Vol ll, No 2,
April-
e 2002 HRT in menopausalwomen
97Effects of
continuous
Hormone Replacement Therapy
(HRT) on
FSH,
lipid
profiles, blood chemistry, and skin thickness
in
menopausal \ilomen
A. Baziad
Abstrak
Penelitian
ini
bertujuan untuk melihat efek pemberinnTSH
estradiol 2 mg+
I mg noretisteron asetat secara kontinyu terhadap
hormon
FSH,profil
lipid, kimia darah, serta ketebalan kulit.pada wanita menopause. Lama pemberian TSH adalah 6 bulan.Bahan penelitian terdiridai
35 wanita menopause. Penelitian ini berlangsung dart Januari 2001 hinggaluni 2001.
Setelah TSH 6 bul.anterjadi penurunan yang bermalma terhadap FSH. Tidak dijumpai pengaruh TSH terhadap kadnr bilirubin, namun dijumpai sedikit peningkatan enzim alkali fosfatase, serta peningkatan yanç bermalqa SGOT dan SGPT. menyebabl<nn penurwtan kadar kolesterol total serta penurunan kadar trigliseida. Selain itu dijumpai sedikit peningkatan LDL, dan penurunan
kalar HDL
secara bermalma. TSH dengan progesteron sintetik noretisteron terjadi peningkatan sintesis kolagen kulit, yang ditandai dengan adanya peningkatan ketebalan kulit. yang bermalua. (Med J Indones 2002; 11: 97-103)Abstract
This study was aimed
to
observe the effect of hormone replncement therapy (HRT) of estraliol 2 mg+
1 mg acetate noretisterone administered continuously on FSH hormone,Iipil
profile, blood chemistry, and skin thickness in menopausal women. The durationof
HRT administration was 6 months. The subjects of the study were 35 menopausal women. The study was conducted from January 2001 to June 2001.After
HRT administration of 6 months, a significant decrease of FSH was observed. No effectof HRT
wasfound
inbilirubin level; however, there was a slight increase of alknli phospluttase enzyme, and a signifcant increase
in SGOT
and SGPT. HRT caused a decrease of total ckolesterol level and triglyceride level. In addition, a slight increase of LDL level and significant decreaseof
HDL
level were obsert,ed. HRT administration with progesterone synthetic noretisterone showed an increase of skin collagen synthesis, which was indicated by the significant increase of skin thiclotess. (Med J Indones 2002; 11: 97-103)Keywords: HRT, FSH, menopause, Iipid profile, blood chemistry, skin thiclctess
Menopause
is
aphysiological process which
will
beexperienced by
every
woman.
Estrogen deficiency
results
in
the menstrual disorder leading
to
menstrual cessation.As
a resultof this
estrogendeficiency,
50-60Vo
of
women
will
experience
complaints
which
require medical help. One
of
the
health
problemsattracting a great deal
of
attention
of
the countries in
the world
is
osteoporosis.
Nearly
4OVoof
womenapproaching
the
age
of
70
suffered
from
bone fractures associatedwith
osteoporosis.l The
expensesincurred by
acountry
in providing
healthcarefor
bone fractures reach ashigh
asbillions
of US dollars.
Department of Obstetrics and Gynecology, Facuby
of
Medicine University of Indonesia/ Dr. Cipto Mangunkusumo General Hospital,Jakarta,
nesiaIn
view
of
the
immense
impacts brought
about by
osteoporosis,
an
early diagnosis
of
osteoporosis
isextremely
important.
It
may even
be
more important
than the
treatment
and early
prevention. HRT
Up
to the present, diagnosisof
osteoporosis hasnormally
been performedby observing
the bones
directly
by
means
of
radiology.
The type
of
radiological
examination
commonly
used
is ratio isotop
(single
photon
absorptiometer),Dual
Photon Absorptiometry
@PA),
Dual
Energy
X
Ray Absorptiometry
(DXA)
and
CT
Scan.Unfortunately,
theseexaminations
arerelatively expensive and carry the risk of radiation.
SB
Baziadthe
skin thickness
of
woman.
By
measuring
skinthickness (collagen),
the presenceof
osteoporosis canbe
identified.
Collagen
in
the
bones consists of
Gellatina,
scleroprotein
which
serve
to
maintain
thestability
of
bones.This type of collagen is
also presentin
the
skin and
cardiovascular structure.
Thus,
this transdermalUSG
tool is
actually
designedto measure
the
collagen content
in
the
skin.
If
the
collagencontent in
the skin decreases,
thecollagen
content
in
the
bone
will
correspondingly decrease.
Thedeficiency
of
collagen
may result
in
wrtnkled,
inelastic skin,
while
suchdeficiency
in
thebone
will
contribute
to the osteoporotic bones.For
the women
who still
have the
uterus,
estrogenshould always
be
combined
with
progesterone
in
order
to
prevent
the
occurrence
of
endometrial
hyperplasia.
The type
of
estrogen
and
progesteronerecommended
is
the natural one.Estradiol
is
the typeof
natural estrogen
most
frequently
used.
Itsmetabolism occurs
in
the
liver,
and
its
long-term
usemay
occasionally interfere
with
liver
functions.
Nowadays, there
are
HRT
specimensusing
syntheticprogesterone, such as noretisterone.
Progesteroneof
this
type requires
an
activation
in
the
liver
to
theextent
that
it
may create
a
burden
in
the
liver."
In
addition,
noretisterone
triggers
the
activity
of
lipoproteinlipase enzyme
in the liver,
which
mayr"iuit
in the disruption ofHDL
andLDL
metabolism.3'aMed J Indone;
MA'T'ERIAL AND METHODS
The
L.1sse61 study was designed as a non-comparatlveclinical
trial"
'Fhis sti.rdy wasllso
desrgnedto
evaluatethe
effect:,
rf
continuors
HRT
;ldmrnrstration before
and
after
6
mlnths on
FSH
hLrrmone,lipid
profile,
blood
chemrstry,
and skin thickness
in
menopausalwomen.
Every womari
received
HRT in
the form of
estradiol
tablets 2mg
anil
noretisterone
acr:tateI
mgcontinuously,
All
patient-c
still
had the intact
uterusand
ovary. The
subjectsof
the studywere
35
patientsof
menopausal
women adrrutted
for
t!'eatment
toMenopausal
Chnic "Menox" in
Jakarta
from
January 2001to
June 2001.History taking
wasundertaken in
all
patients covering
identity, age, and
education.There
were
also asked about history
of
previous
disease
and the
presence
of
climacteric
complaints.After
meeting the
criteria of inclusion
andexclusion,
the patients underwent the
examination
of
FSH,
alkali
phosphatase,
SGOT, SGPT,
total
cholesterol,triglyceride,
LDL, HDL,
ureum, and creatitine.
The
measurement
of
skin
thickness
was
done
using transdermalUSG of
Osteosonbrand manufactured by
Germany
witir
high resolution
(20Mhz) (Fig.
1). Skinthickness
was determined
with
either modus
A
or
modus
B"
The skin
area
measured was the
inside upper partof
left
arm.L\
4 [image:2.612.83.281.459.662.2]?
Vol 1
l,
No 2, April-
June 2002RESULTS
HRT in rnenopausal women 99
Table 1. Mean value of several variables
No Variable
x+SEM
I
2Age (year)
Duration of
menopause (year)
52,4 + 0,76 3,3 + 0,42
Table 2. Education level
Level Frequency %
Primary School Junior High School
Senior High School University graduate
2
9 8 16
5.7 25.7 22.9
45.',l Total
[image:3.612.61.511.341.395.2]Table 3. Effect of HRT on FSH hormone level
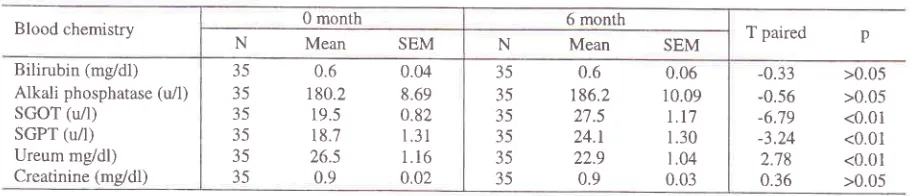
Table 4. Effect of HRT on blood chemistry laboratory
Table 5. Effect of HRT on lipid profile
Table 6. Effect of HRT on skin thickness
100 35
Hormonal 0 month 6 month T paired p
N Mean SEM N Mean SEM
FSH (mIU/nù)
35
63.'t
5.5935
40.1
4.38 6.87 <0.01Blood chemistry 0 month 6 month T
paired
pN
Mean
SEM N Mean SEMBilirubin
(m/dl)
,A,lkali phosphatase
(ùl)
SGOT (u/1) SGPT (u/l) Ureum mg/dl) Creatinine (me/dl)
35
0.6
0.0435
180.2
8.6935
19.5
0.8235
18.7
I .3135
26.5
1.1635
0.9
0.0235
0.6
0.0635
186.2
10.0935
27.5
Lt7
35
24.t
1.3035
22.9
1.0435
0.9
0.03-0.33
>0.05-0.56
>0.05-6.79
<0.01-3.24
<0.012.78
<0.010.36
>0.05Blood chemistry 0 month 6 month T paired p
N Mean SEM
N
Mean
SEMTotal cholesterol (mg/dl) Triglyceride
(m/dl)
LDL (mg/dl)
HDL (me/dl)
35
224.5
4.5635
132.8
14.7335 144.74
5.7335
58.7
2.2135 218.1
5.0235 127.2
13.635 146.5
7.2535
54.3
2.491.',14 0.543
-0.32 2.09
>0.05 >0.05 >0.05 <0.05
Note 0 month 6 month T paired p
N Mean SEM N
Mean
SEM [image:3.612.55.510.423.521.2]100
Baziads2Ê
c
(çOJ
[image:4.612.182.410.86.316.2]O
month
6 monthFigure 2. The effect ofHRT on skin thickness
DISCUSSION
In
1984,
the
average ageof
menopausein
Indonàsiawas 48
years.sIn
this
study,
the
averageage found
was
52.4 years.
This finding
was
not
much different
from
the
average ageof
menopausein
the developedcountries,
i.e.,
approximately between
50
and
51 yea.r.6'tThe
increased ageof
menopausein
Indonesiamay be
attributed
to
the improved nutrition,
and
theevident
improvement
of
living
standard
of
themajority of
Indonesian
women.In
this
study,
the
patients had generally
experienced menopause 3.3 years agowith
most educationlevel
of
university
graduate
(45.1Vo).In
terms of duration
of
menopause,
all
patients were
still
atthe
stageof
early menopause. Since apart
of
the patients had educationlevel
of
junior
high
school and
higher,
it
was
hopedthat
eachpatient
could take the medication regularly
and
appropriately.
The
irregularity.
in
taking
themedication
frequently
resulted
in
bleeding,
and
thismay
causedpatients
to
experience a disorder
and
todiscontinue
therapy.
Table
3
shows
that
aftertermination
of
therapy
a significant
decreaseof
FSHlevel
was
still
found
(p<0.01).
This shows
sufficient
effectiveness
of
the
medication
in
the
body
in
eliminating
theeffects
due to estrogendeficiency.
hr
the
laboratory examination
of
blood chemistry,
asignificant
changeof
bilirubin level
wasfound.
HRT
in
fact has someeffect
onbilirubin.8 In
postmenopausal women,the level
of
alkali
phosphatase wasnormal or
slightly
increased
due
toresorption.e'l0
The long-term
I
year) mayreduce
thelevel
In
this
study,
a slight
increaseof
alkali
phosphataselevel
wasfound
after the administration
of HRT for
6 months,which
isstatistically
notsignificant
(p>
0.05).This
shows
an
increase
of
bone resorption
in
all
patients studied
who may
have developed osteoporosisin
the futureif
theyhad
notbeen
treated.In
the present study, theadministration
of HRT
showsa
significant
increase
of
SGOT and SGPT
levels;however,
this
increase
was
still
within the
normal
values
(normal value
of
SGOT was 11-36
p,/1, andSGPT
was
10
-65
M). In
the
postmenopausalwomen,
an increaseof both
SGOT and SGPT
levelswere
found,
and
the administration
of estrogen may
cause
an
increaseof
thoseenzymes.t'''-t'la Therefore,
caution should be exercised
in
using
HRT in
women
with liver
disorder.Generally
in
the
postmenopausal
women there
is
aVoI I
I,
No 2, April-
June 2002HRT
administration, the
secretionof
urine
wasfound
to return to normal
condition.l6'17[n
the present study,no
changein
thelevel of
serumcreatinine
wasfound
after
the
administration
of
HRT
for
6
months"Generally the ureurn
level in
postmenopausal womenslightly
increases,
and
with HRT
administration
its
level
may return
to
normal
or
slightly decrease.l8
From Table
4 it
is evident that afterHRT
administration theureum
level
decreasedsignificantly;
however,
this decreasewas
still
within
the normal
limits
(normal
limit:
10-50mg/dl).
From epidemiological study
it
was proved that
the decreaseof
total
chole
tp
to
2-3Vomay
reducethe
risk
of
coronary
disease
by
I
Vo.tBThe
administration
of
estrogen
with
or
without
acombination with
progesterone
may
reducethe
level
of
total cholesterol
by 10
-
20
Vo.le'z0Inthis
study,
adecrease
in
the
level
of total cholesterol from
224.5mg/dl
to
218.1 mg/dl and a
decreaseof
triglyceride
level
from
132.8
mg/dl to
127.2
mg/dl
were found
after
the
adminrstration
of
HRT
for
6
months,although
these decreases
were
not
statistically
significant (normal value
of
total cholesterol:
750-225mg/dl,
triglyceride: 40
-145 mg/dl).
From various
studies
it
was evident that
high HDL
level
has
protective properties
for
the heart,zt'22
while high
LDL
level
increasesthe
risk
of
coronary heart disease.2rIn this study,
aslight
increaseof
LDL
level
wasfound
after the administration
of HRT for
6months,
i.e.,
from
144.15mg/dl
to
146.5mg/dl (p
>
0.05).
However,
this
increase wasstill within
normal
values (60
-160 mg/dl).
After
6 months
of
therapy,
asignificant
decreaseof LDL
level was found.
This
decrease was
not
hazardous sinceits
valueswere
still
within the
normal limits
i
normal HDL:
45
-
80mg/dl).
The
decrease
of
HDL
level
was
closely
associated
with
the type
of
progesterone
used.Synthetic
progesterone
such
as
noretisterone
hasbeen
proved
to
reduce the
level
of HDL
serum
andmay
increase
the
level
of LDL
s".um.tn'"
Natural
erone such
as
medroxy
progesteronacetateproved
to slightly affect
lipid
metabolism.2aThe
administration
of
noretisterone
10mg.in
women before menopausewho
underwent theremoval of
bothovaries caused
an
increase
of
LDL
level
by
I3Vo, decreaseof HDL by
35Vo,while
theadmrnistration
of
natural
progesterone such asMPA
proved to
have noeffect
on
lipid
metabolism.2o'2sIn
this
study, a
significant
decreaseof HDL level
wasfound, but this
was followed
by
a
significant increase
of
total
cholesterol
level, in
addition to the
decreasedlevel
of
HRT in menopausal
women l0l
triglyceride.
Metabolic
changesfelt
werenot
disturbing,this is
because the EuropeanAtheroschlerosis.society
stated
that
lipid
disorder could
only
occur
if
total
cholesterol
level was found
above
300
mg/dl,
triglyceride
level
was above 200 mg/dl, and HDL
level
wasbelow
35 mg/d1.26Table
6
showsthat
the
averageskin thickness
beforetherapy
was
0.93 mm, which
means that
all
thecollagen levels
of all
patients have decreased.Normal
values
of
skin
thickness wereabove
1.0 mm.r'27In
thecondition
of
prolonged
estrogendeficiency
a decreaseof
collagen
synthesis
may
occur
in
the
skin
and bones.22In
1987,
Brincat2Tfound
a
decreasein
thecollagen
level
of
the
skin
andbone
with the
increaseof
age. Brincart28 also showed that upto the
ageof
50the
skin
thickness
of
women
is
relatively stable;
however, due to estrogen
deficiency
theskin
thicknessgradually
diminishes.28On
the other
hand, Shuster2e
suggested
that
with
the
increase
of
age
every
yearwomen
will
lose
skin
collagen
by
lVo. From
theresults showed
in
Table 6,
it
may be
concluded
thatall
thosewomen
haveexperienced
osteoporosis sincetheir
skin thickness was on the averagebelow
1.0 mm.Unfortunately,
transdermal
USG
does
show
which
bones
have
undergone osteoporotic
process.Transdermal
USG only
provides
adescription
on
theamount
of
skin
collagen
still possessed
by a
woman.After
6
months
of
therapy,
a significant
increase
of
skin
thickness was
found (p <0.01). The
increaseof
skin
thickness largely depends
on
the type
of
pr^Qgesterone used.
The study conducted
by
Baziad
et al30in
1gg4 did
not
show any
significant
increaseof
skin
thickness
in
the
postmenopausal
womenreceiving conjugated
estrogentablet
0.625
mglday +
Dydrosgesterone
tablet
10mg/dl
for
a period
of
one year.This
may be attributedto
rhefact
that thetype
of
progesterone used wasof
natural type.
By
contrast, in
the
presentstudy
the
type
of
progesterone used wasnoretisterone,
which
is a
synthetic
progesterone. Several investigators haveproved
that anaddition
of
5mg
noretisterone
cyclically
in
the
postmenopausalwomen
resulted
in
the
increase
of skin collagen
by
5OVo.27'31
However, there
is still
controversy
as
towhether
the
increaseof
such collagen
level
is
really
due
to
testosterone-derived
hormone
such
asnoretisterone.
In
fact,
the
level
of
blood
androgen in
the
menopausalwomen
is
sufficiently high,
yer
it
isthe question
to
be answeredwhy
thecollagen level in
those
women remains
low
and they are vulnerable
to102 Baziad
skin
and bonesbe
observed.It
can be concluded
thatthe most
important factor
in
the
increaseof
collagenlevel
is
the
role
of
estrogen.
On
the
other
hand,noretisterone
only
serves
to
facilitate
the work
of
estrogen
in
the skin
and bones.
The
increase
of
progesterone
in
the
HRT
agent
is
in fact
aimed
to preventwomen
from
being
attackedwith
endometrial
cancer.
CONCLUSIONS
The
average ageof
menopausein this
study
was 52.5 years andthe
averageduration
of
menopause was 3.3years.
As
many as
45.7Voof
patients had
educationlevel
of
university
graduate.No
changesin bilirubin
level
after the
administration
of
HRT
for
6
months.There was
aslight
increaseof
akali
phosphatase afterthe
therapy.
A
significant
increase
of
SGOT
andSGPT
levels was found;
however,
this
increase
wasstill within
thenormal limits. In
addition,
there was adecrease
in total
cholesterol and triglyceride
levelsafter
6
months
of
therapy.
The
administration of
testosterone-derived
synthetic
progesterone,
such
asnoretisterone, resulted
in
the slight
increaseof
LDL
level, and significant
decreaseof
HDL
level.
This
decrease
was
not
hazardous as itwas
still
within
thenormal
limits
for
HDL.
HRT with
natural
estrogen +synthetic
noretisterone progesterone
resulted
in
thesignificant
increaseof
skin
thickness.REFERENCES
1.
Kuhl H, Taubert HD. Postmenopausale Osteoporosis. In: Das Klimakterium. Georg Thieme Verlag. Stuttgart-New York, 1987:291-3222.
Conference Report Consensus Development Conference:prophyiaxis and treatment
of
osteoporosis.Br
med
J. 1987;295: 914-63.
TikkanenMJ, Nikkila
EA,
KuusiT,
SipinenS.
Highdensity lipoprotein-2
and
hepatic lipase:
reciprocal changes producedby
estrogen and norgestrel.J
clin Endocr 1982; 54 : I I 13-174.
TikkanenMJ, Nikkila
T,
Kuusi T,Sipinen S. Differenteffects
of
two
progestinson
plasmahigh
densitylipoprotein (HDL2) and postheparin plasma hepatic lipase
activity. Atherosclerosis 1981; 40: 365-69
5.
Agustina T, Keep PAV. The climacteric in Bandung, West Java Provinces, Indonesi a. Maturitas 1984: 6: 333 -7 26.
Krailo MD, Pike MC. Estimation of the distribution of ageat
natural
menopausefrom
prevalencedata.
Am
J Epidemiol 1983; I l7:356'7.
BirkhauserM,
BraendleW,
BreckwoldtM,
Keller PJ,Kuhl
H,
RunnebaumB.
Empfehlungendes
"Zrxcher Gesprachskreises"zu
Substitutionmit
Estrogenen undMed J Indones
Gestagenen im Klimakterium und
in
der Postmenopause.Frauenarzt 1999; 40: 153-55
Kuhl H, Jungh-Hoffmann C, Storch A, Fitzner M, Ruhl E.
New aspects on the mechanism of action of contraceptive steroids
-
recent pharmacokinetic studiesof
low
doseformulations. Adv Contracep 1991;3: 149-63
Christiansen C, Christensen
MS,
McNair
P, Hagen C,Stocklund
KE,
Transbol I. Preventionof
early
post-menopausal bone loss: controlled 2-year studyin
315normal females. Europ
J
clin Invest 1980;10:273-79 Christiansen C, Christensen MS, Larsen NE, TransbolL
Pathophysiological relationshipsof
estrogen effect onbone metabolism. Dose-response relationships
in
early postmenopausal women.J
clin
Endocr 1982;55 :1124-30 Daniell HW. Osteoporosisof
the slender smoker. Arch intern Med 197 6; 136:298-304Moore B, Paterson MEL, Sturdee DW, Whitehead TP.
The effect of menopausal status and sequential mestranol and noretisterone on serum biochemical profiles .
Brit
J Obstet Gynaec 1981; 88 : 853-58McPherson K, Healy MJR, Flynn FV, Piper
KAJ,
Garcia-Weeb P. The effect of age, sex and other factors on blood chemistry in health. Clin chimActa
1978; 84 :373-
97Hodgkinson
A.
Biochemical changes at the menopause:possible role
of
the central nervoussystem.
Maturitas 1984;6 :259- 67Gambert
SR,
Tsitouras PD, Duthie EH. Interpretationof
laboratory results
in
the elderly.A clinician's
guide toendocrine tests. Postgrad med J 1982; 72:251-56 Lobo RA, Brenner P, Mishell DR. Metabolic parameters
and steroid levels
in
postmenopausal women receivinglower
dosesof natural
estrogen replacement. ObstetGynec
19831'62:94-8
Jones MM, Pearlman B, Marshall DH, Crilly
RG,
NordinBEC.
Dose-dependent responseof
FSH,
flushes andurinary calcium to oestrogen. Maturitas 1982;4:285
-
90Kuhl
H. Klimakterium,
Postmenopauseund
Hormonsubstitution. Unimed Verlag, Bremen 1999; 95
-
101Kuhl H.
MetabolischeEffekte
der Ostrogene
und Gestagene. Gynakologe 1997 ;30:357-
69Kuhl H. Cardiovascular disease and estrogen replacement therapy
-
epidemiological data.In :
LippertTH,
MuckAO
(eds). Sex Steroids and the Cardiovascular System. Pathernon London. 1998 : 97- i09Levy RI. Cholesterol, lipoproteins, apoproteins, and heart
disease: present status and future prospects.
Clin
Cheml98l:27:653
-
6l
Fisch FH, Huber JC. Die Hormonsubstitution
in
Wandel der Zeit. Krause&
Pachernegg GmbH, Gablitz, 2000 :119-27
Tikkanan
MJ,
KuusiT,
Nikkila
EA,
Sipinen S. PosG menopausal hormone replacement therapy: effectsol
progestogens on serum lipids and lipoproteins.
A
revierv Maturitas 1986: 8 :7 -17Pickar JH,
Wild RA,
WalshB,
HirvonenE,
Lobo RA. Effectsof
different hormone replacement regimens onpostmenopausal
women
with abnormal
lipid
levels.Climacteric 1998;
I
:26-31
Silfverstolpe G, Gustafson
A,
SamsioeG,
Svanborg A,Lipid
metabolic studies in oophorectomised women:effect on serum lipids and lipoproteins
of
three syntheticVol I l, No 2, April
-
June 2002Study Group, European Atherosclerosis Society. Strategies
for
the preventionof coronary heart disease:
A
policystatement
of
the European Atherosclerosis Society. EurHeartJl98T;8:77
Brincart M, Wong TYA. Response of skin thickness and
metacarpal to
estradiol therapy in
postmenopausalwomen. Obstet Gynec 1987; 70 :538
Brincart
M,
Moniz CJ, StidWW, Darby
A,
Mayor G,Embury G, Verti E. Long-term effects of the menopause
and sex hormones on skin thickness. Br J Obstet Gynaecol
1985;92:256
-9
HRT in menopausalwomen 103
Shuster S, Blach
MM, Verti
E. The informed of age and on skin thickness , skin collagen and density. Brit J Derm 1975;93 :639-43Baziad
A, Salim
A,
HestiantorqA, Kuhl H.
pengukuranketebalan
kulit
untuk deteksidini osteoporosis
denganUSG transdermal pada wanita menopause yang mendapat
terapi substitusi. Maj Obstet Ginekol Indones 199l- 2l :
109
-
13Punnonen R, Vilska S, Rauramo L. Skinfold thickness and
long-term post-menopausal hormone therapy. Maturitas
1984;5:259 -62 29
30 26
27
28