-.
Vol 8, No 3, JulY - SePtember 1999 T hre
e -dimensional ima g in g 201
Three
-
Dimensional
(3-D) video
imaging
as a
tool in pre-operative evaluation
of head and neck
tumors
Masrin Munir
Abstrak
suatu ameloblasloma'
Abstract
nding revealed an ameloblastoma'
Keyworils
:
Three-dimensionalvideo imaging' ameloblastoma' helical lomographyThe introduction
of
conventional computed
tomo-ultY of Medicine' nkusumo HosPital, Jakarta, Indonesia
Ameloblastoma
is
the most common
epithelial
odon-togenic tumors.
It was
recogniz,ed-by Cuzakin
1827 asquît"a
by
Mc
Daniel
RK.r
Other experts
said
ameloblasioma as
adamantinoma,
adamanblastoma'basiloma or epithelioma ameloblastoides'
Case
report
A32-year of
age malepatient
was admitted theDepart-ment
of
Otolaryngology,
Dr.
Cipto
Mangunkusumo
Hospital,
University
of
Indonesia on November
5,1997
with
the
chief complaint
of
alarge
masson
hisleft
mandible,
with 10x8x5cm
in
size(Figure
1).The
patient
was referredfrom Dharmais
CancerCenter
Hospital
with
a tumor
in
his
left
mandible since
15years.
Theinferior left
secondpremolar
and twomolar
teethwere
mobile
andwere
extracted.
Oneyear later
the
tumor grew
bigger, ruptured
with bleeding.
Four
[image:2.595.82.579.329.754.2] [image:2.595.331.577.362.644.2]years
after extracting
the teeth, thetumor
was resectedby
a
general surgeon
at
Pangkal Pinang Hospital
Sumatera.Two
years
later,
recurrencesoccurred
and thetumor
becamebigger.
Figure
I.
A 32-year male with a large mass on left mandible.Med J Indones
General
condition and other otolarynoglogical
ex-amination
were
within normal
limits.
No history
of
dyspnea, nor cough, nausea,
vomiting,
generalfatique,
anorexia
or
lossof weight. Laboratory findings
werewithin
normal
limits.
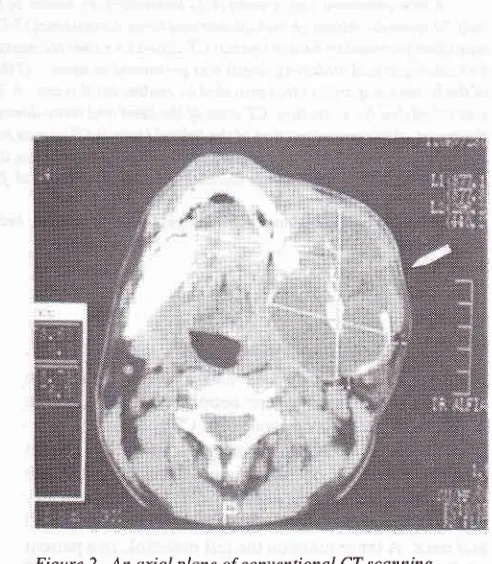
Conventional computerized
tomography
(CT)
scanning
with
andwithout
contrast
of
the head andneck,
was doneon October
24,1997,
with
sagital
andcoronal
section
of
5mm slices.
TheCT
showed
a
dense
mass
at
the
angle
of
the left
mandible.
A
wide
destruction
wasnoticed with
thin-ning of
thecortex of
themandible,
but noempty
spaceshowed
in
the
CT. A
mass oT73.6
x
66.3mm with
lateral enhancement was
seenon
the
CT
(Figure
2).Diagnosis
of
the
tumor
cannot
be madefrom
the
CT
scan.Vol 8, No 3, July - September 1999
[image:3.595.343.571.89.381.2] [image:3.595.81.313.100.379.2] [image:3.595.343.573.385.685.2] [image:3.595.81.311.480.683.2]Biopsy
was done
on November 6
andNovember
12, 1997with no
tumor
cell
seenin
thehistological
find-ings.
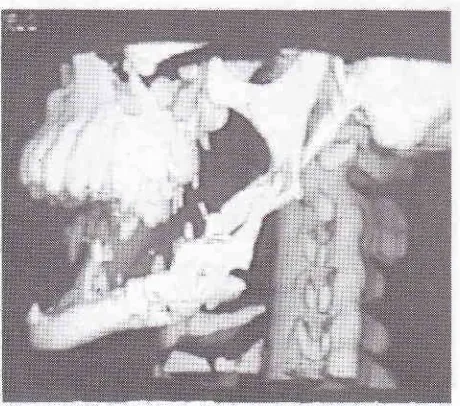
On November
24,
1997 athree-dimensional
(3-D)
imaging
by means
of
helical (spiral)
computed
Figure
3.
Caudal view of the head in a 3-D imaging of spiral CT showing enlarged left mandible, eroded with several holes in it.Figure
5.
Left lateralview of the headfrom a 3-D imagingof
spiral CT.
Three-dimensional
imaging
203tomography
of
the head andneck
r'vas donein
anotherhospital.
The helical (spiral) CT
reconstruction
showed a
tumor
onleft
mandible
with
separated holesin
thetumor
mass(Figures 3,4,5,6).
Figure 4. Proximal view of the head from a 3-D imagitrg
of
spiral CT showing enlarged mandible with the holes in the mass.
Figure 6. Anterior view of the headfrom a 3-D imaging
of
spiral CT.
Munir 204
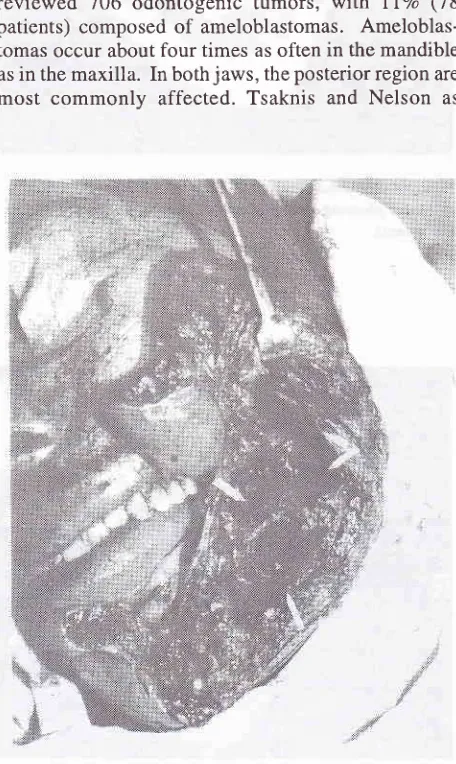
Surgical
treatment
of
the tumor
at
the
left
mandible
was done under general
anesthesiaon
December 20,
1997
with median
submandibular
incision
approach.A multilocular
cystic tumor
of
7 x 6 x 4 cmin
size wasexenterated,
followed by
curretage the
margin of
themandible (Figure
7).The histological
finding
of
the specimen revealed
anameloblastoma
with
follicular
pattern
of
squamousmetaplasia.
The patient was
discharged
without
anycomplaint
on December24,
1997. Three months aftersurgery, on
followed-up,
no recurrence was detected.
DISCUSSION
Ameloblastoma
Regezi et
al
as quoted
by
the
Daniel
RKI
in
1987,reviewed
706
odontogenic tumors,
with llVo
(78patients)
composed
of
ameloblastomas.
Ameloblas-tomasoccur
aboutfour
times
as oftenin
the mandibleas
in the
maxilla.
In bothjaws,
the posterior region are [image:4.595.86.314.305.687.2]most
commonly
affected. Tsaknis and Nelson
asFigure 7. Median submandibular incision of the exenterated tumor.
Med J Indones
quoted
by
Mc Daniel RK
claimed
thatof
24maxillary
ameloblastomas, 83 Vo (20 patients) were located at the
posterior part and the
meal
age was45.6 years. Dierks
EJ
and
Bernstein
ML'
in
1993,
claimed
that
ameloblastomas
may be
affected
in all
ages,but
the peak occurrences werein
thethird
andfourth
decades(-"un
age 40years). Miller
R.H er at3 in tgg6 quoted
that only 20Vo ameloblastomas occurredin the
maxilla,
usually
in
the region
of
the
third
molar.
They
may
however extended
into
themaxillary
sinus, nose,orbit
or even the base
of
theskull.*
The
clinical
manifestation of ameloblastomas is
aslow
growing,
painless
as themost
common
complaint
of
patients, even
the
tumor
is
in
advanced stage.''o'/
Typically, the early
symptoms are absent and
thetumors
aredifficult
to be diagnosed
in early
stagesof
development.
Other less common manifestations
aremobile teeth,
ill-fitting
dentures, malocclusion,ulcera-tion, draining
sinuses and nasal
obstruction.
Large
ameloblastoma
causescortical thinning,
perforation,
pathologic fracture
and soft-tissue penetration.Fi gure 8. Histopatholo gical finding showed ame loblastoma
Vol 8, No
j,
JuIy - September 1999Radiographically,
thetumor is
amultilocular
lucency,
with
no calcified or
radiopaque
components.
Other
radiographic spectrum is that, the tumors may
appearunilocular,
with
or without
association
with
atooth.
Two
predominant patterns
of
ameloblastoma
arefol-liculai
andflexiform.T'8 Of
th"
two
types, thefollicular
pattern
is more
common.
Cystic
degeneration
may occur in thecentral
stellate areaofthe follicles
and alsoin
the stroma.The
recurrence ratefor
ameloblastomastreated
by
exenteration
or
curretage
is
reported
to
be55
to
99percent.'
Pinsolle J" claimed that4l%o
of
4Opatients,
haslocal
recurrences.Large
ameloblastomas causecortical thinning
andper-foration, pathologic fracture
and soft-tissue
penetra-tion.
The
treatment
at
the primary site
for
an establishedmalignant
ameloblastoma, should not
dif-fer
from the
complete excision
for
an infiltrating
ameloblastomas.
Cases
which
have been found
to
metastasize,
retaining their
benign
histologic
pattern,are called malignant
ameloblastomas,
while
amelo-blastoma which
clinically
andcytologically
aremalig-nant,
are
termed
as ameloblastic carcinomas and
onthese cases
appropriate radical resection should
be undertaken.Three-dimensional (3-D) computed imaging
The introduction
of
conventional tomography
(CT)
scanning has had a
major impact
onevaluating
inflam-matory
andneoplastic
massesin
head andneck.
Thebasic
crosssectional
of
axial
imagesis
ableto
distin-guish
soft
tissuedensity
from fat
andtumor invasion,
deep to the
mucosal surfaces. Most recently,
theintro-duction
ofhelical (spiral) CThas dramatically
changedof
ability to
image the
oral cavity,-oropharynx,
hypopharynx,
larynx
andupper
airway.e
This
differs
from
conventional
CT
in
that the patient
is
moved
continuously through the CT
Scanner
during a
con-tinuous
*-.uy
"*po*t".
lo
The
basic
designfor
the3-D
system was developed atSt.
Louis
University
School
of Medicine
in
conjunc-tion with new Dimensional
Communications
Inc.
St.Charles,
MO.eThe 3-D imaging
can rotatecontinuous-ly
along any axis
of the airway
to
optimally
assessdisease. The
goal
of
3-D imaging
is
1.
to evaluate thequality
of
the 3-D
images,
2.
to
evaluate
to
what
degree
these images assisted
the radiologist
andotolaryngologist
in
judging
thelesion extend, relative
to axial
images
3. to
assesswhether there
is
any
dif-ference between
radiologists and
otolaryngologists
perceptions
of
the
3-D
images. The technological
ad-Three-dimensional
imaging
205vances
in
video imaging over the last
l0
years
haveresulted
in
remarkable additions
to
the
tools
of
otolaryngologists.e'10Currently,
3-D
imaging
isbeing
used
in
avariety
ofotolaryngologist in
head andneck
procedures." This
technique has also increased
thenumber of
surgeonability
toview
theoperative
proce-dures
aswell
asfor
permanent documentation
of
theprocedures.l2
^CONCLUSION
A
3}-year of
agemale patient
with
alarge
recurrencemass
of the
left
mandible,
is
reported. In this
case,conventional CT
scan and3-D video imaging
had beendone.
The 3-D video
imaging
showed,the
ameloblas-toma
consists
of multilocular tumor
with
septa
anddestruction of the
left mandible, while
theconventional
CT
scan
only
showed the extension
of
the
tumor
without
septa.
It
seem
that
it
is
difficult
to
detectmultilocular
ameloblastomaby conventional CT
scan.Although
conventional
CT-scandid not show
atumor
with
septa,this modality was
necessaryto
have
theinformation
about the size andextension of
thetumor.
The
histological
finding
of
thetumor
isameloblastoma
of
follicular pattern.
And
showed
the symptoms of
slow growing,
painlessswelling
with
high local
recur-rences.
This patient
already treated
for
several times
with
exenteration
of
the
tumor, but local
recurrences occurred aftersurgical intervention.
The lasttreatment
was
partial mandibulectomy
and exenteration
of
thetumor without
recurrence
after 3
months.
The
tumor
was located at the
mandible
as the mostclinical
featureof
ameloblastoma
while the radiographic feature of
ameloblastoma
is
that
of an
expansive,
multilocular
radiolucence tumor.
Clinical
andradiological
featuresare the same
with
that quotedby many
experts.ACKNOWLEDGEMENT
The author wishes to express his thank to
Dr. Bambang
Budyatmoko from
theRadio-Diagnostic
SubDivision,
Department
of
Radiology, Faculty
of
Medicine,
University
of
Indonesia,
Dr.
Cipto
Mangukusumo
Hospital,
Jakarta, Indonesia
to his
explanation
of
the3-D
Video
imaging photos
in this
article.
REFERENCES
206
Munir
2. Dierks EJ, Bernstein
ML. Odontogenic Cysts, Tumors
andRelated Jaw Lesions, In : Bailey BJ, Johnson JT, Kohut R.I Pillsburry
III HC, Tardi ME(eds).
Head and Neck Surgery-Otolaryngology. Philadelphia
: J.B. Lippincott Company,
1993.
II, p.
ll76
-91.
3. Miller RH, Sturgis EM, Sutton CL. Neoplasms of the Nose and Paranasal Sinuses.
In
: Ballenger JJ, Snow
JB (eds).Otorhinolaryngology Head and Neck Surgery. Baltimore, Philadelphia, Hong Kong, London, Munich, Sydney, Tokyo
: Williams and Wilkins, A Waverly Company; 1996, p. 194 - 205.
4. Montgomerry
WW.
Surgeryof
the maxillary sinus.In
:Montgomerry WW (ed). Surgery of the Upper Respiratory System. Baltimore, Philadelphia, London, Paris, Bangkok, Buenos Aires, Hong Kong, Munich, Sydney, Tokyo, Wroclaw. Williams & Wilkins; 1996,p.323 - 69.
5. Ballenger JJ. Diseases of the Oral Cavity. In : Ballenger JJ,
Snow JB (eds). Otorhinolaryngology Head & Neck Surgery. Baltimore, Philadelphia, Hong Kong, London, Munich, Sydney, Tokyo
:
Williams&
Wilkins,
A Waverly Com-pany; 1996, p.228 - 35.6. Pinsolle J, Michelet V, Coustal B, Siberchicot F-X, Xaver Michelet F. Treatment of Ameloblastoma of the laws. Arch Otolaryngol Head & Neck Surg; 1995,
l2l
:994 - 6.Med J Indones
7. Waldron C.A. Odontogenic Cysts and Tumors. In : Neville BW, Dam DD, Allan CM, Bouquot JE (eds). Oral &
Maxi-llo-facial
Pathology. Philadelphia,London,
Toronto, Montreal, Sydney, Tokyo : Saunder WB Company; 1995, p.511 - 70.8. Shah J.P. Bone Tumors (fumors and Cysts of the Jaws). In
: Shah JP (ed.). Head and Neck Surgery (2nd ed) Diagnostic Approaches, Therapeutic Decisions. Surgical Techniques
and Results of Treatment. New York, Philadelphia, Milan, Boston, London : Mosby-Wolfe;' 1996, p.523 - 52.
9, Maves MD, CooperMH, Benecke JE, YoungPH, Maas CS.
Three-Dimensional Video Imaging
in
Otolaryngology -Head and Neck Surgery. Laryngoscope 1993 ; 103 :lt74
-6. t0. Silverman PM, Zeiberg AS. Sessions RB, TroostTR, Zeman RK. Three-Dimensional Imagingof the
Hypopharynx andLarynx by means of Helical (spiral) computed tomography. Ann Otol Rhinol Laryngol 1995
;104:425
- 31.I
l.
Tsunoda A, Komatsuzaki A, Yamada M, Terasaki O. Three-Dimensional Computed Imaging using a Personal Computer for Nasal Surgery. Laryngoscope 1996 ; 106 : 584 - 8.12. Donnely KJ, Bank ER, Parks WJ, Gussack GS, Davenport
P, Todd NW. Three-Dimensional Magnetic Resonance