140 Saifuddin Med J Indones
Issues
in training for
Essential
Maternal Health
Care
in
Indonesia
Abdul Bari Saifuddin
Abstrak
Anglca Kematian lbu di Indonesia masih tinggi, yaitu sekitar 390 per 100.000 kelahiran hidup pada tahun 1994. Perkiraan
AKI
dari
beberapa penehrtan sejak 1978-1994 menunjukkan penurunan yang lamban, walaupun telah dicanangkan bahwa pada akhir Repelin VI angla kematian ibu diharaplun dapat ,nenjadi 225 per 100.000 kelahiran hidup. Upaya penurunan AKI di Indonesia telah banyak dilakukan. Diurailcan. tentang kerangka l<onseptual dari McCarthy dan Maine yangterdii
atas determinan jauh, determinan antara, dan keluaran. Keluaran meliputi proses kehannilan, komplilcasi kehamilan dan persalinan, dan kematian/disabilitas. Determinan antara rneliputi status kesehatan, status reproduksi, al<ses pada pelayanan kesehatan, dan perilaht/pemanfaatan pelayanan kesehatan,serta faktor-faktor yang tidak terduga. Determinan jauh melipurt stutus wanitct, status keluarga, dan status masyarakat. Pada bagian terakhir ditinjau tentang peran pelatihan pada Gerakan Safe Motherhood, meliputi pendidil<an tenaga kesehatan dan pelntihnn laniutan tenaga kesehatan. Peranan Jaingan Nasional Pelatihan Klinikyang dipeloport okh POGI yang memperkenalkan Pelartlnn Berdasar Kompetensi dalam bidong Keluarga Berencana dan Kesehatan Reproduksi sangat berarti.
Abstract
The Matemal Mortality Ratio (MMR) in Indonesia remains high, i.e. approximately 390 per 100,000 live births. The esrtmated MMR obtained from the studies
from
1978 to 1994 suggests a sbw reduction, although it has been determined that by the end of Five Year Plan VI, the MMR is expected to be reduced to 225 per 100,000 live births. The efforts to reduce the MMR in Indonesia have been reasonably made. The conceptualframeworkfromMcCartlry andMaine, consisrtng of distant determinants, intermediate determinants,and outcomc will be outlined. The outcome includes the process of pregnancy, complication of pregnancy and labor, and mortality/dis-ability. The intermediate determinants include health status, reproductive status, access to health services, health care behavior, and unknown/unpredictedfactors. The distant determilwnts encompasses womm's status, family's status in community, and cotntnunity's status. The last section
of
this paper reviews the role of the trainings in safe motherhood movement, covering the education of health personnel and the subsequent continuing education. The role of the National Clinical Training Network initiated by POGI, which introduces the Competency Based Training in Family Plnnning and Reproductive Health is very significant.Keywords: Maternal
Mornlity
Ratio, comprehmsive framework, determinants, preservice training, in service trainingThe
Maternal
Mortality
Rate, or more accurately
theMaternal
Mortality
Ratio
(MMR),
is
one
of
the
in-dicators
for assessing
the
success ofhealth
develop-ment.MMR is
thekey
indicator
thatreflects maternal
health status,particularly
themortality risk
ofpregnant
women
andfor delivery. The target to
be achievedin
theeffort
to reduceMMR in Indonesia
has beenestab-lished
as a decreaseto
aMMR of
225 maternal deathsper 100,000live-births by
the endof
the 6thFive-Year
Development
Plan
(1994-1999) and
80
maternal
deaths
per
100,000live-births by
the endofthe
SecondTwenty
Five
Year,
Long-term Development
Plan
Department of Obstetrics and. Gynecology, Faculty
of
Medicine, University of Indonesia/Dr. Cipto Mangunhtsutno Hospital, Jalcarta, Indonesia(2015) respectively.
The corresponding
policies
andaction plans
to
reduce maternal mortality have
alsobeen established. These include the improvement
of
integrated management at both central
and regional
levels, the equalprovision
ofhealth
services, an enhan-cementof health
servicequality,
anoptimum
increaseof
basic service resources,
the development
of
ap-propriate technology,
the development
of
amanage-ment information
system and community institution
activities, social
marketing,
andoperational
researchfor improving
thequality of
"ut"
management.l
In
accordwith
thesepolicies,
avariety of efforts
have beeninitiated
by both the government and the
com-munity.
Nevertheless, theMMR
in Indonesia isstill
thehighest
in
the Southeast Asian Region.
In
addition,
there exists a widevariation in
maternalmortality
ratesgiven province. However, unlike
theMMR,
in
the caseof
theinfant mortality
rate there has been arelatively
steepdecline
from
142 infant
death per- 100,000live
birth
in
1968to
57per
100,000in
1992.2MMR IN
INDONESIA
It
isnot
easyto obtain
accurateMMR
datain
develop-ing countries,
particularly in Indonesia, primarily
be-cause of the
limitation
of
avital registration
system and thelack
ofreliable
data.Various
attempts to obtainthis
data over a long period
of
time have been made in
Indonesia. Unfortunately,
thevarying
approachs usedfor
dataidentification,
analysis, and scopeofcoverage
hasled to
a greatvariety of MMR figures that require
very careful interpretation.
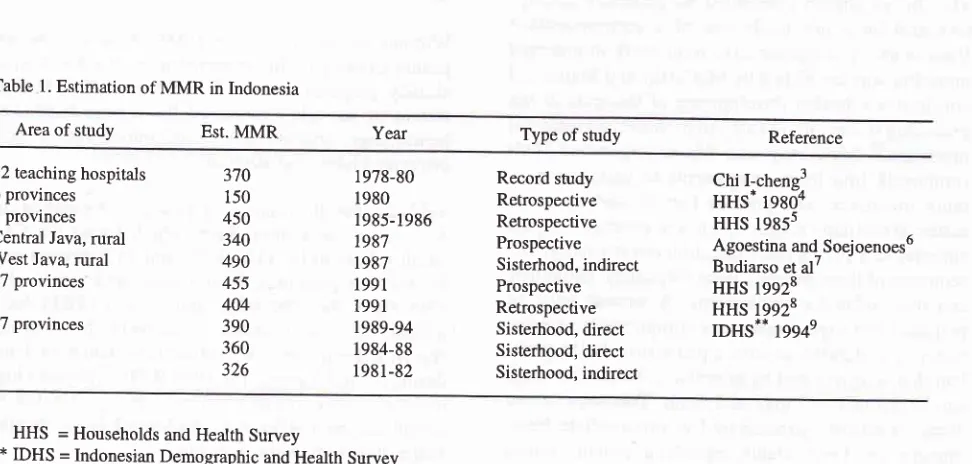
Table
1
shows various estimations
of MMR
in
In-donesia, based on anumber of
studies conductedfrom
1978to
1994.
1985
and
1986Household
andHealth
Survey
(tHS)
data,
using an approach
of
retrospective
data
iden-tification
andmaternal mortality
diagnosiswith verbal
autopsy, estimated Indonesian
MMR
at
450maternal
deaths
per
100,000
live-birthr.5
Ho*"u"r,
the
1985/1986
HHS
sampled households
in
only
sevenprovinces.
Thusthis
estimatedMMR figure
canhardly
be
thought
of
as
a
nationwide representation.
Theretrospective
approach
is
thought
to
be biased
by
atendency
for
underreporting
to
the
extent
that
it
provides
alower
estimation than what is actually
thecase.
Table
l.
Estimation of MMR in IndonesiaThe
1992HHS, covering 27 provinces
of
Indonesia,
provided two
estimations
by means
of
two different
approaches. Basedon
aretrospective
calculation,
theIndonesian maternal
mortality
rate was estimated to be 404 maternal deathsper
100,000live-births.
Based ona
prospective
calculation (follow-up
of
pregnant
women
through the completion
of
the
postpartum
period),
theMMR
was estimared to be 455 per 1 00,000live-births.E
The
Indonesian Demographic and
Health
Survey
(IDHS) provided
anational
MMR
esrimation
of
390per
100,000live-births
for
the period
1989-94, and 360per live-births
for
theother period
of
1984-89
(sister-hood method,
direct),
and estimation
of 326
per
100,000
live-births
for
the period earlier then
1980(sisterhood, indirect).e
It
should
be
noted that
the sisterhoodmethod is essentially retrospective
aswell,
so
that there exists a possibility that the
estimatedfigure
islower
than the actual one,particularly for
thepastperiods. In view
ofthis
"increasingtendency",
theMMR
basedon the
1994HHS
may be interpreted
as suggestingno
changesin
thematernal mortality
rate.If
thesimilar retrospective
approachof the
1985/1986HHS
data is to be comparedwith
that ofthe
1 992HHS,
MMR
shows
a declining
tendency
from 450
per
100,000live-births
to
404per live-birrhs. This figure
was, however, obtained
from two
different
surveyswith
adifferent
coverageof provinces,
and theremay
be aprobable sampling error in
these approaches.In view of
thevarious estimations elucidated
above,it
may beconcluded
thatMMR in Indonesia
isrelatively
Area of study Est. MMR Year Type of study Reference
l2
teaching hospitals 6 provinces7 provinces Central Java, rural West Java, rural 27 provinces
27 provinces
Record study Retrospective Retrospective Prospective Sisterhood, indirect Prospective Retrospective Sisterhood, direct Sisterhood, direct Sisterhood, indirect
Chi l-chene3
HHs.
tgsôa HHS 1985sAgoestina and_ Soej oenoes6 Budiarso et al /
HHS 19928 HHS 19928 IDHS** 1994e 370
150 450 340 490 455 404 390 360 326
1978-80 1980 1985-1986 1987 1987 1991 1991 1989-94 1984-88 1981-82
*
HHS = Households and Health Survey [image:2.595.42.528.505.737.2]142 Saifuddin
very
high
andstill
a averages around 400per
100,000live-binhs in
theearly
1990s.EFFORTS TO REDUCE
MMR IN
INDONESIA
On June 29
1988, President
of
the Republic
of
In-donesia, Suharto,
announced
the
Safe
Motherhood
movement and
called
on
all sectors
and parties
to
support
this movement,
theprimary objective
ofwhich
was
to
reduce
MMR.
A
national meeting was
sub-sequentlyheld
in November
1988with
the purposeof
enhancing the
case andinter-sectoral cooperation
be-tween thegovernment
and thecommunity. In
afurther
effort to
establish
national
strategies
andplans
of
ac-tion to
achieve the targetedreduction
ofMMR
already agreedupon,
anationwide
assessment wâsconducted
in
1991by
Department
of
Health,
supportedby
TheUnited Nations Development Program
and TheWorld
Health
Organization.
The
assessmentreport
has beenpublishedln
six volumes.lo
(1)Assessment
of
Maternal
Health
Situation
andHealth
Services(2) Assessment
of
Socio-cultural
Aspects(3) Assessment
of Midwifery
education
and Practices (4)An
Executive Summary
of
the Assessment and theRecommended
National
Strategies(5) Recommended Plan
of Action
(1992-1996)
(6)
Summary
of
RecommendedProvincial
StrategiesApart
from
the
national
assessment,it
was necessaryto undertake
studiesleading to
theprovision
ofinfor-mation
on the actual
efforts
madein
reducing
MMR.
The
studies already conducted
aregenerally
descrip-tive
and have not made
use
of a
comprehensive
framework.
A
comprehensive
framework in
maternal
nnortality
wasdeveloped by
McCarthy
andMaine
andconstitutes a
further
development
of
thoughts
of
thepreceding
researchesin
safemotherhood
andmaternal
mortality.ll
McCarthy
and
Maine
organized their
framework
into
three
components
of
maternal
mor-tality
processes.
The
process
that
is
the
nearest
to
maternalmortality
is the sequenceof
events oroutputs
cumulatively giving
rise todisability
or
mortality.
The sequenceof
these events covers pregnancy,childbirth,
and their related complications.
A
woman must
bepregnant
andexperience
somecomplication of
preg-nancy or
childbirth,
or
have apreexisting
healthprob-lem that
is
aggravatedby pregnancy, before her
death canbe
defined
as amaternal
death.Îhis
sequenceof
eventsis directly
affected
by five
intermediate
deter-minants, i.e., health
status,reproductive
status, accessMed J Indones
to
health
services,health
carebehavior/use
of
health
services and
unknown or unpredicted factors.
On the other
hand,
various socio-cultural
and
economic factors (women's status
in
family/com-munity,
family status
in
community, community's
status)constitute distant determinants that
will affect
MMR
through
thoseintermediate determinants.
With
this framework in mind, all
theefforts
aimed to reduceMMR
must
be undertakenthrough: (1)
theprevention
of
possible conception;
(2)
the possible
reduction
of
pregnant
women developing pregnancy
or
delivery
complications,
and(3)
the improvement
in
the output
of
pregnantwomen
with
complications.
Prodmate l)eterminants
With
the
successof Family
Planning program,
it
canbe
said
that the current incidence
of
pregnancies
in
Indonesia
is relatively lower than
in
the past.
The
decline
in pregnancy
incidence is
evident
from
the decreaseof
the
Total Fertility
Rate
(TFR) from
5.61(period
of
1967-70,according
toPopulation
Censusof
1,97 0)t92,85
(periodof
1 9 9 I -9 4, accordin g to the 19 9 4IDHS).v The
successof
Family Planning
program is
also reflected
in the
changesof
various
variables
of
proximate determinants
affecting
apregnant woman,
e.g., the increasing use of contraceptives,first
marriage
age,
and
age
at first
sexual
relationship.
The
1994
IDHS
showed adecline
in
theproportion of mortality
of
15-49
yearsold
women
asmaternal
mortality,
and suggested a decreaseof
theMMR
of
15-49
yearsold
women
from
42 maternal
mortalities
per
100,000
women to
37per
100,000.Without any decline in the
MMR,
however, the
ex-posure
to
the possible maternal
mortality for
women
already
pregnant
remained
unchanged.
The
leading
causes
of
mortality remained the classic triad,
i.e.,
hemorrhage, gestosis, and sepsis,
followed
by
anemia,prolonged labor
andabortion.
Table2
shows thefindings of
a studyby Agoestina
and Soejoenoes6in
Centrallava,
whièh ioond
th"
Cu*"
Fatality
Rate
to be
35Vo, l9%o,and
ll.Vo
respectively
for retentio
placentae, hemorrhage,
and
sepsis. The
1986
HHS, the
1992HHS,
andthe
1995HHS
docu-mented the complications
of
delivery:
hemorrhage, sepsis, and eclampsia,with
almost constantprevalence
during
the last 8 years.The
1994IDHS
reported
a highincidence
of
pregnancy/delivery being effected by
complications
(24Vo),
e.g., prolonged labor,
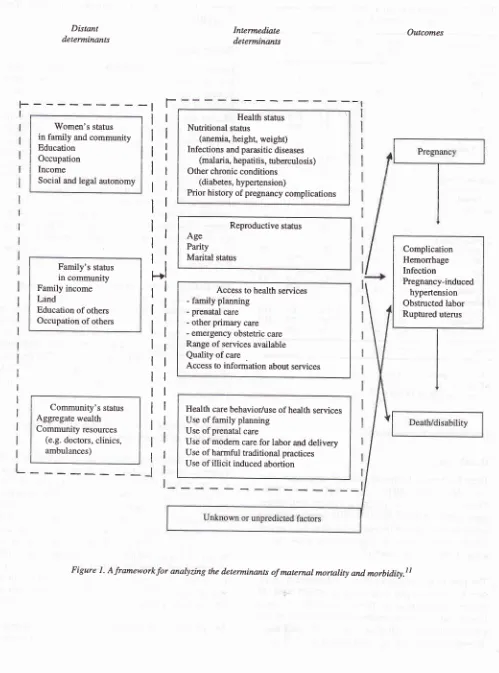
Distant determinants
'Women's stafus in family and community Education
Occupation Income
Social and legal autonomy
Family's status
in community Family income Land
Education of others
Occupation of others
Community's stahrs
Aggregate wealth Community resources
(e.g. doctors, clinics, ambulances)
L
Intermediate determinan*
Health status
Nutritional status
(anemia, height, weight) Infections and parasitic diseases
(malaria, hepatitis, tuberculosis) Other chronic conditions
(diabetes, hypertension)
Prior history of pregnancy complications
Reproductive status
Age Parity Marital status
Access to health services
- family planning
- prenatal care
- other primary care
- emergency obstetric care Range of services available Quality of care
Access to information about services
Health care behavior/use ofhealth services
Use of family planning
Use of prenatal care
Use of modem care for labor and delivery
Use of harmful traditional practices Use of
illicit
induced abortionOutcomes
t.
ll
tl
ri
lr
tl
ll
ir
[image:4.595.38.537.88.761.2]i-i
lt
li
ll
lt
ll
ll
lr
1l
tl
rl
Figure 1. Aframeworkfor analyzing the determinants of matemal mornlity and morbidity.lt
Complication Hemorrhage Infection
144 Saifuddin
Table 2. Complication among a sample of pregnant women
and deliveries, Central Java, 1989
Med J Indones
increased
from
8.6Vo(he
1986
HHS)
to
9.8Vo (The 1992 HHS).5'8Reproductive Status
From the
1991 and1994IDHSs,
it is
evident
that thereis an increase
in the first
marriage
age and inthe
first
delivery
age,
the
reduction
of
average children
delivered,
andthe increasing distance
of
birth
space.Median age for first sexual
relationship
rose,
and the prevalenceofteenager's delivery
decreased.This
pat-tern
of
reproduction
has an effecton
the reductionof
fertility
and thenumber
of
pregnancy,
and the changein
composition
of
women
delivering
according
to
ageand
child
progression.
The
percentage
of
women
delivering
first
children
rose, the percentage ofwomen
delivering the fourth or
more
child
decreased, theper-centage
of
safe
delivery (2-3 children)
remained
un-changed. The percentage
of women
delivering
at a safe age (20-34years) also remained unchanged
but the
proportion
of
deliveries
at
an
age
below
20
yearslowered
and at age 35 andhigher
tendedto
increase.The
changes
in
the reproductive pattern discussed
above
do
not
significantly alter the composition
of
pregnant women
exposed
to
high
risk
maternal
or
infant
mortality.
The percentageof women included
in
one
of
the groups
of
high
risk
deliveries
does
not
significantly
change:
67.2Vofor The
1991
IDHS and
66.4Vo
for
The
1994IDHS
respectively.e
Thepercent-age
of
women
to
be included
in
two, or
more, risk
groups also
remain
unchanged:
36Vo(The
1991
and1994IDHSs).e
Access to
Health Services,
Heolth
Care
Behavior/
Utilization of Health
ServicesAccess
to
health
services
can be viewed from
suchfactors
aslocations of
family
planning
services,prena-tal
care,primary health care, or essential
obstetric
careservices
provided
for
the community, the
available
forms
of
services,
quality
of
services, and
accessto
information
services.
The
government has
made
reasonable
effort to
ensure easy
accessto
those
ser-vices
for
the
community
primarily
by
developing
health
facilities,
multiplying
the
availability
of
health
personnel
anddiversifying
the
kinds
of
services.The
Rural
Midwife
Program,
which aims
atposting
amid-wife
in
every villages,
started
by the
govemment
in
1992, may be abreakthrough towards
theseproblems.
The extent
of
antenatal
care
coverage
for
pregnant
women
has,in point of
fact,
been broadened.During
aComplication
Number
CFRSample Death
RR 7o
ARExposed
Anemia
Yes
No
Emesis
< 5 months
No
Hemorrhage
< 5 months
> 5 months
No
Rupture of membrane Premature
Normal Infection
Yes
No
Retentio placentae Yes No Labor Prolonged Normal Toxemia
0,4
1,40,3
1,00
0,0n
19,1
122,223 0,2
1,03 9,7
30,747 0,3
1,0270 r4658 5348 9580 110
t4t
14677 31 14897 123 14805 34 14894 190 t4'13811
4,139
0,313
10,63',7
0,21,8 98,2 35,8 64,2 0,7 0,8 98,3 0,2 98,8 0,8 99,2 0,2 99,8 1,3 98,7 2,O 0,6 97,4 22 28 15,3 1,0 42,3 1,0 12,7 23,8 20,6 53,4
he-eclampsia
295Eclampsia
88No
toxernia
1454512 3s,3
138,33
8 0,3
1,08 2,7
11,68 9,1
38,934 0,2
1,05,8
25,4
0,7
t7,3 18,3
1 0,5
1,649 0,3
1,0Total 14928 50
RR = CFR exposed/CFR not exposed
AR = p(RR-l)/tpGR-l)+ll
xsourie: Agoesiina and Soejoenoes6
Intermediate Determinants
Health
Status
There has been a
decline
of anemia
in pregnancy
from
74Vo
(The
1985/86
HHS)
to
63.5Vo(The 1992
HHS).
There
is still
l3Vo
of
pregnant women
with
severeanemia
(Hb
< 8 gVo).8 The 1992HHS found nearly
57oof
pregnantwomen in Indonesia suffering
from
hyper-tension,
with
ahigher incidence
in rural
areas than inurban
areas (5.4Vovs
3.9Vo).8The
pattern
of
the causes
of
general
mortality
in
In-donesia
has
changed
freq:1en1lyin
accord
with
theepidemiologic transition.
Degenerative
diseases havebecome
all
the more evident,
while
infectious
andparasitic
diseases
still
play a
part.
TBC
still
has
aperiod
of
I
eragewas
80HHS)"
but
thepercen
to
82Vo
(The
However,
of
delivery
assistance has not changed.According
to the
1994IDHS, only
36.57oof
the
delivery
was assisted
by
health
providers. The remaining
were
assistedby
traditional birth
attendants(TBA). A
greatmajority
of
deliveries took place
at home(77Vo,Tlte
l994IDHS).e
The
IDHS
1994 demonstrates rhathigh risk
pregnant
women have worse neonatal behavior than
thosewithout
risks.
This
also the casewith
pregnantwomen
with lower level
education and
living in rural
areas.The pelcentage
of
high risk
pregnant women
asdescribed above
proved to remain
unchanged.Indirect Determinants
Although these
determinants
do not directly
affect
maternal
mortality, socio-cultural,
economic,
religious,
and
other factors must be
taken
into
con-sideration
andintegrated
into
the interventions
to
beimplemented.
TIIE
ROLE OF TRAINING IN
SAF'E
MOTIMR.
HOOD
INITIATIVES
Based
on the
above discussion,
it
may
be concluded
thattwo
main interventions
can beimplemented
in
theeffort
to
lower MMR:
-
To
continue the efforts to prevent
pregnancy by
means
of
increasing the availability
and
use
of
moderncontraceptive
services as along-term
solu-tion in
reducing
MMR.
-
To promote theprovision
and coverage of essentialobstetric
servicesin
such away that
they
areeasily
accessible
to
the communities as
a more direct
approachto
lowering MMR.
In order to implement
theseinterventions successfully,
it
is necessary to have health personnel (humanresour-ces)
in
a sufficient number with
adequatequalifica-tions. Health personnel
resourcescurrently providing
obstetric
services consist
of consulting
obstetricians/
gynecologists, obstetricians/gynecologists,
general
practitioners, midwives, and traditional
birth
atten-dants.
Pre-service
Training
At
present,
the number
of
consulting
obstetricians/
gynecologists is very
limited
and generally they serveas academic
staff
aT faculties
of
medicine.
Obstetricians and gynecologists (members
of
In-donesian Society
of
Obstetrics and Gynecology,
POGI),
at present, are
approximately
800
in
number
with
an unevendistribution. About
300 obstetricians
and
gynecologists
reside in Jakarta. Thefacility
closestto
the
rural
population where there
might be
anObstetricians and
Gynecologist
aredistrict
hospitals,
although
it
should
be
made
clear
that
not all district
hospitals have obstetricians andgynecologists
on staff.Currently,
future obstetrician and gynecologists
aretrained
atnine educational
institutions
of higher
learn-ing
and
now number
350
participants. The
graduateobstetricians and gynecologists produced
per
year
range between
60 and
80.There are at present 32
faculties of medicine
(compris-ing
15faculties
at stateuniversities
andli
faculties
atprivate universities)
in Indonesia,
producing
anaverage
of2000
graduatesofgeneral practitioners
eachyear.
Every
graduateis
obligated to undertake
aman-datory
assignmentfor
the government
for
aperiod
of
1-3
years as non-permanent employee
at
health
centers, which are
divided into
three categories:"Very
outlying", "Outlying"
and "Normal" health
centers.During
their education
atmedical faculties,
it
is hopedthat the graduates
will
obtain
acapability
in
essential obstetricsfunctions
asoutlined in the Core
Curriculum
of Faculty of Medicine specified by the Consortium
of
Health
Sciences."
However,
asoutlined
in
the Report ofMOIVUNDP/IVHO,
itis
statedthat "There is
awide
variation
in
the uniformity
of
skills
and
technical
capability
among healthpersonnel of the
sameprofes-sional level,
particulary
those postedin
health centers
andDistrict
Hospitals
in
the managementof
pregnan-cy,
delivery
and postpartum
period".ls
It
is alsoafactthatnearly
6O7oof
thefunctions carried
out
by
health center physicians are administrative
tasks, e.g. meetings
with sub-district
leaders
andMin-istry of
Health personnel,
aswell
asproviding
reportsto
the
Ministry of Health, sub-district
leaders,
or
theNational Family Planning Coordinating Board.
The
clinical
functions,
particularly
essential obstetrics,that
the doctor
undertakes
is
consequently
limited, with
most
of
thesefunctions carried out by
midwives.
Paramedics
providing
theseprimary
services aremid-wives.
In
addition, there are general nurses graduated
from nursing
schools,
nursing
academy (a three-year
educational program), and nursing diploma
coursest46
Saifuddinschools
'wereclosed
in
1980),
(2) nursing
and
mid-wifery
schools,
(3)
Midwifery
Training
Program-A,
(4)
Midwifery
Training Program-B,
and (5)Midwifery
Training
Program-C.
The
Midwifery
Training
Program is situated innursing
schools. Currently, there exists 118 public
nursing
schools
(this
doesnot
include
Army
nursing
schools)and 54
private nursing
schools locatedin
27provinces.
The
Midwifery Training
Program is
established as anacceleration
program
to
produce 54,000
Rural
Mid-wives through
1996.Upon
the
completion of
the
ac-celeration program,
TheMidwifery Training
Program
will
becontinued
with
the purposeof
producing
only
about 5,000
midwives
eachyear
aspart
of
a
"main-tenance" program.
The midwives
arecoordinated by
The
Indonesian
Midwives
Association
(IBI), currently
with
46,1_13members
in282
chaptersthroughout
In-donesia.l5
Traditional Birth
Attendants play
amajor role in
preg-nancy
anddelivery
assistancein Indonesia.
According
to the
1994IDHS, only
37Voof
the pregnancies wereassited
by health
personnel
in
Indonesia.e
The
1991IDHS
showed
a percentageof
327o.This
meansthat
more than 60Vo
of
pregnancy was not assisted byhealth
personnel.
It
should be noted
that
there
is no formal
training required
to be atraditional birth
attendant andgenerally the skills
of
a
traditional
birth
attendantis
handed
down by
meansof
infofmal
apprenticeship.At
present, the
number
of
traditional
birth
attendantsis
approximately
70,000,
andthe
majority
have
alreadygained
somebasic knowledge
andskills
such asfind-ing
and referring pregnant women, assisting with
delivery,
postpartum care, and
the
treatment
of
high
risk newborns,
"threeclean" delivery
assistance, homecare, postpartum
mother
and
newborn
care, nursing
and
health
careby traditional birth
attendant, reportsand services
for
pregnant women,
delivery,
postpar-tum,
andnewborn.
In-service
Training
Today, the
great
majority
of
health personnel
in
In-donesia are those employed under the
Ministry of
Health,
including
Non-
Permanent Employees.During
the
period
of
employment,
they
areusually
provided
with opportunity for
in-service
training,
both through
the
Ministry
of Health
andthrough
othergovernmental
institutions such as the National
Family
Planning
Coordinating Board
(Division
of
Family
Planning
Training),
aswell
asother professional organizations
(Indonesian Medical Association, Indonesian
Mid-Med. J Indones
wives
Association, Indonesian
Association
of
SecureContraceptives, Indonesian Society
of
Obstetrics
andGynecology,
etc).Faculties of medicine
arefrequently
engaged
in
launching continuing
educationin
theform
of training
courses,refreshing
courses, seminars,sym-posia
and soforth.
Regretably,
the vastmajority
of
thesetrainings
arenot
standardized and
coordinated; they
areoverlapping
in
their
contents and do
not utilize
"competency
based"training
method.The existing
courses
held by the
Ministry of
Health
range
from
manageriaUadministrative
courses to basicclinical skill training,
aswell
aspublic
health
courses.Through
its
Directorate General
of Medical
Services,the
Ministry
of
Health has conducted a number
of
courses
for
health personnel destined
to
be posted
to
hospitals.
The majority
of
these courses are
held in
cooperation
with
teaching hospitals and professional
organizations.
Under the coordination
of
the
Direc-torate
of
Public Health,
these courseslast
for
one to
three weeks
and
provide in-service training
for
ap-proximately
1,000midwives
each year.The plan is to
increase these
midwife
participants
to 4,900 each year.Since
1994, aLife
Saving Skills (LSS)
course,
com-prising
10modules,
has beenheld_in
13provinces by
the
Directorate of
Family
Health.rÔThe
10modules
of
this
Life
Saving
Skills
Course were
adaptedfrom
theACNM
andcover:
-
Introduction
toMaternal
Mortality
- Antenatal Risk
Assessment andTraining
-
Monitoring
Labor
Progress-
Episiotomies
andRepair
of
Lacerations
- Prevention
of
Treatment
of
Hemorrhage
- Resuscitation
-
Prevention
andManagement
of
Sepsis-
Hydration
andRehydration
-
Vacuum
Extraction
-
Neonatal
careDuring
1994 and 1995, as many as 4,922
Yillage
Midwives
were trained
through this LSS
Course.
An
assessment
of
the
effectiveness
of
this LSS training
program was conducted
in
1995by Wibowo
et al.
in
East
Java,
South Sulawesi,
and West
o.r7
A
similar
study was undertaken by
.
in
13
Indonesian
provinces.ls
thesl
studies
arrived
at theconclusion that
theLSS
training
was necessary
but not quite
effective
towards
enhanc-ing
the
skills
of Village Midwives, particularly
when
there-by
which
thecompetency of
the trainees areovaluated
both at the
beginning
and at the endofthe
training,
andso
forth. Also,
more attention
should be focused at the adequacyof
training
sites
in
terms
of
equipment
andtraining
materials,
trainers, staffing,
caseload
avail-able
for
practice,
and manageméntof
thetraining.
POGI's
RoIe
in
Strengthening Reproductive
Ilealth
Training
Based
on
findings
in
the
7992 Jojnt
IUD/1.{orplant
Trainings
Assessmentla
by BKKBN, pOGI,
and
JHPIEGO,
it
was proposed todevelop
aunified,
stand-ardized,
andsupervised national
clinical training
net-work. This network would
be establishedfrom
already
existing,
operating
clinical
training
facilities;
andwould
concern
itself
initially with clinical
training
for
Norplant,
IUD,
and Infection prevention
(NIIp),
aswell
asproviding
aRefresher
NIIp
Training
Course. Once a systemfor
applying
Competency BasedTrain-ing
(CBT)
to
one
area
of
reproductive health
was masteredby
a core groupof
trainers, theintention
isto
expand
CBT through the National Clinical Training
Network
to
other
areas
of
reproductive health.
To
facilitate
change
throughout
the
clinical training
net-work, POGI
proposed
implementation
of
a training
system
which
createdspecific roles
for
andcollabora-tive
relationship among various levels/institutions
within
the
network,
including a NRC
(National
Resource Center), PTCs
(Provincial Training
Centers),and
DTCs
(District Training
Centers).The
primary
role of
theNRC
is toguide
the processof
developing
nationally
agreed uponreproductive health
service standards, developing
training
materials,
preparing master expert trainers
andclinical
trainers,
and
develop
a systemof
follow
up and supervisionthat
should
be
able
to maintain
the
quality
of
the
clinical
training
network.
The
PTCs' primary
role is to
standardizedistrict level
trainers
in
clinical skills, train district
level trainers
in
clinical training skills, carry out clinical training for
doctors
andmidwives from
thedistrict level,
andfol-iow
uptraining
at thedistrict
level.
The
primary role of
theDTCs is to carry out clinical
training for
doctors andmidwives from Health
Centersand supervise service
delivery,
To
datemuch
progress has been achievedin realizing
the
unified
and standardizednational
clinical training
network, with
the focus
initially
on
Family
planning.
Approximately
1,800 service providers have
par-ticipated
in
theNIIP
Refresher Course, more than
20expert trainers
have proceededthrough the Advanced
Training
Skills
Course
level, more than 70 clinical
traines have been standardized and
undergone
aClini-cal
Training Skills
course, and morethan
1,800 serviceproviders have qualified and
are
practicing clinical
family
planning
based
on the completion
of
a CBT
courss.
A
National
Resource
Document
for
Family
Planning Services
has beencompleted
for
use
as thestandardized resource
forFamily
Ptanningtraining
andservices.
A
National Resource Center
for
Clinical
Training,
located
in two
sites(Jakarta
and Surabaya),and
7 PTCs have
beenestablished. Other
pTCs
havebegun
to
take
part
in
the
two
stepprocess
of
servicedelivery
standardization and
clinical training skill
training
andpractice.le
STJMMARY AND RECOMMENDATIONS
.
From
the above observations,it
may beconcluded that
the
MMR
--
with
a target
to
to
225 maternal
deaths per
the end
of
the 6th Five
Year
Development
Plan
--
will
undoubtedly pose
anenor-mous challenge.
The main interventions should be directed
atthe
out-come
of
conception
or
pregnancy:
reduction
of
thecomplications
andwhat
complications
regnancy (by
meansinitiatives
(essentialobstetric services) must be made
in
concert
andin
aprofessional
way. For this reason, the adequatenumber
of
health personnel and the optimalization
of
their
skills
gained through
both
pre-service
andin-service
training constitute
an indispensable partin
the strategy.ing
network in Family
Plan-PTCs
andDTÇS, developed
be
beneficial.le
It
is
hopedso be
used
for
the clinical
training
in
essential obstetrics,
through both
as-148 Saifuddin
sociated
with
the outcome
(proximate
determinants),particularly
physicians
andmidwives,
will
be able
to come awaywith
betterskills from
thistraining.
Inview
of
the breadthof
coverage, apilot
project
for
EssentialObstetrics
at thelevel of NRC may
be necessary,with
several PTCs
to
implement
an Essential
Obstetrics
clinical training project
at aninitial
stage.Through
POGI
the obstetricians
andgynecologists
atthe
district
level,
whose number isvery
limited,
should
be encouraged
to
broaden
their
tasksto include
rolessuch
as resource
person
and
initiator
in
developing
improved
system
of
maternal health services at
their
locations.
Also the
delegation
of
authority
from
obstetricians and gynecologists
to
general
prac-titioners
and
midwives
in
the front-line
will
provide
tdlutionr to
the existing
geographical and
time
con-trarnt problems,
particulu.ty
i"
emergency situations.
Health centers should be
ableto
carry out
their
func-tions
in
essential
obstetrics, as recommended
by
WHO.20 On the other
hand, thehealth providers who
have proved themselves to be capable to
carry
outtheir
tasks should receive a rewardin
theform
of creditsthat
can be
caulculated
in
pursuing
ahigher or continuing
education.
The
utilization of
appropriate
andrelatively
new
com-puter
assistedtraining tools,
such as
Repro
System,will
be
of
benefit
in
improving the
transfer
of
knowledge, updating trainers, and
strengthen
plan-ning.
Trainees can come to theclinical
training
sitefor
the purpose
of
enhancing their
clinical skills
since the necessarynew knowledge
has already been
acquiredthrough
a
computer
assisted
learning program
like
ModCal,
whichis alsopartof
Repro System.Usingthis
approach, a gteat deal
of time
andmoney
can be savedfor
basictraining
activities.
Another
factor worth
considering is
areorientation
of
the
physician's
tasks athealth
centers.This
reorienta-tion
could
beaccomplished by
putting
more emphasison
clinical functions
that
include
essential obstetrics.Administrative
and
other
non-medical functions
should
be
gradually transfered
to
other
competent
health personnel,
such aspublic
health
graduatesthat
have
hitherto
been producedin
afair
numberfrom five
faculties
ofpublic
health
in
Indonesia.
REFERENCES
1, Gunawan N. Kebij aksanaan Departemen'Kesehatan tentang
pengelolaan kasus obstetri di tingkat pelayanan dasar dalam
Med J Indones
rangka menunjang upaya Safe Motherhood (Government policy on management of obstetrics cases at prirnary health
services to support Safe Motherhood initiatives). Bandung:
VIII
POGI Annual Meeting, 1992.2. Soemantri S. Angka kematian anak,
bayi,
dan maternal (Child, infant, and maternal mortality). Jakarta: SDKI 1994Seminar, 1995.
3. Chi l-cheng, Agoestina T, Harbin J. Maternal Mortality in
Twelve Teaching Hospitals in Indonesia. An epidemiologic analysis. Int J Gynecol Obstet 1981;19:259-66.
4. Budiarso LR, F\rtrali J, Muchtaruddin. Laporan dan Statistik SKRT 1980. Jakarta: Balitbangkes RI, 1981.
5. Survei Kesehatan Rumah Tangga 1985. (1985 Health Household Survey). Jakarta: Balitbangkes RI, 1986.
6. Agoestina T, Soejoenoes A. Technical Report on the Study
of Matemal and Perinatal Mortality
in
Central Java. Ban-dung: BKS Penhn, 1989.7. Budiarso LR. Maternal Mortality in West Java. Maj Obstet Ginekol Indones.
l99l
;17:l
66-7 2.8. Survei Kesehatan Rumah Tangga 1992 (1992 Health Household Survey). Jakarta: Balitbangkes RI, 1992.
9. CBS, NFPCB,
Ministry
of
Health, MacroInt.
Inc.
In-donesian Demographic and Health Survey 1994.10.
Ministry
of
Health,UNDP, WHO.
Safe Motherhood. Volumel-6
Jakarta, 1991.ll.
McCarthyJ,
MaineD.
A
Frameworkfor
Analyzing the Determinantsof
MaternalMortality.
Stud Fam Plan.l99l;23:23-33.
12. Departemen Pendidikan dan Kebudayaan
RI
(Ministryof
Education and Culture). Kurikulum Nasional Pendidikan Dokter di Indonesia, 1992.
13.
Ministry
of
Health,UNDP, WHO.
Safe Motherhood. Recommended Planof
Action
(1992-1996). Volume 5.Jakarta, 1991.
14. Saifuddin AB, Affandi B, Djajadilaga, Santoso BI, Fihir IM,
Bergtbold GD, Mclntosh N, Tietjen LG. IUD and Norplant Training Assessment Report.
BKKBN,
POGI, JHPIEGO; 1992.15. Annas
Y.
Continuing Education for Indonesian Midwives.Jakarta:
IBI,
1995.16. Marshall MA, Buffington ST. Life Saving Skill Manual for Midwives. Washington, DC, USA: American College
of
Nurse Midwives, 1991.
17. Wibowo A et al. Evaluative Study on The Life Saving Skills Trainning for Village Midwives at Central and East Java,
South Sulawesi and West Nusa Tenggara, Indonesia.
Jakar-ta: Ministry of Health, University of Indonesia, UMCEF,
1995.
18. Maclean
GD,
SweetBR,
Tickner VJ. Evaluationof
the Effectiveness of the Life Saving Skills Programme for Bidan di Desa in Indonesia. The British Council, 1995.19. Saifuddin AB, Affandi B, Djajadilaga, Widohariadi, Bimo,
Ajello
C. Strengthening Indonesia's Reproductive Health Education and Training System. Pre-congress Seminar: Leaming without Walls. Bali, 1995.20. WHO. Care
of
Mother and Babyat
the Health Centre.