Impact
of
ablation dose
in
the
treatment
of
thyroid
cancer
\ryith
I-l3l
Cholid Badri,
Dharma Gayo, Suryo Seto
Abstrak
Tuiuan
:
Untuk menilai keberhasilan terapi ablasi denganlodium-l3l
menggunakan dosis yang berbeda pa4a penclerita karsinoma tiroid berdiferensiasi baik yang telah menjaLani operasi tiroidektomi totaL àlau hampir total.Cara : Penelitian retrospektif terhadap 42 pasien yang dirawat di Rumah Sakit
Dr
Cipto Maigunkusumo antara tahun lgg3 - I996. Diberikan ablnsi dengan dosis 80 mCi dan 100 mCi pada kelompok pasien yang masing-masing terdiri dari 2l penderita. Sebelunr ablasi, dilakukan pemeriksaan dengan sidik tiroid dan seminggu sesutlah abiasi dilakukan sidik seluruh tubuh. penilaian keberlnsilart abLasidilakukan
3 buLan seteLah ablasi dengan pemeriksaan sidik seluruh tubuh dengan 5 mCi I-l 3I.
Hasil:
Keberhasilanterapiablasidengandosis I00mCiberbedabermaknadengan aoiisAOmCi, yaitu sebesar g5,7Vo clibandingkan dengan 57 vo (p = 0,04). Efek samping akut dijumpai sebanyakl9
Vo pada pemberian dosis 100mCi dan 4,8
vopada
tlosis g0 nCi. Sidik tiroid yang dilakukanI
minggu setelah ablasi menunjukknn metastasis sebanyak 19 vo dengan pemberian dosis 100 rnCi dan4,8
Vo dengan dosis 80 mCi.Kesimpulan
: Ablnsi
dengan dosis 100mCi
I-l3t
memperlihatkan hasilyang lebih baikdibandingkan dosis g0 tnCi dan tklak meningkatkan efeksamping pengobatan secara bermakna. Di samping itu ablasi dengandosis 100 mCi kemungkinan dapat lebih banyakmenentukan adanya metastasis
jauh
dibandingkan dengan dosis g0 mCi. .Abstract
Purpose : To evaluate the fficacy of ablation therapy using lodine- I 3
t with
twodffirent
doses on patients with well-dffirentiatetl thyroid cancer who had been operated upon with total or near-total thyroidectomy.Methods:
A retrospective study
was conducted on 42 patients admitted at theDr.
Cipto Mangunkusumo Hospital, Jakarta between 1993- 1 996. Thyroid ablation was performed with 80 mCi and 100 mCi on each grorp,onriring
of2l
patients respectively.Tlq,y6ir1 scan wa's perfotmed before ablative procedure, and followed by whole body scanning
or" *""k
oyt", the ablation.. Oytrcacyo1 ttrc treatment was evaluated three months after ablation therapy using whole body scanning with 5
mCi of
I- t 3 t .Results : The
fficacy
of ablation therapy with a dose of 100 mCi was 85,7 Vo, significantly bettertlnn
57 Vo with a doseof
g0 ntCi dose (p=0,04). Acute side effects were seenin
4,8 Vo with a doseof
l00 mCi anà 19 Vo oj patients witha tlose
g0mCi. Whole botl1, scanning performed one week after ablation therapy revealed I9Vo distant ntetastases with the dose of I 00 mCi as cotnpared to 4,g Eo with the dose
of
80 mCi.conclusions:ThyroidabLatiottwithadoseofl00mcil-131
showedabetterresultascomparecltoB0mCidose,assideeffectsrftlte treatnrcnt were not signfficantlydffirent.
Moreover, ablation therapy with a doseof 100
mCi
probably cou2l detect,iior"
,lirto,rt metastases as compared to 80 mCi dose.Keywords
:
Thyroid cancer, radioiodine treatment, ablation doseINTRODUCTION
Ablation
wirh radioiodine
(I-131)
is
ro
eliminate
thyroid
tissue remnantsin
thyroid
cancer patientsafter
surgicaltreatment.
Someretrospective studies
showed thattreatment
with
radioiodine
was the only bestprog-nostic indicator on free
of
diseaseinterval and
im-provement
of
survival rate
of well
differentiated
thyroid
cancer patients. l'2Department of Radiology, Faculty of Medicine {lniversity
of
Indonesia, Dr. Cipto Mangunkusumo Hospital, Jakarm, IndonesiaSurgery is the
primary
treatmentof
thyroid
cancer, andall follicular
andpaprllary carcinomas
with
a cllameterof
cm
-
1,5cm
are suggestedto
unclergotot
al thvroidectomy due to multicentricityof
-4Such aggressive
surgical
approachcould enhance
theability of
I-l3l
to
ablate
rheremaining gland and
rotreat distant metastases.
Residual thyroid
tissue
will
prevent
detection
of
local
dan
distant
metastases onfollow-up with
I-l3l
scanning.5no
Badri et al.have been evaluated
in randomized control
mannerfor
efficacy of
therapy.6'7Nevertheless,
there aretwo
dif-ferent opinions on
the dosagethat
should begiven
for
thyroid
cancerablation.
It
is
known
that
thelow
doseranges
from
30 - 50mCi
and thehigh dose
from
80- 150mCi
of
I-131.
Since
1990, at theDr. Cipto Mangunkusumo Hospital,
a doseof
80 mCi
hasbeen
usedfor
ablation
and the success rate achieved was58%
for
thegroup
ofpapil-lary type, and
J}Vofor
thefollicular
type. But, with
are-irradiation,
ahigher
success ratecould
be achievedas
high
as 6JVo and 80Vorespectively. Therefore, it
wasestimated that
a dose higher than 80 mCi would
be neededto
achievebetter ablation result.
According
toBeierwaltes,l0 the
effective
ablation
doseis
between100
-
150
mCi
despite reports
from
other
authorsshowins
that a
lower dose
was also effective
aswell.ll
Éasedon
these references,since
1993 someof
thepatients
wereirradiated
with
a doseof
100mCi
for
ablation
insteadof
80mCi.
The aim
of
this
study
is to compare
the efficacy of
the treatment
using
both
different
doses
and
its
toxicity
aswell.
METHODS
Data
were
collected-from
medical records
of
all
patients who underwent ablation
during
1997to 1996
at the Radiotherapy
Unit,
Dr.
Cipto
Mangunkusumo
Hospital.
Thediagnosis of thyroid
cancer wasroutine-ly confirmed
and
classified
according
to
the WHO
classification
atthe Department
of
Anatomic
Pathol-ogy, Faculty of Medicine
University of
Indonesia. Thefollicular
variant
of
papillary
thyroid
cancer
wascategorized into
thepapillary type, while
theHtrthle
type
wasput
into
thefollicular
one.Patients
who
cameto
theRadiotherapy Unit
generally
had been operatedupon previously
at theDepartment
of
Surgeryof
the sameinstitution
orfrom
otherhospi-tals.
The
determination
of clinical staging
was basedon physical examination, surgical
report,
his-topathologic examination and
on
the possibility of
metastatic
spreadto regional lymph
nodes or distant
metastases. TheTNM
svstem
was usedand based
on theUICC classification
of
1987.eThe subjects
were
all
patients who
fulfilled
the
in-clusion
criteria, consisting
of
a
well
differentiated
thyroid
cancer(follicular
orpapillary),
residualthyroid
tissue detected onpostoperative thyroid
scanning, had been on alow iodine diet for
morethan I
week and hadundergone total or near-total
thyroidectomy. The
ex-Med J Indones
clusion
criteria
werethyroid
cancerof other type
thanfollicular
orpapillary type,
poor generalcondition
andblood hemoglobin
lessthan
l0 gVo.
Post-operative
thyroid
scanning was performed with
1 mCi I-131, mostly
within 4 to
6
weeks after
thyroidectomy. The administration
of
substitute
hor-mone
after
surgery,
if
any,
should
be
withheld
2weeks
before the scanning.
If
residual
thyroid
tissuewas
still found on
the
scanning,
the preparation
for
theablative procedure
was started. Patientswere
sub-sequently put on
alow iodine diet
andwithheld from
the substitute hormone
for
about 2 weeks.
At
the endof
the preparation, laboratory
tests were performed
including
among others:
T3,
T+,
TSH,
serum
thyroglobulin, hemoglobin, leucocytes, and
throm-bocytes.The ablation
should
be
performed soon
after
thepreparation
wascompleted. During
theadministration
of
I-131,
the patientswereput into
anisolation room.
The patients were asked
to
drink
much water
and urinatefrequently
as amethod
tolower
radiation
doseto whole body
andparticularly to the bladder.
Urine
and faeces
were
collected
and treated as a
specialwaste.
Acute side effects,
if occurred, were
treatedsymptomatically
as needed.Body
uptake was measuredusing
asurvey meter, at
1hour
afteradministration of
I- 131 , and repeated48-72
hours afterwards. Patients were allowed
to
leave
thehospital when measurement
from 3
meter
distance gave afinding of
less than 0,37mR/hour.
Post-ablative whole body scanning
wasperformed
I
-2
weeksafter
theablation
tofind
out thepossibility
of
existing distant
metastases.After
whole body
scan-ning,
thyroid
hormone
wascontinuously given to
thepatients
as a suppressive therapy.Clinical follow-up
was doneregularly after
1week,
1month,
3months,
6months,
I
year,
andevery 2
yearsafter the ablation. Follow-up with whole body
scan-ning
wasperformed
using
a doseof
5mCi
I-131
, at 3months after ablation.
Table
l.
Distribution of age and histopathologic rypesAge
Histopathologic typesYear
Papillary
Follicular Total thyrodectomyI
-
3-4 weeks
I
Thyroid scanning
I
mCiI
Residual thyroid tissue
I-l3l
therapy (80 mCi or 100 mCi dose)l-
t
*""t
I
Whole body scanning
l-
3 monthsI
r
whorebodv'iu""'"t
t
"t
--l
Metastases
+
Residualtissue
Metastases-lll
100
/
I 50mCi
80/
I 00mCi
Follow-upTota
2l
-30
31-40
4l-50
5l
- 60>60
8 3
9 J 4
7 I 3 3 I
l5 4
[image:3.595.45.277.85.416.2]12 6 5
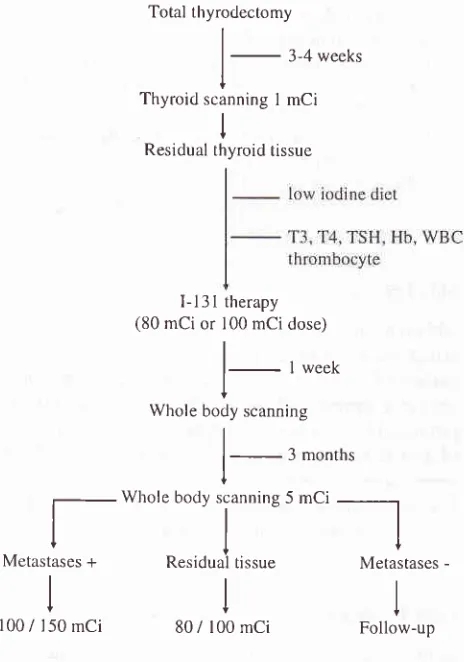
Figure
l.
Managentent of therapyfor
thyroid cancer with I-13l
at Rarliotlrcrapy Unit Dr. Cipto Mangwtkusumo HospitalRESULTS
Patient Characteristics
Among
42patients,
the mostfrequent
histopathologic
finding
was the
papillary
rype,
tbund
in
27
patients(64,3Vo).
Most
patients
( I5 out
of 42
parients,36
Vo) werein
the age groupof
2l-30year. Outof
all patients studied, the mostfrequent
were fèmale ,i.e.27
patients (64,3Eo)and in
this female group,
rhehisroparhologic
findings
were nearly
equal,
l4
of papillary
and
l3
of
tbllicular
type. There
were
l5
male patients
and
13(
86,67a) of
them
had
a
histology
of papillary
rype (p=
0,002).
Thusin
this study
thepapillary
rype wassignificantly
more
frequent
than
the follicularytype
in
themale
patients.The
distribution
of
age, sexand histopathologic
rypes are presentedin
Tables
I
& 2.
Table2. Distribution
ol
sex and histopathologic typesHistopathologic types Sex
Papillary Follicular
Male Female
The
Extent of Tumor
Among
42
patients with
awell differentiated
rhyroid
cancer
included
in
this study, the
highest number
of
cases
were
in
StageI,24
patients
(57Vo). The
otherswere
included
in
stageII,
5 patients(12 Vo)
and srageIII,
7patients
(l7Vo). Six
patienrs
(14 Vo)
were
clas-sified
into stage
IV
according to metastatic
lesions detected onwhole
body
scanning after
ablation.
Therelationship between
stagesand
histologic
finding
aswell
asrelationship
between
agegroups
and
stagcs are presentedin
Table
2and
Table
3.Table
3,
Relationship between stageand
histopathologic typesHistopathologic types
Stage olTumor Total
Papillary Follicular
I II
III
IV
42 l5
27
Tota
42
l5
27
l5 27 2
l3 t3
l4
24
5
7
6*
t02
2
I
t4 J 5 5
Total
172 Badri et al.
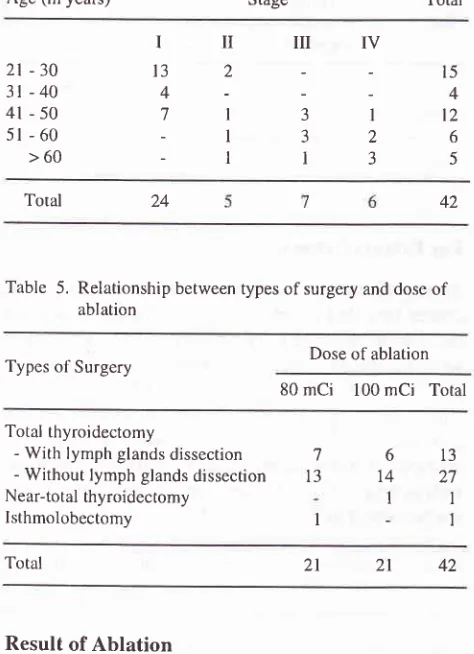
Surgery
The highest number
of
surgery
performed was
total
thyroidectomy,
with or
without
dissection
of neck
lymph
nodes (957o).In
this study,
I
patient underwenr
right isthmolobectomy.
Since
this patient
refused
toundergo
a
second surgery, an external
radiation
was addedto
the
neck
with
a doseof
50
Gy.
However,
even
after
the external
radiation
the
thyroid
scanningstill showed
uptake
of
I-131. Relationship
between typesof
surgery
with
dosesof
ablation is
presentedin
Table
5.Table
4.
Relationship between Age group and StageAge (in years) Stage
Med J Indones
-
successof
ablation
achieved was 807oin
males and 67Voin
females
(p>
0,05);
-
for
ageless than
45
years,
successachieved
was 79Vo, andfor
the
agegroup
of
45 years
andolder
was 57Vo
(p
>
0,05).-
based
on
histopathologic
findings,
success achievedfor
papillary
type
was 77Vo,and
63Vofor
follicular
type (p > 0,05);
-
success ratefor
StageI
was 75 Voas for
StageII-IV
was67Vo
(p >
0,05).Side
Effects
Ablationwith thedoseof 80mCi
produced
acute sideeffects
in
4 out
of
2l
patients
(l9Vo)
in
the form
of
nausea
in
I
patient,
dysphagiain
I
patient
and hoarse-nessin
2patients.
Ablation
with
the
doseof
100mCi
produced acute side
effects only
in
I
outof
21patients
(4,8Vo)
in
the
form of
neck
edema. Thesecomplaints
were taken care
off
with
symptomatic
therapy.
Cor-ticosteroid therapy
wasgiven
for
neck
edema, and thepatient
recoveredwithin
afew
days.DISCUSSION
In
this study,
thefactor
of
the doseamount resulted in
significant difference
of
ablation results.
A
dose
of
100
mCi
gave asuccess
rateof
86Vo,wh1le a doseof
80 mCi
gave
only
57Vo.Several results
of
previous
studies showed
that
a
high
initial
dose
of
I-131
will
improve
the
successrate
of ablation
and lessened the needfor
a repeat ablation.lo-12Beierwaltes
l3 suggested thatresidual
tissuewhich
still
took
I- 1 3I
in
thethyroid
bed should begiven
a doseof
ablation
no lessthan
100mCi. As
anadjuvant
therapy,a
dose
of
100-150
mCi
should
be
given
ro
ablatemicrometastases
unseenin
I-131 scanning
with
1-5mCi,
particularly
if
prior
toablation
tumor
uptake wasknown to
bequite low (<47o).to'ta
At
our
institution, the ablation procedure has
beenapplied
since 1987in
several patientswith
a doseof
30mCi. This
low
dose was chosen to makeit
possible
for
the
patient
to getambulatory
treatment since the wastetreatment
facility
was poor. One year later,
with
a better wastetreatment
facility,
the dose was increasedto
50 mCi.
In
1990,
a
general concensus
with
other
departments and
considering many
references
produced
aprotocol
for
ablation
with
a
dose
of
80mCi.
Total
21
-30
3t-40
4l
-50
5l
- 60>60
IIIIilIV
13
2
-
4-7t3l
-132
-l13
l5 4 t2
6
5
[image:4.595.49.286.276.603.2]Total
Table 5. Relationship between types of surgery and dose
of
ablation
Dose of ablation Types of Surgery
80
mCi
100mCi
Total42 24
Total thyroidectomy
- With lymph glands dissection - Without lymph glands dissection Near-total thyroidectomy
lsthmolobectomy
'l
l3
I
6 14
I
13
27
1
I
Total
Result of
Ablation
The
correlation
among sex, age, stage, typeof
surgery,histopathologic
finding,
dose
of
medication,
andfailure of
ablation was analyzed
statistically with
chi-square test and
Fischer
test.Evaluation of results
achievedin
thefirst
three months were asfbllows
:-
successrate
based
on
dose administered
for
100mCi
and
80
mCi
groups were
86Vo and
57?orespectively
(p < 0.04).
42
2l
On evaluation
of
patients treated
from
1990-lgg2,8
using the
doseof
80
mCi,
the average successrate
of
ablation performed on 44
patients
was
64Vo,with
ahigher
success rate onfollicular
type (7ÙVo) comparedwith papillary type (58 %).
Patients
who were
not
ablated
at the
first
treatment,
most
of
them
will
beablated on subsequent
treatment,
therefore the successrate
for
ablation could be improved
from
64Voto
79,5Vo.
This fact
lead
to
anassumption that the
dosegiven
on
the
first
ablation was relatively less
thanoptimal,
and
this
was also
in
accordance
with
Beierwaltes' opinion.who
suggested 100-150
mCi
asthe dose
fbr
ablation.lo
The present study showed
that
administration
of 100
mCi
ablation
doseresulted
in
asignificant
better
suc-cess rate
than
80mCi,
that
was 85,7Vo as compared to57Vo
(p=Q,Q!).
Thesefindings
were
found
to
have nosignificant correlation
between success rateofablation
with
thosevariables
such as age, sex,type,
stage andhistopathologic
type.Therefore,
radiation
with
a doseof
100mCi
wasbetter
than
80mCi
because the success rate washigher,
andthere was
no
needfor
thepatient to undergo
a secondablation.
It
can reduce daysofhospitalization,
shortenthe hypothyroid
period
in
ablation preparation,
andmay
also lessen the occurrenceof
metastasesbefore
asecond
ablation
wasperformed.
Ablation with
80mCi
dosecaused
side effectsin
4out
21 patients (l9Vo), those were
nausea
in
I
patient,
dysphagia
in
I
patient,
and
hoarsenessin
2
patients.With
100mCi
dose,side effects occurred
in
theform
of
neck
edema
in
I
patient
(4,8%).
Nausea
was
anearly
side
effect
of
I-131
therapy and lasted
from
Ihour
to
2
days,
and
responded
well
to
anti-emetic
administration.
Pain, uneasefeeling
and disturbanceof
salivary gland
production
were
early
complications
which
could
behandled
well.
Hoarseness
was
causedby
atemporary
edemaof
thesalivary
glandswhich
resultedin
pressure to therecur-rent nerve.
The characteristic
of
neck edema was seenas a
painful swollen neck, which
occurred
48
hoursafter therapy,
and wasrelated to invasion
of
tumor to
the soft
tissues
or
due
to
too much thyroid
remnant
left.l
Using
a doseof
100mCi
in
this
studydid
not increasequantitatively
side
effects
compared
to
a
doseof 80
mCi.
Qualitatively,
the side effectsfound in
the
group
given
a 100mCi
dosewas
aIittle
more grave, such asedema
of
the
neck,
but this
side
effect could
bemanaged
with
administration
of
corticosteroids.
As
the ablation
dose
of
80
mCi
used
in
this
study showed 4,8Vo metastases(l/21)
in
thebones,
the
100mCi
dose rev ealed 7 9 Vo of metastase s (4 I2l)
inc I udi n g3 metastases
in
the bones and 1in
thelymph
node. Thenumber
of
patient
with
metastaseswas
higher
in
theablation
doseof
100mCi
as comparedto
the doseof
80
mCi
(19
Vo vs4,8
Vo).The probable
causecould
be thefact
that metastatic depositsof carcinoma took
lessI-131,
thus
a
higher dose
is
needed
to
reveal
theactivity on whole body scanning.
Nevertheless,
thepossibility
remained that those patients
who
weregiven
a doseof
100mCi
hadin
fact distant
metastasesin
a greaternumber compared
to thegroup
which
wasgiven
a 80mCi
dose.There
are severallimitations
found
in
this study,
suchas
no
records were available about
the
size
of
thetumor, multicentricity, estimation
of
residual
thyroid
gland, TSH
blood
level before ablation,
andresults
of
follow-up on
ablation
for
the
first
three months after
ablation.
Thosevariables should
beconsidered
in
fur-ther
studiesof
the ablation
dose.REFERENCES
'L Varma
VM,
Beierwaltes WH, NofalMM,
Nishiyama RH, Copp JE. Treatmentof
thyroid cancer: Death rate aller surgery and after surgery fbllowed by sodium iodine I-l3l
.JAMA, 1970: 214: 1437 -42.
2. Mazzateni
EL,
Jhiang SM. Long term impactof
initial surgical and medical therapy on papillary and tbllicular thyroid cancer. Am JMed
1994; 97: 418-23.3. Ramli HM, Kamajaya. Penatalaksanaan karsinoma tiroid di Bagian Bedah Sub Bagian Bedah Onkologi FKUI/RSCM. Dalam: Keganasan kul'it leher dan kepala. Semarang: Badan Penerbit Univ. Diponegoro,
l99l;
185-200.4. Wanebo HJ, Andrews W, Kaiser DL. Thyroid câncer: solre basic considerations. Am J Surg
l98l;142
474-9. 5. Sweeney DC, Johnston GS. Radioiodine therapy fbr thyroiclcancer. Endocrinol Metab Clin North Am 1995; 72:828-32. 6. Maxon
III
HR, Smith HS. Radioiodine-l3l in the diagnosis and treatment of metastatic well differentiated thyroid can-cer. Endocrinol Metab Clin North Am 1990;l9:
685-71 87. Robbins J. Thyroid cancer:
A
lethal endocrine neoplasm. Ann Intem Medl99l;
I l5:133-9.8.
Badri
C,
KuswantoO,
GondhowiardjoS,
Astarto B, Kusumawidjaya H. Papillary and follicular thyroid câncer:Impact
of
treatmentin
44
patientsat the Cipto
Man-gunkusumo Hospital. Med JUniv
Indon 1994; 4 : 42-7. 9. Hermanek P, Sobin LH.TNM
classitlcationof
rnalignanttumors. International Union Against Cancer. 4th cd. Ncw
174
t0
Badri et al.
Beierwaltes WH, Rabbani R, Dmuchowski C, Lloyd RV,
Eyre P, Mallette S. An analysis of ablation of thyroid rem-nants with I-13 I in 51 I patients from 1947-L984:Experience atthe University of Michigan. J Nucl Med 1984;25:128'l-93.
DeGroot
LI,
Reilly M. Comparison of 30 and 50 mCi doseof
Iodine-l3l for
thyroid ablation. Ann Intern Med 1982;96:5 I -53.
Metl J Indones
12. Mazzafeni EL, Young RL. Papillary thyroid cancer:
A l0
year
follow-up
reportof
the impactof therapy
in 576
patients. Am J Med 1981; 70:511-8.13. Beierwaltes
WH.
The treatmentof
thyroid
cancer with radioactive iodine. SeminNucl
Med 1978; 8: 79-93. 14. Greentield LD, Luk KH. Thyroid. In: Perez CA, Brady.LW,eds. Principles and practice of radiation oncology. 2no ed. Philadelphia: Lippincott, 1992; 1356-81.