56
Adirama Med.l IndonesSmoking problem
in
Indonesia
Tjandra
Yoga Aditama
Abstrak
Kebiasaan merokok merupakan masalah kesehatan penting di Indonesia. Sampai 60Vo
pria
Indonesia dan sekitar 4Vo perempuan dinegara kita punya kebiasaan merokok. Kadar tar dan nikotin beberapa rokok kretek ternyata
juga
cukup tinggi. Selain dampak kesehatan rokok juga punya dampak buruk pada ekonomi, baik tingkat individu maupun keluarga. Dari sudut kesehatan, kendati data nrorbiditas dan mortalitas berskala nasional sulit didapat, data dari berbagai kota menunjukkan timbulnya berbagai penyakit akibat rokok seperti kanker paru, PPOK, gangguan pada janin dan sebagainya. Masalahnya lagi, kebiasaan merokok telah dimulai usia sangat muda di Indonesia. Pada tulisan ini disampaiknn juga hambatan-hambatan dalam program penanggulangan masalah merokok serta hal-hal yang perlu dilakukan untuk meningkatkan program penanggulangan yang ada. (Med J Indones 2002;l1:
56-65)Abstract
Smoking is an important public health probLem in Indonesia. Up to 60Va of male aduk population as well as about 4Va of female adult population are smokers. In fact, some of Indonesian kretek cigarettes have quite high tar and nicotine content. Besides health effect, smoking habit also influence economic status of the individuals as well as the family. In heahh point of view, even though reliable nation wide morbidity and mortality data are scarce, report from various cities showed smoking related diseases, such as Lung cancer, COPD, effect of pregnancy, etc. Other problem is a
fact
that smoking habit start quite in early age in Indonesia. This article also describe factors complicate smoking controL program as well as several things to be done to strengthen smoking controL progrant itt Indonesia. (Med J Indones 2002;II:
56-65)Keywords : smoking, I ndonesia, impact
The
Republic
of
Indonesia,
which consists of
approximately
17,000 islands, had apopulation
of 210
million;
it
is
the
fourth
most populous country
in
theworld atter
China,
India,
and
the United
Stateswith
hundreds
of ethnic groups and
language
/
dialectsbeing practices
in
the
country.
An
estimated
55.4million
persons(3lVo
of the
population)
were livingin
urban areasin 1990, compared
with
73.4
million
(36Voof
the population)
in 1997.t'23
All
of
these
factors complicate tobacco-control measuresin
Indonesia.Smoking
Pattern
Table
I
compiles
the
results
from
several studies
onsmoking behavior
in
Indonesia. The
percentage
of
current smokers among males
rangesfrom
30.2Vo toPuLmonology Department Faculty of Medicine University of I ndo ne s ia / P e r s ahab atan H o sp ital, J aknrta, I ndone sia
72Vo,
with
the
highest percentage belong
to
thedrivers
of public
buses
in
Jakarta.Among tèmales,
the percentage rangesfrom
I .5Voto
9.1Vo.The
Indonesian
Smoking Control Foundation
('LM
3")
compiled
a
meta-analysis
study
on
smoking
patternsin
Indonesia. laThe conclusions
of
the
meta-analysis studyperformed
by
"LM3"
included
the following:rl1.
The studies
found that
59.O4Voof
males over
ten yearsof
agein the
14provinces
in Indonesia were
currently
smoking.
Among
femalesover
10 yearsof a5e,4,837o were
culrent
smokers.2.
There was a negativecorrelation
betweenthe
level of education and the percentage of current smokers.3.
On
average,
cullent
male
smokers consume
almost
ten
cigarettes each
day, while
femalecuffent
smokers consumearound three
cigarettesVol. I I , No
l,
January-
March 2002 Smoking problem inIndonesia 5j
4.
Among both current
and
former
smokers,
males 7.
Clove-flavoured cigarettes
(kretek)
were the
or
females,
the fiequency
of
smoking was
still
favourite choice
of
smokers
in
Indonesia.
Forfairly mild,
less than
200
score indexed
by
male current smokers,
84,3l%o preferred
kretekmuftiplication of
number
of
cigarettes andlength
cigarettes,as
did'79,42Voof
the female smokers.of
smoking.
Similar
figures were
found in former
smokers, as5.
Ex-smokers generally reported smoking
higher
84,31Voof
the males and
7294Vo
of
the
femalesnumbers
of
cigarettes
than current
smokers.
In
preferred the clove cigarettes.males
it
was
13versus
l0
cigarettesdaily,
andin
8.
For both current
or
former
smokers,
the
age
of
fèmales
it
was more significant at 6.2
versus
3
smoking
initiation
were
quite
young.
Femalescigarettes
daily.
tend to start to smoke at the older age.6.
The
averageof
ouncesof
tobacco
per
week
was0.79 in current
users, andI.42in
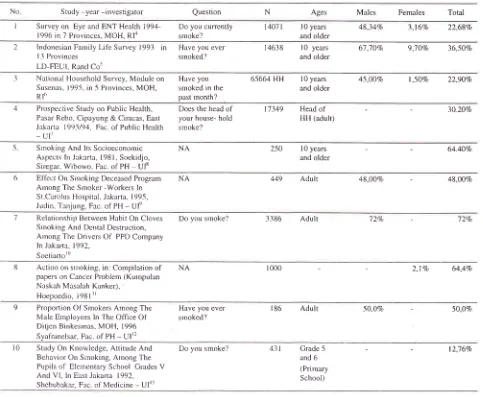
ex-users.Table
L
Percentage of Current Smokers in some studiesin
IndonesiaNo
S tudy -year-investigator
Question
N
Ages
Males Females
TotalI
Surveyon EyeandENTHealth1994- Doyoucunently
1407 Il0years
48,34Vo 3,l6Vo
22,68Vo 1996 in 7 Provinces, MOH,Rl4
srnoke? and older2
lndonesian Farnily Life Survey 1993in
Have youever
14638 l0 years
67,7OVo 9]0Vo
36,50Vo I 3 ProvincesLD-trEUl. Rand Co'
srnoked?
3
National Household Survey, Moduleon
Haveyou
6-5664HH
l0years
45,00Vo
I,50Eo
22,90Eo Susenas, 199-5, in -5 Provinces,MOH,
smoked inthe
and olderRl6
past lnonth?4
Prospective Study on PublicHealth,
Does the headof
'17349
Headof
3020VoPasar Rebo, Cipayung & Ciracas,
East
your house-hold
HH (adulQ Jakarta 1993/94, FacolPublicHealth srnoke?
-ur
and older
5
Smoking And ltsSocioeconornic
NA Aspects In J;rkarta, 1981, Soekidjo,Siregar, Wibowo. Fac. of
PH
UF2-50
l0years
64.40Voand older
6
Eifèct On Sntoking DecemedProgram
NAArnong Tlre Srnoker -Workers ln
St Carolus Hospital, Jakarta, I 995, Judin. Tanjung, Fac of PH
-
Ul'r7
Relationship Between Habit OnCloves
Do yousrnoke?
3386 Adult
72Vo
-
12VoSrnoking And Dental Destruction, Arnong TIre Drivers
Of
PPD Company ln Jakarlr, 1992,S oetiartor0
449 Adult
48,00Vo -
48,NVo8
Action on smoking, in: Comprlationof
NA papers on Cancer Problem (Kumpulan Naskah Masalah Kanker),Hoepoedio, l98lrl
9
Ploportion Of Srnokers ArnongThe
Have youever
186 Adult
50,0Vo -
50,OVoMale Ernployees ln The OfÏce
Of
smoked? Ditjen Binkesrnas, MOH, 1996Syalranelsar, Fac. of PH
-
UIr21000
2,17o
64,4Vol0
Study On Knowledge, AttitudeAnd
Do yousmoke?
431
Crade5
l2,76VoBehavior On Srnoking, Among
The
and 6Pupils of Eletnentary School Crades
V
(primaryAnd V[, ln East Jakarta
1992,
School) [image:2.612.50.533.294.691.2]58
AditamaThe
above datashow
no significant
differences
when comparedwith
theWHO
(1997) estimation, where in
Indonesia
the
prevalence
of
current smokers
wasreported
to be
53.0Voof
the males and
4Voof
the fèmales.But
it
should
be notedthat
theWHO
figures
werefor
people over the ageof
15 years.r-tThe
Indonesia Household
Health
Survey
in
1980 showedthat
about 54Voof
males and about 37oof
the f'emalesover ten years
of
age were regular
(daily)
smokers.
A
similar
survey carried
out
in
1986reported simrlar prevalence
rates (537oof
males, 4Voof
fèmales).Other
surveyscarried
outduring
he 1980sin
Lombok,
Jakarta,
and Yogyakarta
reported
maleprevalence
levels
of
75Vo, 65Vo,
and
67Vo,respectively, and
female
prevalence
levels
less
than 5Vo (exceptfor
Jakarta
where 9.8Voof
the females aresmokers).
Nationally, the
prevalence
of
smoking
isapproximately
607ofor
men
and 5Vofor
women.'7According
to
a
1985 survey
in
Semarang,
36Voof
doctors smoked, asdid'l9Vo of
paramedical personnel.Almost
all
(96Vo)of
the "peddle
rickshaw"
drivers
inthe
survey
smoked,
as did
over
half
(527o) of
governmentcivil
servants.A
1992survey
of
medical stuclentsrevealed
that 8Voof
males
and lVoof
femalèswere
daily
smokers,
while
39Voof
males
andl5Vo
of
females were occasional smokers.The Indonesian Household
Health
Surveyin
1995 wasone
of
the
biggest health survey
performed
in Indonesiawith
over
200.000 respondents.oAmong
itsfindings
were thefbllowing:
l.
The prevalenceof
smoking
in
the malepopulation
(10 yearsold
and above) were 457o(daily
smoker), 6.3Vo (occasional smoker) and 3Vo (fbrmer smoker).For the fèmale population, the figures were
l.5Vo, 0.57o and 0.270, respectively.2.
For
people
20
years
of
age and
above,
61 '27owere regular smokers,
and'7 .5Vowere
occasionalsmokers.
The
prevalence
in
urban areas
washrgher
than
the rural
areas,
and the
prevalence decreasedwith
higher
levelsof
education.3.
For
20 year old and
above,
4l.8Vo
of
the respondentsconsumed
1l-
20
cigarette
per
day, and 5.3Voconsumed
more that 21
cigarettes
per day.On
average, 3.9 cigarettes were consumedby
a smoker per day,or
1,421 cigarettes per year.4.
ln
urban
populations, 12.l7o
of
the
respondentsconsumed
filtered
cigarettes, 3Vo
non-filtered
c i garettes, 59 .8Vo smoked kr e t ek ci gat ettes, 20.8VoMed J Indones
smoked non-filtered
kretek
cigarettes,
O.3Vaconsumed cigars, 3.8Vo
rolled their own
cigarettes,and 0.17o smoked tobacco using
a
pipe.
Thecomparative numbers
for
the
rural
population
areas
follows:
11.6Vo, 2.8Vo, 33|7Va, 24.9Vo, O.6Vo,25 .4Vo and O.5Vo respecti vely.
Most
of
the tobacco
consumedin
Indonesia
is
in
theform
of
cigarettes, and between
85Vo and 90Voof
all
cigarettes smoked
in
Indonesia
are
kreteks.
The cigarettemarket
shareof
kreteks increasedfrom
about 30Voin
1914
to
about
90Voin
the
1990s. Since
theearly
1970s,
the per-capita adult (over 10 years of
age) consumption
of
cigarettes
(all
forms)
has
morethan
doubled,
from
500
to
I 180 per adult.
A
surveycarried
out
in
Jakarta
in
1981
estimated
that
eachsmoker consumed
(on the
average)twelve
cigarettes eachday.
About
5Voof
all
smokerssmoke more
than 20 cigarettes a day.Table 2. Consumption of manufactured cigarettes
Tar
levels
in
domestically
grown
Indonesian
tobacco arehigh.
In
1983, the average tarcontent
of
18 brandsof
kretek
cigarettes
was 58.0
mg
(range
41
-
11),while
the averagenicotine content
was2.4
mg
(range1.3
-
3.2).
These are substantially
higher
than
levelsusually
found
in
industrialized
countries.
About
73Voof
manufactured
cigarettes arefilter-tipped.r6
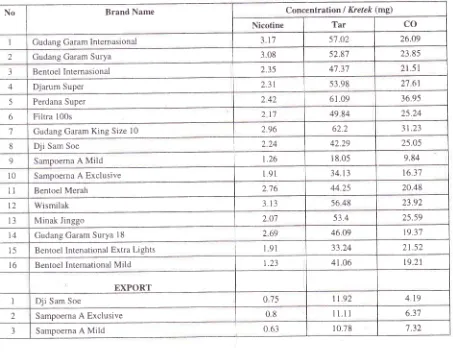
Table 3
shows
the tar, nicotine and
Carbon
Monoxide
(CO)
content
of
somekretek
cigarettesin
Indonesia.
It
isparticularly
interesting
to
compare
lhe
difTèrences inthe levels
of
the
domestic and exported products
of
the same brandsof
cigarettes.Production
and
Economic Impact
In
1990, 183,785
hectaresof
land were
set
asidefor
tobacco farmrng,
which
was down
from
288,000 hectaresin
1985.
Between lVo
and 2Voof
all
arableland
in
Indonesia
is
used
to
grow
tobacco.
Between1990
and
1992, Indonesia
grew approximately
2.OVoof
all
the
tobacco
in
the world.
In
1994,
Indonesiaproduced
about
180,000
million
cigarettes
(about-Vol I
l,
No 1, January-
March 20023.3Va of
the
world's
production),
which
wasup from
83,900 cigarettes
in
1980.
This
increase
in
cigaretteproduction is Iargely
a
reflection
of
the
dramaticincrease
in
the production
of
machine-made
kretekIn
1992, Indonesia imported 21,650
tons
of
rawtobacco
(accounting
for
l.4Vo
of all
imports), while
exporting
18,900tons (about
l.lVo
oTglobal exports)'
Indonesia
imported
15million
cigarettes and exported 15,000million
cigarettes,
or
2.27oof
global
exports.Table 3. Tar, nicotine and CO content of kretek
Smoking problem in
Indonesia
59In
1990,
the
costs importing
tobacco
leaf
andcigarettes amounted
to
US$ 42.1
million
(O.lVoof
all
import
costs), comparedwith uS$
17million
in 1985.
In
1990, Indonesia earned
an
estimated
US$
124.6million from
tobacco exports
(0.4Va
of
all
export
earnings), upfrom
approximately US$ 48.2
million
in
1985.
On the
other
hand,
Indonesian
cigarettesproduction could be
seenin
figure 1, which
showedthe
total
production
in
the
year
2000
was23'7,206,000,000 cigarettes
a year,
while
in
1995
it
w as 204,365,000,000 a year.No Brand Name Concentration I Kretek (rng)
Nicotine Tar CO
Gudang Garam Internasional 3 l'7 5'7.02 26.09
2 Gudang Garam Surya 308 52,87 23.85
3 Bentoel Internasional 2.35 47.37 21 .51
4 Djarum Super 231 53.98 27.61
5 Perdana Super 242 61.09 36.95
6 Filtra 100s 217 49.84 25.24
7 Gudang Garam King Size
l0
2.96 62.2 3t.238
Dji
Sam Soe 224 42.29 25.059 Sampoerna A Mild r.26 1 8.05 9.84
l0
Sampoerna A Exclusive 191 34.t3 t6.37u
Bentoel Merah 276 44.25 20.48t2 Wismilak 313 56 48 23.92
t3 Minak Jinggo 207 53.4 25.59
t4 Gudang Garam Surya 18 269 46.09 19.3'7
15 Bentoel Intenational Extra Lights 191 33.24 21.52
16 Bentoel International Mild 1.23 41.06 t9.21
EXPORT
I Dji Sam Soe 075 1t .92 4.19
2 Sampoerna A Exclusive
08
11.11 6.37 [image:4.612.47.500.285.638.2]'!
[image:5.612.52.280.101.249.2] [image:5.612.55.280.427.621.2]60 Aditama
Figure
l.
Indonesian cigarettes productionAbout
214,300workers were
engagedfÏll-trme in
thetobacco-manufacturing
industry
in
1989.
The Indonesiankretek industry ranks
asthe
second largestemployer
after
the
Government.
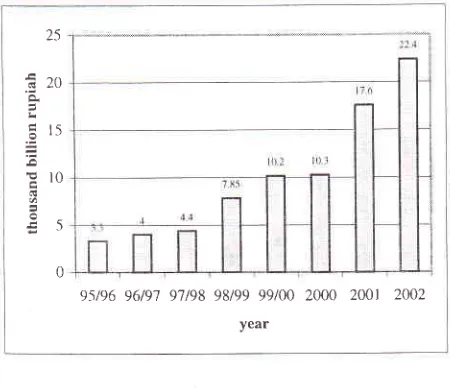
Figure
2
below
showed
tax
fee target
from
cigarettes,
which showed
that in 1995/1996it was
only
3.3 quintillion (thousandbillions)
,
in
2000
it
was
increasedto
10,3 thousandbillions and
in
2002
iT"was expected
to
be
22,4 thousandbillions
ruprah.25
Ëzo
L
É rç
= =
Er0
l!0
95196 96/91 97t98 98199 99/00 2000 2001 2002
year
Figure 2. Tax fee target
A
study
by
the
National Institute of
Health
Research&
Development
(Ministry
of
Health)
attempted
toanalyze the
economic impact
of
smoking in
Indonesia.With the
GDP per capita
in
1995 aboutUS$ 1,100,
it
is
estimated
that
the
macro economic loss
for
theMed J Indones
country
(government perspective) was
in
the amount
of US$
9,806,423,000
(almost
10billion
US
dollars)
or
about
50Vo
of
the total
annual
budget
of
theMinistry
of Health.
Economic
losses
due
to
tobacco
at
the
individual/
family
level
can bedivided
rnto:Direct
Loss:Indirect
Loss:loss
of
income
due
to
illness
and
ordisability
cost for
medical
treatmentloss
of
income
due
to
illness
and
ordisability
loss of income due to premature deaths
loss
of
income
of
family
members,due to
taking
careof
the patientsEstimated
economic loss
at community level fbr eachlung
cancerpatient
was asfbllows:
r
Average
cost formedical
treatment-- US$
738.00.o
Average number
of
absenteeismper year due to
hospitalization --
23 days..
Thus,
thelost income
dueto illness
for one patient
is 23X
US$
5.00--
US$
I
15.00.Loss
of income
of family
members (duetaking
care of the patients) is also equal toUS$ 115.00.'e
Health Impact
Reliable national
mortality
and morbidity data
are scarce.However, whatever
data areavailable
all
point
to an increase in the
major chronic
diseases associatedwith
smoking.
Estimates suggest
that
tobacco-attributable
mortafity
has risen
from
l-37o
of
all
deaths
in
1980
to
3-4o/oin
1986.
Thrs
suggests thatabout 57,000
deathseach
year (primarily
males)
arealready attributable
to
tobacco use, and
this
number can be expectedto
increasedramatically over
thenext
few
decades.'A
studyof
COPD
andsmoking
in East Java
province
found
that
1,546
men
(60.3Vo)
were
smokers
ascompared
to only 71
(1.8Vo)of
the women.
COPD
prevalence
was
l3.l
Vooverall. In
men
it
was
15.67o,and
in
women the prevalence
was
77.3Vo. However,
among
mde
smokers theprevalence
was
15.87o. Therelative
risk of
COPD
in smokers
was 1.02.
Smoking
and
impaired
PEFR (PeakExpiratory
Flow Rate) were
recorded
in
12.47oof
all respondents,
and the
resultsof the
testing correlated
well
with the results
from the
questionnaire.Risk of
impaired PEFR
in smokers
was 240,0(x)2_r0,ux)
220,(rx)
!
zro.rxxt.* 2(X),(XX)
r 90,(xx)
I 80,(XX)
Vol 1 1, No 1, January
-
March 20021.04.
Asthma was found
in
8Voat
all respondents,
while
its
prevalence
in
men was
9.67o,
in
women 6.4Vo, andin
male
smokersit
was 9.2Vo.The relative
risk
asthmain
smokers was 0.88.All smokers smoked
cigarettes;
none
of
them
professed
to
being a
cigar
smoker
and
only
one was
a
pipe
smoker.
Kretek
cigarettes
were
the
most
widely
smoked
type
of
cigarette
(61.57o).Only
270
(l'7.5Vo)
of
the
respondents
had stopped
smoking,
but
only
154
(57Vo)had done so
for
morethan
I
year,
and
only
I2.6Vo
of
clove
cigarettesmokers
have
tried
quitting.
Most
of
the
smokers (76.6Vo)can
be classified
as
light
smokers, smoking
less
than
10 cigarettes/
day.The
numberof
cigarettesI
male smoker
/
day
comes
to
6.7
cigarettes.
Theprevalence
of
smokers goes
up
almost
linearly with
age,
being
22.47oin
the
under
20
group
to
15.67oin
the
over-S0 group. Although paradoxically
almost40Vo
of
them
started
smoking
in
their late
teens(38.5Vo)
and
more
lhan
757obegan
to
smoke
before the age of 25 (77 .2Vo).2oIn
a
study
on smoking
and
lung
cancer
in
Jakarta,it
wasfound
that the relative
risk to
getlung
cancerfor
smokers
20
-
39
yearsof
age was 6.'76, and for thosewho
had
smokeclfor
more
than40
years,the relativd
risk
was
9.37.'fhey
found a significant
relationship
between
smoking
and
lung
cancer among
their
malerespondents,
but
not
among
the
females.
The
dose-responseimpact
was also discovered to besignificantly
u-àng
their
male respondent.2lAnother survey
in
1993 assessed
effects
of
passivesmoking
on pregnancy outcomesin
Jakarta.The
studyconcluded
that
odds
ratio
for
a
pregnant
women exposed to passivesmoking having
alow
birth-weight
infants
was2.3.22Smoking problem in
Indonesia
6l
Prevalence
Among Youth
A
1985 survey
of
primary
schoolchildren
in
Jakartafound
that
49Voof
theboys
and 97oof
the
girls aged
10-14
were
daily
smokers.
However,
a
study in
Jakarta
in
1990 reported
that
only
IVo
of
the 1l-14
year
olds,
9Voof
the15 year
olds,
and
67oof
the 16
year
olds
weredaily
smokers,although
thefigures
for
occasional smokers
were
157o, 22Vo,
and
44Vo,respectively. The latter study
also revealedthat9Vo
of
the
children
startedsmoking when under
l0 years old,
\Va at the age
of
ll,
l87oat
age I2,23Vo at age 13, and40Vo
at
age
14-16.The
vast
majority
(95Vo) smokedkreteks,
and 72Voreported
that their
parents
did
not
know
that they smoked.r3The meta-analysis study done
by "LM 3"
found
thatin
both
current
and former
smokers,
most
initiated
smoking between 10 and
29
yearsof
age; there
wasno
clear
difference between males
and females.
However,
the studydid
show thatmale
teenagers startsmoking earlier,
while
females tend
to
wait
to
try
smoking
at-terthe
age of 20,but all
were
at theyoung
group. This
was happenedin
the severity
of
smoking,which both
groups togethermajority
were
still
stay in themild
group,
l.e. less than 200.14This
study also concludedthat
teenager smokers werefound in
the proportion ranged
from
l2.8Va
to 2'1,'lVo
in
males, and among females were
O.64Voro
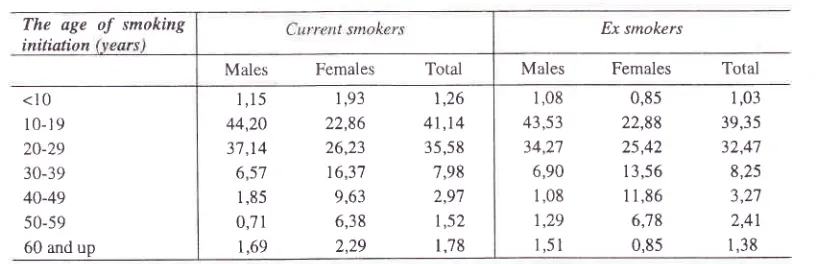
lVo.Either
in
current or
ex-smokers
the
age
of
smokinginitiation
were quite
young, since
the
highestproportion
wasfound
in l0
to
lessthan 30
years old.In
malesthere
were
8l,34Vo
of
current smokers,
and 77,80Vo ofex
smokers,while in
femaleslooked
likely
to
be
lower,
49.O5Voof
current smokers, and
48.30Voof ex
smokers. Femalestend
to
start
to
smoke at
theolder
age.Table
4.
The Age of Smoking Initiation among SmokersThe age
initiation
of smoking
Ex smokersMales Females
Total<10 10-19 20-29 30-39 40-49 50-59 60 and up
1,08 43,53 34,27 6,90 1,08 1,29
1 ,51
0,85 22,88 25,42 13,56 1 1,86 6,78 0,85
1,03 39,35 32,47 8,25 ? ?',7 2,41 1,38
Males Females
Total1,15
1,93
1,2644,20 22,86
41,1437,14 26,23
35,586,57
16,37
7,981
,85
9,63
2,970;71
6,38
t,sz [image:6.612.84.502.582.714.2]-l
62 Aditama
The
Indonesian
Household Health Survey
1995found
that
the
youngest
ageto
start smoking was
5 yearsold.
While
afair
number
of
respondents startedsmoking between
the
agesof
10and
14 yearsof
ageor
between
21
and
25
years
of
age, most
of
therespondents
started
smoking between
15 and
l9
years
old. Only
a
very
small proportion
of
therespondents started
smoking
between
26 - 30
yearsold.6
Another survey
by
the
University
of
Indonesiashowed
that young adult men (when
compared
toyoung
adult women)
are
far
more
likely
to
usesubstances
that
increase
health risks. For
example,8l
.lVo of young adult men
have smoked
cigarettescompared
to only
8.)Voof
women.
Similarly,
21.9Voof
men say they have
drunk alcoholic
beverages(compared
to
only
7.0Vo
among women), and
ahistory
of
recreational
drugs was reportedin
8.5Voof
the men and
only
0.5Vofor
women.
In
general,
theconsumption
of alcohol
andrecreational
drug
use ishigher
among
older
respondents (aged
20-24
yearsof
age),in
urban
areas,and among the more
highly
educated.
In
contrast,
does not vary
significantly
Med J Indones
with
age, urban ys.
rural
setting, and
their level of
education.
While
menwho
have beenmarried report
higher levels
of
smoking and
drinking,
single
malesare
slghtly
more
likely
to
have used
recreational
drugs (8.6%
of
single
men compared
to
'7.2Voof
married men).
When
askedif
smoking,
drinking,
and
drug
use
areharmful activities, nearly
all
respondents
said
yes.Many young
adults
who
are
using
these
substancessay
they would
like to
stop.
Among youth who
arecurrently smoking,
83.2Vowould prefer to give
up thehabit. Young adult
smokers
who were
interviewed
are
quite
heavy consumersof
ci
arettes; men average7.6
ctgarettes andwomen
3.7ci
arettes eachday.'''
Another
survey
in
Bali
found that
15Voof
primary
high
school
students(14-15
yearsold)
are
smokers.Data
from
1219 primary
and
secondary
school
in
Bandung
(1998) showed
that
32,33Vo
had
trredsmoking,
andthat
12.3Vo aredaily
smokers.Another
survey
on
streetvendor
children
in
I998 found
that18.217o
of
those
children
are smokers
in Semarang
and 58Vo
of
themin
Bandung.2aTable
j.
Smoking attitucle2lSex of Respondent Total
Male Female
Do you thinks smoking is harmful?
Total Respondents:
Have you ever smoked?
Total Respondents:
Are you just "experimenting?"
Total Respondents:
Do you smoke now?
Total Respondents:
Do you want to stop smoking?
Total Respondents:
Have you tried to stop smoking ?
Total Respondents Yes No Yes No Yes No Yes, regularly Yes, sometimes
No Yes No Yes No 9'7.\Vo 2.2Vo 42t9 8l.9Vo 18.lVo 4221 3'7.8Vo 62.2Vo 3456 '78.2Vo 20.5Vo l.3Vo 2152 83.lVo l6.9Vo 2122 85.jVo 15.ÙVo r763 96.8Vo 3.2%
3 854
8.jVo
92.jTo
3 858
89.4Vo 10.6% 308 t'7.9% 44.40k 37.'7Vo 33 94.3Vo 5.7Vo 20 87.9% 12.lVo 19 97.3Va 2.t10 8073 46.6Va 53.4% 8079 42.1Vo 57.9Vo 3'764 77.3Vo 2O.9Vo 1.8Vo 2185 83.2Vo 16.8Vo 2143 85.OVo 15.OVo
Vol I
l,
NoI,
January-
March 2002A
survey was conducted
by the
Indonesian Smoking
Control
Foundation
("LM3")
to
determine
thesmoking pattern among children street vendors
in
Jakarta.
This
survey interviewed 250 street vendors
in
Jakarta,
all
below
14 years
of
age.
20.27Voof
thesechildren
sell cigarettes.9.57Voof
thesechildren
startedsmoking
before the
age
of
10
years,
25.36Vo startedbetween
l0 -
1I
yearsold,
52.63Vo start smoking ar 72-13 years
old and
14.447o startsmoking
at
14 yearsof
age.
Of
thesestreet vendor
children,
40.67oof
themsaid
they
planned
to
continue smoking
in
the
future.Their
reasonsto start smoking were
"for fun," it
"tastesgood," "proud"
to
be
smoker,
and
to
feel
"macho."
54.9Vo
of
the respondents consumed less
than l9Vo
of
their
income
to
buy
cigarettes,
37.74Va respondentconsumed l0-20Vo
of
their
income, 5.037o
consumed21-30Vo. 1.89Vo consumed 31-40Vo
and
1.26Varespondent consumed
more than
40Voof
their
incometo buy
cigarettes. 7'7Voof
thegroup actually
felt
afraidthat
their
parents
would learn
that their
childrensmoked cigarettes. 86.98Vo
of
them knew that smokingwas dangerous,
but only
40.60Voof
them
felt
that
hadany current health problem
related
to
their
smokinghabit.
Of
these, 71.087o experienced
coughing
and12.05V0
described
dyspnea.
About
70.91Vo of
respondents said that almost
all
street vendor children,are active smokers.2-5
Another
preliminary
non
random survey
by
theIndonesian Smoking Control Foundation
("LM
3")
focused
on
stLldentsfrom
one
of
the top-ranked high
schools
in
Jakartanamely
SMUN
8. The
respondentswere
95
students,of
which
on]ly 7.4Vowere smokers
and 6.3Vo
were
former
smokers.On the other
hand,it
is estimated
that the smoking prevalence
in
other high
schools
is
much higher
compared
to
thrs
finding.
A
similar survey was also conducted
on
senior
yearmedical
and dentist
students,
with 71
respondents;5.6Vo
of
them are
current smokers,
and another 5.6Vo'are
former
smokers.In
contrastto those
data, a surveyon
students
at a
nursing
academy
found that
only
1.lVo
of
these students areactive smokers,
and 4.3Voare
fbrmer
smokers. Lessonsin
schoolwere
felt to
bemost important source
of information
about the harmfuleffêcts
of
smoking
by
4l.5%o
of
the high
school students respondents, 48Vo medical and dentist studentsand 38.2Vo
of
nursing
academy students.This
surveywill
be continued and extended in the near future.A
survey
on
the
knowledge
and
attitudes
aboutcigarette smoking among schoolchildren
in
centralJakarta concluded that:27
Smoking probLem in
Indonesia
63l. The
basic
knowledge concerning
cigarettesmoking
of
schoolchildren
jn
the slum
and
non-slum
areasof
Central Jakarta
is
sufficient, but it
needs to be broadened.2.
Theattitude
of
schoolchildren
in
both the slum
andnon-slum areas
of
Central Jakarta
is
generallyagainst ci garette smoking.
3.
Advertisements,
through
television,
radio
andother public media
(posters, banners, billboards)
are
the
most
persuasive sources
of
information
used to promote cigarette smoking.
Efforts
shouldbe
made
to
eliminate these
media
from
theschoolchildren's surroundings, especially
in
theneighbourhood of the schools.
4.
Educational programs
on
television
and
direct
participation
by
healthcarepersonnel
are the mostimpressive
sourcesof
information
concerning
thehazards
of
smoking,
but
at the present
time,
theseaddress
only
a
very limited
audience.
Efforts
should be made
to
increase therole of
educationaltelevision
programs
and
the
use
of
healthpersonnel
asthe source
of
information
concerningthe hazards of cigarette
smoking.
5.
The roleof
friends,
families
and school teachers assources
of information
on the hazards
of
smokingis still
very limited.
Efforts
should
be
made
toincrease
the
role
played
by
thesegroups
for
themto
become
more effective
in
delivering the
non-smokrng message.
Social activities at the
schoolssuch
as
non-smoking gatherings
with
parents,teachers,
and
students
should
be
encouraged
topromote the idea
of non-smoking.
6.
Radio
and printed media are very under-utilised assources
of
information concerning
smoking
hazards.
Attractive
programs
for
children
need
tobe
designed
so
that
children
can
get
accurateinformation
about the
harmful
effects
of
cigarettes and smoking.Summary
Smokrng
is
an important problem
in
Indonesia.
Thesmoking prevalence
in
male
population is
more
then6OVo.
The relatively
low
prevalence
rate
in
female(about 5Vo)
may
be
due
to
traditional
socialrestrictions,
but
it
is
safeto
assume that the smokingprevalence
in
w_omenwill
be
increasing
in
the
nearfuture.
Up to
30Voof
male
teenagers
smoke.
Themajority of
smokers start smoking between 15 and 2064 Aditama
young
as5
years
old. Kretek
clove cigarettes
are the mostpopular type
consumedby
smokersin
Indonesia.In fact, most
of these
kretek
cigarettes havevery high
tar and
nicotine
content.At
least
five
factors
complicate smoking-controi
programs
in lndonesia
One,
it
is estimated that about
12million
people
aresupported
by tobacco-related industries. This
includestobacco
and clove
farmers,
workers
in
tobaccofactories, the
distributors,
shops andall
theway down
to the
children
streetvendors;
and one must addall of
their families. Second,
the cigarette industry
is
animportant source
of
tax
revenuesfor
Indonesia.
Theincome that the government receives
will
surely be
aimportant consideration
while
making any
policies
regarding
to smoking-control
programs.Third,
there
is
insufficient
scientific
research
onsmoking
and health
in
the
Indonesian population.
Most doctors and health professionals use literature
from
abroad
when
designing
health-educationactivities.
Discussions
with
respectful
medical
specialists
found out that there
arequite few
researchbeing
done
in
the
field
of
smoking
and
health.Furthermore,
since colrlmon infections and
tropical
diseases
are
still
very
prevalent
in
Indonesia,
they(probably understandably) receive
more attention
compared to research on tobacco and health.
Fourth, smoking
is
socially
accepted
by
mostIndonesians.
"Cigarette money"
is a
slang
phrasecommonly used
for
giving
somebody
a tip.
During
social gatherings,
in
urban as
well
as
in
rural
areas,cigarettes are
usually
served.Asking
somebodynot
tosmoke
is
still
sometimes considered
impolite
or
perhaps
even "foreign" behavior. Fifth, the political
commitment from
decision
makersin the
governmentis not yet strong enough.
To
strengthen
the
smoking-control
program
in
Indonesia, several things are needed.
First,
healtheducation
for
the
general
public
is
very important.
Many
kinds
of
public
media
must'be
used,
sincecigarette advertising
is actively using all of
them.
In
fact, the knowledge
of
the general
population
aboutsmoking
is still
quite limrted.
In
most medical
andnursing school
cuiricula,
there
areno special
classesfor
smoking
and health. Improving the knowledge
about
smoking, its impact on
health, the economy andthe many other
aspectsof
the problem would be
anMed J Indones
important
first
step
toward
an
effective
smoking-control program in
Indonesia.Secondly,
every
segment
in
the
society must
beorganized
andutilized
optimally.
Government has
aresponsibility
of
coordination
and
regulation,
andprofessional organization and NGOs can and
alreadyplay important roles in any srnoking-control
program.ln
fact,
they
can play even more effective roles
if
allowed to work in
aconducive environment.
Third, regulation and laws
in
the
field
of
smoking
should
be
enacted
and
firmly
implemented.
Theseregulations
should
at
least include policies
onadvertisement,
tar
and
nicotine
content,
defining
smoke-free area, tobacco
tax
and fiscal
issues,protection
for vulnerable groups (such
aswomen
andchildren), etc. Many
considerations
must be keep in
mind, but
in
the end,
it
is the health
of the people of
Indonesia
who
should receive the highestpriority.
Fourth, especially
for
a tobacco and clove-producing
country like
Indonesia, adiversification
of
the tobaccoindustry should
be started.
There must be a way
tofind a
smooth transition
betu'een
the
tobacco-dependent
economy
andone which is healthy. Fifth,
political commitment from
government and parliamentshould be
encouraged. They play
acritical
role in
thedecision-making process
in
the country. NGOs
andother public
organization should lobby
hard to obtain
this important
political
commltment.
Sixth, there are
still
much
to
be done
in
the
field
of
research.
Epidemiological
research must beimproved.
Indonesia
is a
huge country
with
more
than
200million
inhabitants in hundreds ethnic
groups
spreadover
17,000 islands. Specialepidemiological
techniquesare needed
to obtain
reliable data that
represents thewhole country.
The health-related economic
researchis
also needed.
"Money talks," and
having
goodinformation
will
accomplish
alot in
discussions abouteconomic
policies.
International collaboration
can,
indeed,
play
animportant
role in
smoking
control.
This
kind
of
collaboration
does
not
only cover
researches,but
it
also
servesas a
kind of
bench-marking
of
activities
between
countries
in
various
aspects
of
their
respective smoking-control programs.
Success storiesfrom
one
country
could
provide motivation
for
neighboring
countries. On the other hand, failure of
I
Vol I
l,
Nol,
January-
March 2002example
for another.
Smoking is, after
all,
a
global
problem, and
only a
global solution can
effectively
deal with
it.
Acknowledgment
The
authorwould like
to
rhanksDr John W Aldis MD
for
his
valuable advice
rn
the
presentation
of
this article.REFERENCES
i.
Central Bureauol
Statistics. Demographic and HealthSurvey I 997. Jakarta, Central Bureau of Sratistics, 1 998: I-3
2.
National Household Health Survey 1992 (lndonesian).Jakarta,
NIHRD Ministry
of
Health Republic
oflndonesia,1992
3
Internatjonal Medical Founclationol
Japan. SEAMIC Health Statistics 1998. Tokyo, IMFJ, 1998.4.
Ministry
of
Health Republicof
Inclonesia. Survey onEye and E-N-T Health 1994-1996 in 7 provinces, MOH,
RI
(lndonesian). Jakarta:NIHRD Ministry
of
Health Republic ol Indonesia, 1 996.5.
Ministry
of
Health Republicof
Inclonesia. IndonesianFamily
Lifè
Survey 1993in l3
Provinces (lndonesian). LD-FEUI, Rand Co, 1993.6.
Ministry
of
Health Republicof
Indonesia. NationalHousehold Survey, Module
on
Susenas,1995,
in
5 Provinces (lndonesian).NIHRD Ministry
of
HealthRepublic of lndonesia, 1996
l.
FKMUI.
ProspecLive Studyon
Public
Health, pasarRebo, Cipayung
&
Ciracas, East Jakarta: (Indonesian). Jakarta: FKMUI, 1993194.8.
NotoatmodjoS, Soekidjo, Siregar
KN,
Wibowo
A.Smoking habit and its socioeconomic aspects .in Jakarta
(lndonesian). Jakarra: FKMUI, I 981.
9.
Tanjung, Judin P. Effect on Smoking Deceased programamong
the
smoker-workersin
St.Carolus HospitalJakarta (Indonesian). Jakarta: FKMUI, 1995.
10.
Soetiarto, Farida. Relationship between habit on clovessmoking and dental destruction, among the drivers
of
ppD company in Jakarta (Indonesran). Jakarta,F
tJl j992.11.
HoepoedioRS. Action
on Smoking: Compilation of
pâpers on Cancer Problem (Indonesian). Jakarta: 1981.
Smoking problem in
Indonesia
65Syafranelsar. Proportion
of
Smoker amongthe
male employees in the office of Ditjen Binkesmas (Indonesian). Jakarta: FKUI, 1995.Shehbubakar, Sukaenah. Study
on
knowledge, attitudeand behaviour
on
smoking,among
the
pupils
of elementaryschool
gradesV
andVI
in
East Jakarta(Indonesian). Jakarta: Faculty of Medicine, University of Indonesia, 1992.
Indonesian Smoking Control Foundation. Meta-Analysis
Smoking
Pattern
in 14
Provinces
in
Indonesia(lndonesian). Jakarta: Indonesian
Smoking
Control Foundation("LM3"),
1998.National Household Health Survey 1980 (Indonesian).
Jakarta:
NIHRD Ministry
of
Health
Republic
ofIndonesia, 1980
World Health Organization. Geneva, Tobacco or Health:
A Global Status Report. World Health Organization, 1997.
National Household Health Survey 1980 (Indonesian).
Jakarta, NIHRD Ministry
of
Health
Republic
ofIndonesia, 1980
Aditama TY. Tobacco and Health (lndonesian). Jakarta,
UI Press I 997.
Kosen
S.
Analysis
of
Current Economic
Impact(Government and Community Perspective)
of
Smokingin
Indonesia. Jakarta:A
Report Submittedto
WHO Indonesia.NIHRD Ministry
of
Health
Republic of Indonesia,1998.Benyamin
M.
Smoking:An
East Java COpD Survey.Surabaya: Department
of
Pulmonology
AirlanggaUniversity School of Medicine, 1990.
Suryanto
E,
Yusuf A, HudoyoA.
Smoking and LungCancer (Indonesian).
MKI
1986: 36: 369-74.Tanuwijaya S. Youth Epidemiology Problems (Indonesian). National Congress of Pedi atrici an. Jakarta, I 999.
Demographic Foundation,
University
of
Indonesia.Reproductive Youth Health (Indonesian). Jakarta, I 992. Adisasmita A. Efïect of Passive Smoking on pregnancy
Outcome (Indonesian). Jakarta: FKMUI, 1993.
Wijayata
M.
Smoking Patrern Among Street VendorChildren
(Indonesian). Jakarta, Indonesian SmokingControl Foundation
("LM3"),
I995.'landra
YA.
Smoking Habit in High School, Denral andMedical School
(Indonesian).Jakarta,
IndonesianSmoking Control Foundarion
("LM3"),
1995.Shebubakar,
Jusuf A.
The Knowledge ancl
Attitude Concerning Cigarette Smoking Among Schoolchildren in Central Jakarta. Jâkarta: (lndonesian), Department of Respiratory Medicine, Faculty of Medicine, University of Indonesia,1992I2
14
l3
l7
21. l5
l6
l8
t9
.A
22 23 14 25
26