final assessment.