Vol9, No
l, January
- March2000 Experience in lung cancer treatment 43Experience of treatment of lung cancer
patients using paclitaxel and
carboplatin
Anwar
Jusuf
*,
Sutji
Astuti Mariono**,
Karmel
L.
Tambunan*,
A.
Harryanto Reksodiputro*, Noorwati
Soetandyox,Ronald Hukomx, Eddy
Suratmanx,A.
Mulawarman
Jayusman*Abstrak
Sembilan belas pasien kanker paru jenis karsinoma bukan sel kecil stage
III
&N mendapat kemoterapi dengan paduan paklitalcsel
dan karbopl.atindi Rumah Sakit Kankcr Dharmais
dan Rumah Sakit Pusat Pertamina Jalcarta,terdiri dai
14laki-laki
dan 5 perempuan. Diagnosis histologisinlah
adenokarsinomapada
13 pasien, knrsinoma skuamosa pada 4 pasiendan
knrsinoma adenoskuamosa padaI pasien. Empat
belas pasien termasuk stage IV, stage IIIB terlihat pada 4 pasien dan stage IIIA padaI
pasien. Paduan obat terdiri dari paklitaksel, dengan dosis 135-200 mg/m2 dan karboplatin 300 mg/m2 atau AUC 6 mg/ml.min, diberikan melalui infus setiap 3 minggu, paling sedikit 3 sikLus. Pasien diikuti secara teratur sampai meninggal. Respon objektif berupa respon parsial (partial response) terlihat padaI2
pasien (63Vo), 2 pasien tidak menunjukkm perubahan (stable disease) dan perburulan terlihat pada 5 orang (26Vo). Dua pasien masih hidup masing-masing 22 dan 23 bulan setelah kemoterapi dimulai. Masa tahan hidupI
talun adaLah 587o dan masa tengah tahan hidup ialah l4 bulan.Abstract
Nineteen patients with stage
III
& IV nonsmall cell lung cancer were fteated with regimen containing paclitaxel and carboplatin at Dharmais National Cancer Center Hospital and Pertamina GeneraL Hospital, Jakarta- Indonesia. There were 14 males and 5
females, the histologic diagnosis being adenocarcinomain 13 patients, squamous
carcinomain 5
patients and adenosquamouscarcinoma
in 1 patient. Fourteen patients were
in
stage IV,4
had stage lllB, one had stage IIIA disease. The regimen contains paclitaxel 135-200 mg/m2, combined with carboplatin 300 mg/m2 or AUC 6 mg/ml. min, given every 3 weeks. Those who underwent at least 3 cycles of chemotherapy were followed up until death. Objective improvement (partial response) was seen in 12 patients or 63Vo; 2 had stabLe disease ( I IVo) and 5 had progressive disease (26Vo). Two patients are still alive at 22 months and 23 months after starting chemotherapy. The one year surttival rate was 58Vo and median survivaL time was I4 months.Keywords : nonsmalL cell carcinoma, chemotherapy, paclitaxel, carboplatin
The
treatment
of
lung
cancer
hasbeen
a problem
in
Indonesia.
In
Dharmais
National
Cancer
CenterHospital, 541 lung
cancer patients
were
hospitalized
during
1993-1997,
344
of
them were nonsmall
cell
lung
cancer
in
stageIII &
IV.
Chemotherapy
shouldhave been indicated
for
them,
but
mainly due
tofinancial reason
only 54 of
them could
be so treated.
In
spite
of
such
a
situation,
a
small number
of them
were able toprovide cytostatic
drugs for themself.Paclitaxel
in
combination
with carboplatin were among
of
the regimens that werechosen
for
these
patients. In*
Dharmais NationaL Cancer Center Hospital, Facultyof
Medicine, Universityof
Indonesia, Jakarta, Indonesia**
Pertamina Central General Hospital, Jakarta, IndonesiaPertamina
Hospital, 40-50 nonsmall
lung
cancerpatients
were seen annually. The majority
of
thepatients were
theemployees
of
Pertamina,
for
whom
thecytostatic drugs were provided by
thecompany.
44
Jusufet alMATERIAL
AND METHODS
This
is a
retrospective
study on nonsmall
cell
lung
cancerpatients that were
treatedduring
1994-1998 atDharmais
National Cancer Center Hospital
andPertamina
Hospital.
Theinclusion criterias were
:-
confirmed
histologic diagnosis
of
nonsmall
cell
carcinoma
-
nonsmall normal blood
counts,normal CCT
-
stageIIIA, IIIB
and
[V,
with
measurable disease,performance
status>/
70(Karnofsky)
-
chemotherapy regimen,
containing paclitaxel
135mglm2
-
200 mg/m2
and carboplatin
200
mglmZ
or
AUC
6 mg/ml.mm given every
3- 4
weeks,for
6 cycles.
-
at least 3 cycles must be administered-
follow
up
was done every month
up
to
3
monthsand
then
every
3-4
months
or
whenever
the patients hadcomplaints,
until
death-
objective
responses were be recorded,according
toUICC
criteria
(complete response,
partial
response, stable
diseaseand progressive
disease)by
physical
examination
and
chest
X-ray
exarrunatron
-
all
side effects were recorded according
to WHO
Classification
-
dates
of
death
were
recorded
in
the
patient's
journal,
survival time
was calculatedfrom
the dateof
the
beginning
of
chemotherapy.
A
special call
wasgiven
onDecember
3l't,
1998to check which
patients weresurviving
The details
of
treatment were asfollows
:-
hydration
with
saline solution before
theadministration of cytostatic
-
premedication
with
dexamethason,
ondansetron anddiphenhydramine
-
paclitaxel
was
given
over
3
hrs
infusion,
the
dosebeing 135 mg/m2 at the beginning
of
the
study, laterbeing
175mg/m2 or
200mglm2.
Med J Indones
-
carboplatin was given 300 mg/m2
intravenously,
later
dosedto
a targetedAUC
6-
hematologic examination
(Hb,
granulocytes,trombocyte
count) was
performed
every
weekduring
treatmentRESULTS
Nineteen patients were
recruited
for
evaluation.
Therewere
12males and females,
the
ageranged
between42
years and73
years(median
: 57 yrs).
Fourteen
of
them were
stage[V
disease,4
stageIIIB
disease andone had stage
IIIA
disease.Histologic
diagnoses were squamouscarcinoma
in
4 patients,
adenocarcinomain
14
patients
and
adenosquamous
carcinoma
in
I
patient.
Seventeen
patients completed
6
cycles of
chemotherapy, one had
only 3
cycles and one had
4cycles.
The
shortest
follow
up period
was
4
monthsand
the
longest was
35
months
after the
start of
chemotherapy.
Two
patients are
still
alive at
22
and23
months after the start
of
chemotherapy. Objective
responsewas
seenin l2
out
of
19patients
63%.
No
patients had complete
response,
twelve had
partial
response.
Two
patients(l0,5Vo)
showed stable diseaseand progression
was
seen
in
5
patients
(26,3Vo), as seenin Table
l.
Tablel.
Objective Responsein
16
Lung
Cancer Patients Treated with Paclitaxel & Carboplatin (n =l9)
Response No o/o
-
Complete response-
Partial response-
Stable disease- Progressive disease
0
12
2
5
0 63
lt
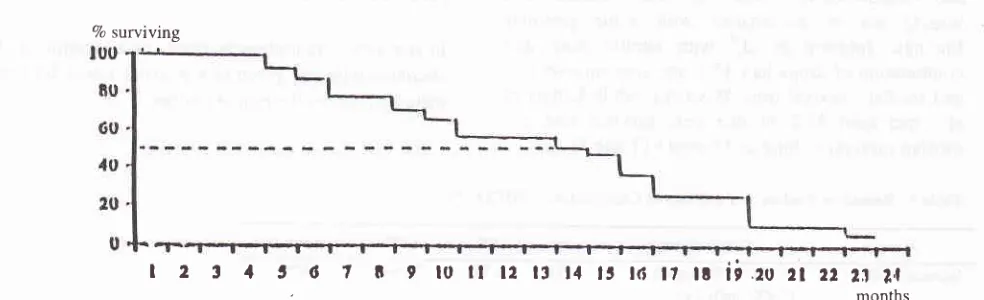
26Eleven patients
live
one year
after
chemotherapy,giving
the one year
survival rate
of
58. The
mediansurvival time
was 15 months as shownin Figure
1.I 2 3 .l t 6 ? I 9 loll
12lt141316171819202122212n
months
Figure 1. The Survival Cuwe of Lung Cancer Patients Receiving a Combination of Paclitaxel and Carboplatin Calculatedfrom the Beginning of Chemotherapy (n
=
19)Vol 9, No
I,
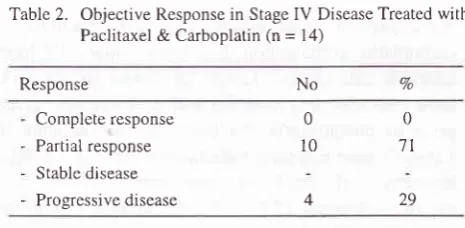
January - March 2000Fourteen patients
had
stagefV
disease.Among
this
group,
4
patients
had
radiotherapy
for
metastasis tothe weight
bearing bones
or the primary tumor.
Theresults
are shovynin Table 2
andFigure
2.
Completeresponse
was
not
seen,
partial response
in
l0/14
(7lVo)
andprogressive
diseasein 4l14
(29Vo), as seenin
Table 2. Among
thesepatients, one
year
survival
rate was
6
out
of
14
patients
(43Vo);
the
mediansurvival time was l4 months
(seeFigure
2).Table
2.
Objective Response in Stage IV Disease Treated with Paclitaxel & Carboplatin (n = 14)Response
Experience in lung caneer
fteatment
45Table
3.
Side Effects of Paclitaxel & Carboplatin CombinationToxicity Parameter WHO Grade (7o)
Neutropenia Thrombocytopenia Nausea./vomiting Neurotoxicity
R'bnat
Cardiac
5 (3l.3Vo) 2 (r2.5 Vo)
|
(6.3 Va)All
patientshad
nauseaand vomitting grade l-2,
none had grade 3-4.Alopecia
was seenin
all patients. No renalor
cardiac
toxicity was found. Neurotoxicity
such
asperipheral neuropathy was
not well
recorded,but
were seenin
some patients, noneof
themhad
grade3 or
4.Serious
side
effects,namely
grade3
thrombocytopeniawere
seenin
5
patients
(26Vo),I
patient
(5Vo) and 2 patients(IIVo),
respectively (Table 3).7o surviving
DISCUSSION
Paclitaxel
and
carboplatin combination
has
beenstudied
by
many investigators
with
various results,
as seenin
Table 4 and 5.Using
similar
doseof
paclitaxel
and
carboplatin,
Johnson et al, Giaccone
et al
andBunn
et
alahad
seen response ratesof less
than 5OVoor
more.
Other investigators
like
Belani et al,
Schutteet al,
and Rowinsky
et
ala used combinations of
paclitaxel
with
carboplatin
dosedto different
targetedAUC-s,
also
hadPR
of
over50Vo.
Our
result which
was
surprisingly high, may
bedue
to more
selectedpatients;
asthis
is
a
retrospective
report
of
patients aftercompleting
the treatment andfollow
up.Complete response Partial response Stable disease Progressive disease
0
t0
4
0
7t
29
I2 t 1 5 6 t 8 I t0il t2llt1 Irt6t7ttii.2021
222t2|
[image:3.595.72.307.229.349.2]'
months [image:3.595.76.568.475.625.2]Vol9, No
I,
January - March2000Fourteen patients
had stage
fV
disease.Among
this
group,
4
patients
had radiotherapy
for
metastasis tothe weight
bearing bones
or
the primary
tumor.
Theresults
areshown
in Table 2
andFigure 2.
Completeresponse
was
not
seen,
partial
response
in
10/14 (7l%o) andprogressive
diseasein
4114 (297o), as seenin
Table 2. Among
these patients, one
year survival
rate was
6
out
of
14
patients (43Va);
the
mediansurvival time was
l4
months
(seeFigure
2).Table
2.
Objective Response in StageIV
Disease Treated with Paclitaxel & Carboplatin (n =l4)
Response
Experience in Lung caneer
treatment
45Table
3.
Side Effects of Paclitaxel & Carboplatin CombinationToxicity Parameter WHO Grade (7o)
Neutropenia Thrombocytopenia Nausea/vomiting Neurotoxicity
R'bnal
Cardiac5 (3l.3Vo) 2 (12.5 Vo)
|
(6.3 %)7o
No
All
patientshad
nausea andvomitting grade
l-2,
none had grade34.
Alopecia was seen in all patients.No
renalor
cardiac
toxicity was found. Neurotoxicity such
asperipheral neuropathy was
not well
recorded,but
were seenin
some patients, noneof
them had grade3 or
4.Serious side effects,
namely
grade3
thrombocl,topeniawere
seenin 5
patients
(26Vo),I
patient
(5Vo) and 2 patients(llVo),
respectively (Table 3).DISCUSSION
Paclitaxel
and
carboplatin combination
has
beenstudied
by many investigators with
various results,
asseen
in
Table 4 and 5.Using
similar
doseof paclitaxel
and carboplatin,
Johnson
et
al, Giaccone
et al
andBunn et
alahad
seen response ratesof less
than 5OVoor more.
Other investigators like Belani
etal,
Schutteet al,
and Rowinsky
et
ala used combinations of
paclitaxel
with carboplatin
dosedto different
targetedAUC-s,
also
hadPR
of
over50Va. Our result which
was surprisingly high, may
bedue
to more
selectedpatients;
asthis
is
a retrospective
report
of
patients aftercompleting
the treatment andfollow
up.Complete response
Partial response Stable disease Progressive disease
0
l0
4
0
71
29
80
60
,l (,
20
0 ttttttttlt
I 2 31t
6 t 8 9 toil
t2 ll
f r11 15
t-t--It6 Ir
ra
ii
.ru
2t
22 21
1,,1'
monthsFigure 2. The Survival Curve of Patients with Stage IV Lung Cancer Receiving a Combination of Paclitaxel and Carboplatin, Calculated after the Beginning of Chemotherapy (n = 14)
[image:4.595.74.307.224.338.2]Vol9, No
I,
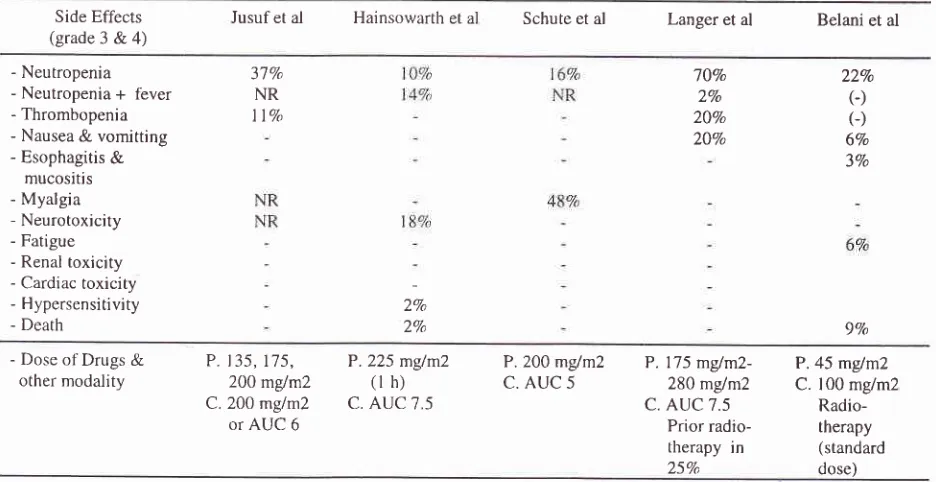
January - March2000fable
6
reviews the
sideeffects
seenin our
serie andin
other studies. Neutropenia
grade
3
and grade
4 seenin
l}Vo -
70Vocases, depending on the
dosesof
drugs and that
of
the othermodality.
Thrombocytopeniagrade
3 was foundin llVo
- 207oof
patients, none hadExperience in lung cancer treatment
grade
[V
trombocytopenia. Other side effects like
gastrointestinal symptoms,
myalgia,
neurotoxicity,
fatigue, renal
toxicity,
cardiac
toxicity,
hipersensitivity
and
other
symptom/signs
were
seen,but
otherwise
quite tolerable
to the patient.Table
6.
Side Effects of Paclitaxel and Carboplatin Combination in Various Regimens, Including MultimodalitySide Effects
(grade 3 & 4)
Iusuf et al Hainsowarth et al Schute et al Langer et al Belani et al
- Neutropenia - Neutropenia
+
fever- Thrombopenia - Nausea
&
vomitting- Esophagitis
&
mucositis - Myalgia - Neurotoxicity - Fatigue
- Renal toxicity - Cardiac toxicity - Hypersensitivity - Death
37Va
NR
I lVo
7j%o 2Vo 20Vo 20Vo 22Vo G)
(J
6Vo 3Vo ZVo 2% 9o/o- Dose of Drugs
&
other modality
P.135,175, 200 mglm2 C.200 mglm2 or AUC 6
P.225 mglm2
(l h)
C. AUC 7.5
P.200 mglm2
c.
AUC 5P. 175 mglm2-280
m{m2
C. AUC 7.5
Prior radio-therapy in
25Va
P.45
m/m2
C. 100 mgim2
Radio-therapy (standard dose)
CONCLUSION
l.
Paclitaxel
in
combination
with
Carboplatin
isquite efÏective
for
stageIII & IV
nonsrnall cell
lung
cancer,
with
63Vo responserate (PR),
oneyear survival
rate
of
58Voand median survival
time
74.2 months.2.
Major
sidL efïects are gastrointestinal
symproms(nausea
and
vomitrng), alopecia
and
bonemarrow
depression,which
arequite
tolerable.Acknowledgement
The
authorswish
to
thank theOncology
Team,Bristol
Meyer
Squibb Indonesia
for
their
support
in
carryingout this
study
and
Dra.
Sita Laksrni Andarini
and Wahyr.rAniwidyaningsih, Miss Anggriani, SKM
andMr.
Apong
Sulaimanfbr
preparing the report.REFERENCES
l.
Hainsworth JD. Thomson DS. Urba WJ. et al. One Hour Paclitaxel plus Carboplatinin
Advanced Nonsmall Cell Lung Cancer (NSCLC). Preliminary Results of a Multi-institutional Phase 1l Srudy, Scientific Proceedings, 32ndAnnual Meeting, American Thoracic Society of Clinical Oncology, 1996:125.
2.
Langer C. Kaplan R. Rosvold E. etal.
Paclitaxel (P) by Ihr
lntusion
Combinationwith
Carboplatin(C) in
Advanced Nonsmall Cell Lung Carcinoma (NSCLC) : A Phasell StudyJ. Clin Oncology 1995,l3:
1860-70.3.
Schutte W. BorkI.
Sucker S. PhaseII
Trial of Paclitaxel and Carboplatin asFirst Line
Treatment in Advanced Nonsmall Cell Lung Cancer, Scientific Proceedings, 32ndAnnual Meeting, American Thoracic Society
of
Clinical Oncology, 1996: 137.4.
Belani CP. Paclitaxel/Carboplatinin
the Treatment of Nonsmall Cell Lung Cancer. Oncology (Suppl), 1998, 12: 74-9.5.
PistersKMW,
Ginsberg RJ. Phase IITrial
of
Induction Paclitaxel & Carboplatin (PC) in Early Stage (T2N0, Tl -2 [image:5.595.72.540.198.439.2]48
6.
Iusuf et
al
Scientific Proceedings, 346 Annual Meeting, American Thoracic Society, 1998:129.
Langer C. Kaplan R. Rosvold E. Milleson
M'
Smith MR' JohnsonC, et
al.
Paclitaxel(P)
by
I
hr
Intusion Combinaton with Carboplatin (C) in Advanced NonsmallCell
Lung
Carcinoma (NSCLC):
A
PhaseII
Study'Scientific Proceedings,
32d
Annual Meeting, American Thoracic Society of Clinical Oncology, 1996: I 35'Med J Indones
7.
Belani CP. AisnerJ.
HiponiaD.
et
al.
Paclitaxel and Carboplatin with Concurrent Thoracic Radiotherapy'for
Regionally
AdvancedNonsmall
Cell
Lung
CancerNSCLC)
Scientific Proceedings, 32nd Annual Meeting,American Thoracic Society
of
Clinical
Oncology,