S U M M A R Y
BAN QUEMONDIALE BAN COMUNDIAL
placeinwhichtolive.
AnishVergheseKoshy,President,FriendsforLife,Bangalore,India
We,thesurvivingrelativesofthevictimsofroadaccidents,appreciatetheinitiativeofWHOandthe publicationofthisreport.Itiswrongtoplacetheresponsibilityforcausingandpreventingroadcrasheson thedriveronly;weneedtolookatthevehicleandtheroadaswell.
Ben-ZionKryger,Chairman,Yad-Haniktafim,Israel
Therearenotmanyroads,thereisasingleroadthatextendsacrossthelengthandbreadthofourvast planet.Eachofusisresponsibleforasegmentofthatroad.Theroadsafetydecisionsthatwemakeordo notmake,ultimatelyhavethepowertoaffectthelivesofpeopleeverywhere.Weareoneroad–oneworld.
RochelleSobel,President,AssociationforSafeInternationalRoadTravel,UnitedStatesofAmerica
Thehumansufferingforvictimsandtheirfamiliesofroadtraffic–relatedinjuriesisincalculable.Thereare endlessrepercussions:familiesbreakup;highcounsellingcostsforthebereavedrelatives;noincomefora familyifabreadwinnerislost;andthousandsofrandstocareforinjuredandparalysedpeople.DriveAlive greatlywelcomesthisreportandstronglysupportsitsrecommendations.
MoiraWinslow,Chairman,DriveAlive,SouthAfrica
WHOhasdecidedtotackletherootcausesofroadaccidents,aglobalscourgecharacteristicofour technologicalera,whoselistofvictimsinsidiouslygrowslongerdaybyday.Howmanypeopledieorare injured?Howmanyfamilieshavefoundthemselvesmourning,surroundedbyindifferencethatisalltoo common,asifthisstateofaffairswereanunavoidabletributesocietyhastopayfortherighttotravel?May thisboldreportbyWHO,withtheassistanceofofficialorganizationsandvoluntaryassociations,leadto greaterandgenuineawareness,toeffectivedecisionsandtodeeperconcernonthepartofroadusersfor thelivesofothers.
JacquesDuhayon,Administrator,AssociationdeParentspourlaProtectiondesEnfantssurlesRoutes,Belgium
Worldreport
onroadtraffic
injuryprevention
andeconomicimpactoftheseincidentsworldwide.Weheartilywelcomethisreportandstronglysupport thecallforaneffectiveresponse.
MarcelHaegi,President,EuropeanFederationofRoadTrafficVictims,Switzerland
Roadaccidentsareanever-endingdrama.Theyaretheleadingcauseofmortalityamongyoungpeople inindustrializedcountries.Inotherwords,theyareahealthemergencytowhichgovernmentsmustfinda response,andallthemoresobecausetheyknowwhattheremediesare:prevention,deterrenceandmaking theautomobileindustryfaceuptoitsresponsibilities.Thisreportisacontributiontowardstheeffortsofthose whohavedecided,whetherornotafterapersonaltragedy,tocometogripswiththisavoidableslaughter.
GeneviéveJurgensen,FounderandSpokesperson,LeagueagainstRoadViolence,France
Manydeathsandinjuriesfromroadcrashesarecompletelypreventable,especiallythosecausedbyalcoholor drug-impaireddrivers.WHOhasdoneimportantworkbyfocusingattentiononroadviolenceasagrowing worldwidepublichealthproblem.ThisreportwillbeavaluableresourceforMothersAgainstDrunkDriving anditsalliesinworkingtostopimpaireddrivingandinsupportingthevictimsofthiscrime.
DeanWilkerson,ExecutiveDirector,MothersAgainstDrunkDriving,UnitedStatesofAmerica
TheWorldHealthOrganizationwasestablishedin1948asaspecializedagencyoftheUnitedNationsserving as the directing and coordinating authority for international health matters and public health. One of WHO’s constitutional functions is to provide objective and reliable information and advice in the field of human health,aresponsibilitythatitfulfilsinpartthroughitsextensiveprogrammeofpublications.
TheOrganizationseeksthroughitspublicationstosupportnationalhealthstrategiesandaddressthemost pressingpublichealthconcernsofpopulationsaroundtheworld.TorespondtotheneedsofMemberStates atalllevelsofdevelopment,WHOpublishespracticalmanuals,handbooksandtrainingmaterialforspecific categories of health workers; internationally applicable guidelines and standards; reviews and analyses of health policies, programmes and research; and state-of-the-art consensus reports that offer technical adviceandrecommendationsfordecision-makers.ThesebooksarecloselytiedtotheOrganization’spriority activities,encompassingdiseasepreventionandcontrol,thedevelopmentofequitablehealthsystemsbased onprimaryhealthcare,andhealthpromotionforindividualsandcommunities.Progresstowardsbetterhealth forallalsodemandstheglobaldisseminationandexchangeofinformationthatdrawsontheknowledge andexperienceofallWHO’sMembercountriesandthecollaborationofworldleadersinpublichealthand thebiomedicalsciences.
Worldreporton
roadtrafficinjuryprevention:
summary
Editedby
MargiePeden,RichardScurfield,
DavidSleet,DineshMohan,
AdnanA.Hyder,EvaJarawan,
ColinMathers
1.Accidents,Traffic–preventionandcontrol2.Accidents,Traffic-trends 3.Safety4.Riskfactors5.Publicpolicy6.Worldhealth.I.Peden,Margie
ISBN9241591315 (NLMclassification:WA275)
©WorldHealthOrganization2004
Allrightsreserved.PublicationsoftheWorldHealthOrganizationcanbeobtainedfromMarketingandDissemination,WorldHealth Organization,20AvenueAppia,1211Geneva27,Switzerland(tel:+41227912476;fax:+41227914857;e-mail:bookorders@who. int).RequestsforpermissiontoreproduceortranslateWHOpublications–whetherforsaleorfornoncommercialdistribution –shouldbeaddressedtoPublications,attheaboveaddress(fax:+41227914806;e-mail:[email protected]).
Thedesignationsemployedandthepresentationofthematerialinthispublicationdonotimplytheexpressionofanyopinion whatsoeveronthepartoftheWorldHealthOrganizationconcerningthelegalstatusofanycountry,territory,cityorareaorofits authorities,orconcerningthedelimitationofitsfrontiersorboundaries.Dottedlinesonmapsrepresentapproximateborderlines forwhichtheremaynotyetbefullagreement.
Thementionofspecificcompaniesorofcertainmanufacturers’productsdoesnotimplythattheyareendorsedorrecommendedby theWorldHealthOrganizationinpreferencetoothersofasimilarnaturethatarenotmentioned.Errorsandomissionsexcepted, thenamesofproprietaryproductsaredistinguishedbyinitialcapitalletters.
TheWorldHealthOrganizationdoesnotwarrantthattheinformationcontainedinthispublicationiscompleteandcorrectand shallnotbeliableforanydamagesincurredasaresultofitsuse.
Thenamededitorsaloneareresponsiblefortheviewsexpressedinthispublication.
Contents
Foreword v
Preface vii
Acknowledgements xi
Thefundamentals 1
Introduction 1
Apublichealthconcern 1
Thesocialandeconomiccostsofroadtrafficinjuries 2
Changingfundamentalperceptions 2
Thepredictabilityandpreventabilityofroadcrashinjury 2
Theneedforgooddataandascientificapproach 3
Roadsafetyasapublichealthissue 3
Roadsafetyasasocialequityissue 4
Systemsthataccommodatehumanerror 4
Systemsthataccountforthevulnerabilityofthehumanbody 4
Technologytransferfromhigh-incomecountries 4
Thenewmodel 5
Asystemsapproach 5
Developinginstitutionalcapacity 5
Achievingbetterperformance 7
Sharingresponsibility 7
Settingtargets 8
Buildingpartnerships 9
Theglobalimpact 11
Global,regionalandcountryestimates 11
Global,regionalandcountrytrends 12
Profileofpeopleaffectedbyroadtrafficinjuries 13
Socioeconomicstatusandlocation 14
Otherhealth,socialandeconomiccosts 14
Healthandsocialcosts 14
Economiccosts 15
Needforreliableinformation 16
Riskfactorsandinterventions 19
Introduction 19
Managingexposurewithland-useandtransportpolicy 19
Exposuretoriskofroadtrafficinjury 19
Reducingexposurethroughland-useandtransportplanning 20
Minimizingexposuretohigh-risktrafficscenarios 21
Planninganddesigningroadsforsafety 22
Riskofinjuryfrompoorplanninganddesign 22
Safety-consciousdesignofroads 22
Safetyaudits 24
Remedialactionathigh-riskcrashsites 24
Providingvisible,crashworthy,smartvehicles 24
Riskofinjuryfrompoorvehicledesignandmaintenance 24
Improvingthevisibilityofvehiclesandvulnerableroadusers 25
Improvingthecrashworthinessofmotorvehicles 26
Designingsmartvehicles 27
Settingroadsafetyrulesandsecuringcompliance 28
Riskofinjuryfromlackofrulesandenforcement 28
Settingandenforcingspeedlimits 28
Settingandenforcingalcohollimits 29
Medicinalandrecreationaldrugs 31
Addressingtheproblemofdriverfatigue 31
Reducingtheriskofjunctioncrashes 31
Requiringseat-beltsandchildrestraints 32
Requiringhelmetsontwo-wheelers 33
Banningdriversfromusinghand-heldmobilephones 33
Educatingandinformingthepublic 34
Deliveringcareaftercrashes 34
Improvingcarebeforereachingahospital 34
Improvinghospitalcare 35
Improvingrehabilitation 36
Doingresearch 36
Conclusionsandrecommendations 37
Mainmessagesfromthereport 37
Recommendedactions 39
Conclusion 42
Foreword
Every day thousands of people are killed and injured on our roads. Men, women or children walking, biking or riding to school or work, playinginthestreetsorsettingoutonlongtrips, willneverreturnhome,leavingbehindshattered families and communities. Millions of people eachyearwillspendlongweeksinhospitalafter severecrashesandmanywillneverbeabletolive, workorplayastheyusedtodo.Currenteffortsto addressroadsafetyareminimalincomparisonto thisgrowinghumansuffering.
TheWorldHealthOrganizationandtheWorldBankhavejointlyproducedthisWorldreportonroadtrafficinjury prevention .Itspurposeistopresentacomprehensiveoverviewofwhatisknownaboutthemagnitude,riskfac-torsandimpactofroadtrafficinjuries,andaboutwaystopreventandlessentheimpactofroadcrashes.The documentistheoutcomeofacollaborativeeffortbyinstitutionsandindividuals.CoordinatedbytheWorld HealthOrganizationandtheWorldBank,over100experts,fromallcontinentsanddifferentsectors–includ-ingtransport,engineering,health,police,educationandcivilsociety–haveworkedtoproducethereport. Road traffic injuries are a growing public health issue, disproportionately affecting vulnerable groups ofroadusers,includingthepoor.Morethanhalfthepeoplekilledintrafficcrashesareyoungadultsaged between15and44years–oftenthebreadwinnersinafamily.Furthermore,roadtrafficinjuriescostlow-incomeandmiddle-incomecountriesbetween1%and2%oftheirgrossnationalproduct–morethanthe totaldevelopmentaidreceivedbythesecountries.
Butroadtrafficcrashesandinjuriesarepreventable.Inhigh-incomecountries,anestablishedsetofinter-ventionshavecontributedtosignificantreductionsintheincidenceandimpactofroadtrafficinjuries.These includetheenforcementoflegislationtocontrolspeedandalcoholconsumption,mandatingtheuseofseat-beltsandcrashhelmets,andthesaferdesignanduseofroadsandvehicles.Reductioninroadtrafficinjuries cancontributetotheattainmentoftheMillenniumDevelopmentGoalsthataimtohalveextremepovertyand significantlyreducechildmortality.
Roadtrafficinjurypreventionmustbeincorporatedintoabroadrangeofactivities,suchasthedevelop-ment and manageRoadtrafficinjurypreventionmustbeincorporatedintoabroadrangeofactivities,suchasthedevelop-ment of road infrastructure, the provision of safer vehicles, law enforcement, mobility planning,theprovisionofhealthandhospitalservices,childwelfareservices,andurbanandenvironmental planning.Thehealthsectorisanimportantpartnerinthisprocess.Itsrolesaretostrengthentheevidence base,provideappropriatepre-hospitalandhospitalcareandrehabilitation,conductadvocacy,andcontribute totheimplementationandevaluationofinterventions.
Thetimetoactisnow.Roadsafetyisnoaccident.Itrequiresstrongpoliticalwillandconcerted,sustained effortsacrossarangeofsectors.Actingnowwillsavelives.Weurgegovernments,aswellasothersectorsof society,toembraceandimplementthekeyrecommendationsofthisreport.
LEEJong-wook JamesDWolfensohn
Director-General President
WorldHealthOrganization WorldBankGroup
P
ho
to
:©W
H
O
,P
.V
IR
O
T
P
ho
to
:©W
or
ldB
an
kP
ho
toL
Preface
Over3000Kenyansarekilledonourroadseveryyear,mostofthembetweentheagesof15and44years. ThecosttooureconomyfromtheseaccidentsisinexcessofUS$50millionexclusiveoftheactualloss oflife.TheKenyangovernmentappreciatesthatroadtrafficinjuriesareamajorpublichealthproblem amenabletoprevention.
In2003,thenewlyformedGovernmentoftheNationalAllianceRainbowCoalition,tookuptheroad safetychallenge.Itisfocusingonspecificmeasurestocurtailtheprevalentdisregardoftrafficregulations andmandatingspeedlimitersinpublicservicevehicles.
AlongwiththeabovemeasurestheGovernmenthasalsolaunchedasix-monthRoadSafetyCampaign anddeclaredwaroncorruption,whichcontributesdirectlyandindirectlytothecountry’sunacceptably highlevelsofroadtrafficaccidents.
IurgeallnationstoimplementtherecommendationsoftheWorldreportonroadtrafficinjurypreventionasa guidetopromotingroadsafetyintheircountries.Withthistoolinhand,Ilookforwardtoworkingwith my colleagues in health, transport, education and other sectors to more fully address this major public healthproblem.
MwaiKibaki,President,RepublicofKenya
In2004,WorldHealthDay,organizedbytheWorldHealthOrganization,willforthefirsttimebedevoted toRoadSafety.Everyyear,accordingtothestatistics,1.2millionpeopleareknowntodieinroadaccidents worldwide.Millionsofotherssustaininjuries,withsomesufferingpermanentdisabilities.Nocountryis sparedthistollinlivesandsuffering,whichstrikestheyoungparticularly.Enormoushumanpotentialis being destroyed, with also grave social and economic consequences. Road safety is thus a major public healthissuethroughouttheworld.
WorldHealthDaywillbeofficiallylaunchedinParison7April2004.Franceishonoured.Itseesthisas recognitionofthemajoreffortsmadebytheFrenchpopulationasawhole,whichmobilizedtoreducethe deathanddestructionitfacesontheroads.Theseeffortswillonlyachieveresultsiftheyaresupportedby agenuinerefusaltoacceptroadaccidentsfatalisticallyandadeterminationtoovercomeall-too-frequent indifference and resignation.The mobilization of the French Government and the relevant institutions, particularlycivicorganizations,togetherwithastrongaccidentpreventionandmonitoringpolicy,reduced trafficfatalitiesinFranceby20%,from7242in2002to5732in2003.Muchremainstobedone,butone thingisalreadyclear:itisbychangingmentalitiesthatwewill,together,managetowinthiscollectiveand individualstruggleforlife.
Globally deaths and injuries resulting from road traffic crashes are a major and growing public health problem.VietNamhasnotbeenspared.Intheyear2002,theglobalmortalityrateduetotrafficaccidents was19per100000populationwhileinVietNamthefigurewas27per100000population.Roadtraffic collisionsonthenation’sroadsclaimfivetimesmorelivesnowthantheydidtenyearsago.In2003atotal of20774incidentswerereported,leadingto12864deaths,20704injuriesandthousandsofbillionsof VietNamDongincosts.
AmaincontributortoroadcrashesinVietNamistherapidincreaseinthenumberofvehicles,particularly motorcycles, which increase by 10% every year. Nearly half of the motorcycle riders are not licensed, and three quarters don’t comply with traffic laws.Also, the development of roads and other transport infrastructurehasnotbeenabletokeeppacewithrapideconomicgrowth.
To reduce deaths and injuries, protect property and contribute to sustainable development, the Government ofViet Nam established the National Committee onTraffic Safety in 1995. In 2001 the Government promulgated the National Policy on Accidents and Injury Prevention with the target of reducingtrafficdeathsto9per10000vehicles.Governmentinitiativestoreducetrafficaccidentsinclude issuingnewtrafficregulationsandstrengtheningtrafficlawenforcement.In2003,thenumberoftraffic accidentswasreducedby27.2%overthepreviousyear,whilethedeathsandinjuryratesdeclinedby8.1% and34.8%respectively.
TheGovernmentofVietNamwillimplementmorestringentmeasurestoreduceroadtrafficinjuries throughhealthpromotioncampaigns,consolidationoftheinjurysurveillancesystem,andmobilization ofvarioussectorsatalllevelsandthewholesociety.TheGovernmentofVietNamwelcomestheWorld HealthOrganization/WorldBankWorldreportonroadtrafficinjuryprevention,andiscommittedtoimplementing itsrecommendationstothefullestextentpossible.
H.E.MrPhanVanKhai,PrimeMinister,SocialistRepublicofVietNam
InThailandroadaccidentsareconsideredoneofthetopthreepublichealthproblemsinthecountry.Despite theGovernment’sbestefforts,therearesadlyover13000deathsandmorethanonemillioninjurieseach year as the result of road accidents, with several hundred thousand people disabled.An overwhelming majorityofthedeathsandinjuriesinvolvemotorcyclists,cyclistsandpedestrians.
TheRoyalThaiGovernmentregardsthisproblemtobeofgreaturgencyandhasaccordedithighpriority inthenationalagenda.Wearealsoawareofthefactthateffectiveandsustainablepreventionofsuchinjuries canonlybeachievedthroughconcertedmultisectoralcollaboration.
To deal with this crucial problem, the Government has established a Road Safety Operations Centre encompassing the different sectors of the country and comprising the government agencies concerned, nongovernmental organizations and civil society. The Centre has undertaken many injury prevention initiatives,includinga“Don’tDrinkandDrive”campaignaswellasacampaigntopromotemotorcyclists towearsafetyhelmetsandtoengageinsafedrivingpractices.Inthisregard,wearewellawarethatsuch a campaign must involve not only public relations and education but also stringent law enforcement measures.
Theproblemofroadtrafficinjuriesisindeedahighlyseriousone,butitisalsoaproblemthatcanbe dealtwithandpreventedthroughconcertedactionamongallthepartiesconcerned.Throughtheleadership andstrongcommitmentoftheGovernment,weareconfidentthatwewillbesuccessfulinoureffortsand wehopethatotherswillbeaswell.
WearepleasedthattheSultanateofOman,withothercountries,hasbroughtuptheissueofroadsafetyto theUnitedNationsGeneralAssemblyandplayedamajorroleinraisingglobalawarenesstothegrowing impactofdeadlyroadtrafficinjuries,especiallyinthedevelopingworld.
The magnitude of the problem, encouraged the United Nations GeneralAssembly to adopt a special resolution (No 58/9) and theWorld Health Organization to declare the year 2004 as the year of road safety.
Intakingthesetwoimportantsteps,bothorganizationsstartedtheworldbattleagainsttraumacausedby roadaccidents,andwehopethatallsectorsofoursocietieswillcooperatetoachievethisnoblehumanitarian objective.
Theworldreportonroadtrafficinjurypreventionisnodoubtacompellingreadingdocument.Wecongratulatethe WorldHealthOrganizationandtheWorldBankforproducingsuchamagnificentpresentation.
QaboosbinSaid,SultanofOman
Landtransportationsystemshavebecomeacrucialcomponentofmodernity.Byspeedingupcommunications andthetransportofgoodsandpeople,theyhavegeneratedarevolutionincontemporaryeconomicand socialrelations.
However,incorporatingnewtechnologyhasnotcomeaboutwithoutcost:environmentalcontamination, urbanstressanddeterioratingairqualityaredirectlylinkedtomodernlandtransportsystems.Aboveall, transportationisincreasinglyassociatedwiththeriseinroadaccidentsandprematuredeaths,aswellas physicalandpsychologicalhandicaps.Lossesarenotlimitedtoreducedworkerproductivityandtrauma affecting a victim’s private life. Equally significant are the rising costs in health services and the added burdenonpublicfinances.
Indevelopingcountriesthesituationismadeworsebyrapidandunplannedurbanization.Theabsence ofadequateinfrastructureinourcities,togetherwiththelackofalegalregulatoryframework,makethe exponentialriseinthenumberofroadaccidentsallthemoreworrying.ThestatisticsshowthatinBrazil, 30000peopledieeveryyearinroadaccidents.Ofthese,44%arebetween20and39yearsofage,and82% aremen.
AsinotherLatinAmericancountries,thereisagrowingawarenessinBrazilastotheurgencyofreversing this trend.The Brazilian Government, through the Ministry of Cities, has put considerable effort into developingandimplementingroadsecurity,educationcampaignsandprogrammesthatemphasizecitizen involvement.AspartofthisendeavourBrazilrecentlyadoptedanewroadtrafficcodethathasbroughtdown theannualnumberofroaddeathsbyabout5000.Thisisawelcomedevelopmentthatshouldspurustoeven furtherprogress.Thechallengesareenormousandmustnotbesidestepped.Thisiswhyroadsecuritywill remainapriorityformyGovernment.
Thepublicationofthisreportisthereforeextremelytimely.Thedataandanalysisthatitbringstolight willprovidevaluablematerialforasystematicandin-depthdebateonanissuethataffectsthehealthof all.Ofevengreatersignificanceisthefactthatthereportwillhelpreinforceourconvictionthatadequate preventivemeasurescanhaveadramaticimpact.Thedecisiontodedicatethe2004WorldHealthDayto RoadSafetypointstotheinternationalcommunity’sdeterminationtoensurethatmodernmeansofland transportationareincreasinglyaforcefordevelopmentandthewell-beingofourpeoples.
Acknowledgements
The World Health Organization and the World Bank would like to acknowledge the members of the committees,regionalconsultationparticipants,peerreviewers,advisersandconsultants,fromover40 countries,whosededication,supportandexpertisemadethisreportpossible.
TheWorldHealthOrganization,theWorldBankandtheEditorialCommitteewouldliketopayaspecial tributetoPatriciaWaller,whopassedawayon15August2003.Shewasamemberofthetechnicalcommit-teeforchapter1butsadlybecametooilltoparticipate.Hermanycontributionstothepromotionofroad safetyinthecontextofpublichealthareacknowledged.Shewasafriendandmentortomany.
Thereportalsobenefitedfromthecontributionsofanumberofotherpeople.Inparticular,acknowledgement ismadetoJeanneBreenandAngelaSeayforwritingthereportunderverytighttimeconstraints,toTony Kahaneforeditingthefinaltext,toStuartAdamsforwritingthesummaryandDavidBreuerforeditingthe summary.Thanksarealsoduetothefollowing:CarolineAllsoppandMarieFitzsimmons,fortheirinvaluable editorialsupport;AnthonyBlissfortechnicalsupportontransport-relatedmatters;MeleckidzedeckKhayesi andTamitzaToroyan,forassistancewiththeday-to-daymanagementandcoordinationoftheproject;Kara McGeeandNielsTomijima,forstatisticalassistance;SusanKaplanandAnnMorgan,forproofreading;Tushita BosonetandSueHobbs,forgraphicdesignandlayout;LizaFurnivalforindexing;KeithWynnforproduction; Desiree Kogevinas, Laura Sminkey and Sabine van Tuyll van Serooskerken, for communications; Wouter Nachtergaele for assistance with references; Kevin Nantulya for research assistance; and Simone Colairo, PascaleLanvers-Casasola,AngelaSwetloff-Coff,foradministrativesupport.
Introduction
Roadtrafficinjuriesareamajorbutneglectedpub-lichealthchallengethatrequiresconcertedefforts foreffectiveandsustainableprevention.Ofallthe systemswithwhichpeoplehavetodealeveryday, roadtrafficsystemsarethemostcomplexandthe mostdangerous.Worldwide,anestimated1.2mil-lionpeoplearekilledinroadcrasheseachyearand asmanyas50millionareinjured.Projectionsindi-catethatthesefigureswillincreasebyabout65% overthenext20yearsunlessthereisnewcommit-ment to prevention. Nevertheless, the tragedy be-hindthesefiguresattractslessmassmediaattention thanother,lessfrequenttypesoftragedy.
TheWorldreportonroadtrafficinjuryprevention1isthe
firstmajorreportbeingjointlyissuedbytheWorld Health Organization (WHO) and theWorld Bank on this subject. It underscores their concern that unsafe road traffic systems are seriously harming globalpublichealthanddevelopment.Itcontends thatthelevelofroadtrafficinjuryisunacceptable andthatitislargelyavoidable.
Thereporthasthreeaims.
• Tocreategreaterlevelsofawareness,commit- mentandinformeddecision-makingatalllev- els–government,industry,internationalagen-ciesandnongovernmentalorganizations–so thatstrategiesscientificallyproventobeeffec- tiveinpreventingroadinjuriescanbeimple-mented.Any effective response to the global challenge of reducing road traffic casualties will require all these levels to mobilize great effort.
• To contribute to a change in thinking about the nature of the problem of road traffic
in- juriesandwhatconstitutessuccessfulpreven-tion.Theperceptionthatroadtrafficinjuryis thepricetobepaidforachievingmobilityand economic development needs to be replaced by a more holistic idea that emphasizes pre-ventionthroughactionatalllevelsoftheroad trafficsystem.
• To help strengthen institutions and to create effective partnerships to deliver safer road traffic systems. Such partnerships should ex-ist horizontally between different sectors of government and vertically between differ-ent levels of government, as well as between governmentsandnongovernmentalorganiza- tions.Atthegovernmentlevel,thismeanses-tablishingclosecollaborationbetweensectors, includingpublichealth,transport,finance,law enforcementandothersectorsconcerned. ThissummaryoftheWorldreportonroadtrafficinjury prevention is primarily intended for people respon-sibleforroadsafetypoliciesandprogrammesatthe nationallevelandthosemostcloselyintouchwith road safety problems and needs at the local level. Theviewsexpressedandtheconclusionsdrawnare takenfromthemainreportandthemanystudiesto whichthatreportrefers.
Apublichealthconcern
Everydayaroundtheworld,morethan3000peo-ple die from road traffic injury. Low-income and middle-income countries account for about 85% ofthedeathsandfor90%oftheannualdisability- adjusted life years (DALYs) lost because of road trafficinjury.
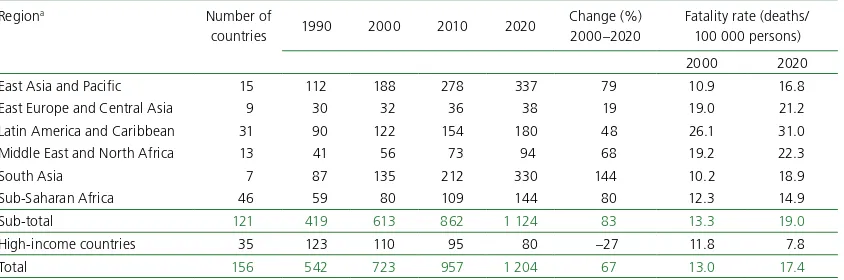
Projectionsshowthat,between2000and2020,
roadtrafficdeathswilldeclineby about30%inhigh-incomecoun-tries but increase substantially in low-income and middle-income countries. Without appropriate action,by2020,roadtrafficinju-ries are predicted to be the third leading contributor to the global burden of disease and injury (Table1)(1).
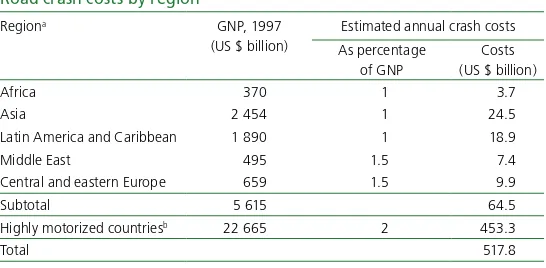
Thesocialandeconomic costsofroadtraffic injuries
Everyone killed, injured or dis-abledbyaroadtrafficcrashhasa networkofothers,includingfam-
ilyandfriends,whoaredeeplyaf-fected.Globally,millionsofpeoplearecopingwith thedeathordisabilityoffamilymembersfromroad trafficinjury.Itwouldbeimpossibletoattachaval-ue to each case of human sacrifice and suffering, addupthevaluesandproduceafigurethatcaptures theglobalsocialcostofroadcrashesandinjuries.
Theeconomiccostofroadcrashesandinjuriesis estimatedtobe1%ofgrossnationalproduct(GNP) inlow-incomecountries,1.5%inmiddle-income countries and 2% in high-income countries.The globalcostisestimatedtobeUS$518billionper year.Low-incomeandmiddle-incomecountriesac-countforUS$65billion,morethantheyreceivein developmentassistance(2).
Road traffic injuries place a heavy burden, not only on global and national economies but also householdfinances.Manyfamiliesaredrivendeep-lyintopovertybythelossofbreadwinnersandthe added burden of caring for members disabled by roadtrafficinjuries.
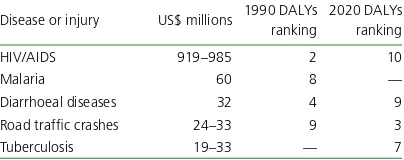
Bycontrast,verylittlemoneyisinvestedinpre-ventingroadcrashesandinjuries.Table2compares the funds spent on research and development fo-cused on several health concerns, including road safety.Comparativelylittleisspentonimplementa-tion, even though many interventions that would prevent crashes and injuries are well known, well tested,cost-effectiveandpubliclyacceptable.
Changingfundamental perceptions
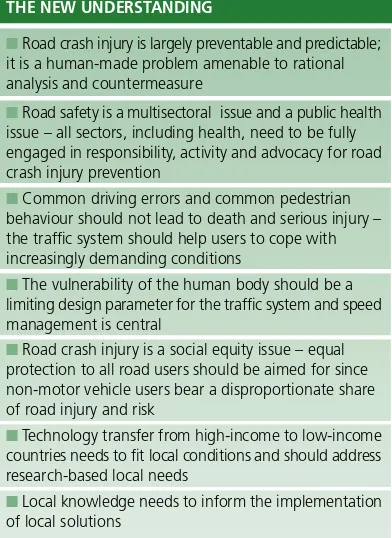
Since the last majorWHO world report on road safetyissuedover40yearsago(4)therehasbeen a major change in the perception, understanding andpracticeofroadinjurypreventionamongtraf-ficsafetyprofessionalsaroundtheworld.Figure1 setsouttheguidingprinciplesofthisshiftofpara-digms.
Thepredictabilityandpreventabilityof roadcrashinjury
Historically, motor vehicle “accidents” have been viewedasrandomeventsthathappentoothers(5) andasaninevitableoutcomeofroadtransport.The
term“accident”,inparticular,cangivetheimpres-TABLE2
Estimatedglobalresearchanddevelopment fundingforselectedtopics
Diseaseorinjury US$millions 1990DALYs ranking
2020DALYs ranking
HIV/AIDS 919–985 2 10
Malaria 60 8 —
Diarrhoealdiseases 32 4 9
Roadtrafficcrashes 24–33 9 3
Tuberculosis 19–33 — 7
Source:reference3. TABLE1
ChangeinrankorderofDALYsforthe10leadingcausesoftheglobal burdenofdisease
1990 2020
Rank Diseaseorinjury Rank Diseaseorinjury
1 Lowerrespiratoryinfections 1 Ischaemicheartdisease
2 Diarrhoealdiseases 2 Unipolarmajordepression
3 Perinatalconditions 3 Roadtrafficinjuries
4 Unipolarmajordepression 4 Cerebrovasculardisease
5 Ischaemicheartdisease 5 Chronicobstructivepulmonarydisease 6 Cerebrovasculardisease 6 Lowerrespiratoryinfections
7 Tuberculosis 7 Tuberculosis
8 Measles 8 War
9 Roadtrafficinjuries 9 Diarrhoealdiseases
10 Congenitalabnormalities 10 HIV
sionofinevitabilityandunpredictability–anevent thatcannotbemanaged.Thisisnotthecase.Road trafficcrashesareeventsthatareamenabletoratio-nalanalysisandremedialaction.
In the 1960s and early 1970s many highly-mo-torized countries began to achieve large reduc-tions in casualties through outcome-oriented and science-based approaches.This response was stimu-latedbycampaignersincludingRalphNaderinthe United States ofAmerica (6) and given intellectual strengthbyscientistssuchasWilliamHaddonJr(7).
Theneedforgooddataandascientific approach
Dataontheincidenceandtypesofcrashesaswellas adetailedunderstandingofthecircumstancesthat lead to crashes is required to guide safety policy. Knowledgeofhowinjuriesarecausedandofwhat typetheyareisavaluableinstrumentforidentify-inginterventionsandmonitoringtheeffectiveness of interventions. However, in many low-income
and middle-income countries, systematic efforts to collect road traffic data are not well developed andunderreportingofdeathsandseriousinjuriesis
Traditionally, road safety has been assumed to be theresponsibilityofthetransportsector.Intheearly 1960smanydevelopedcountriessetuptrafficsafe-ty agencies, usually located within a government’s transportdepartment.Ingeneral,however,thepub-lichealthsectorwasslowtobecomeinvolved(8,9). Butroadtrafficinjuriesareindeedamajorpub- lichealthissue,andnotjustanoffshootofvehicu-lar mobility.The health sector would greatly ben-efitfrombetterroadinjurypreventionintermsof
• discovering, through injury surveillance and surveys,asmuchaspossibleaboutallaspects ofroadcrashinjury–bysystematicallycollect- ingdataonthemagnitude,scope,characteris-ticsandconsequencesofroadtrafficcrashes;
• researchingthecausesoftrafficcrashesandin-juries,andindoingsotryingtodetermine: — causesandcorrelatesofroadcrashinjury, — factorsthatincreaseordecreaserisk, — factors that might be modifiable through
interventions;
• exploringwaystopreventandreducethese-verityofinjuriesinroadcrashesbydesigning,
ROAD INJURY PREVENTION AND CONTROL – THE NEW UNDERSTANDING
�Road crash injury is largely preventable and predictable; it is a human-made problem amenable to rational analysis and countermeasure
�Road safety is a multisectoral issue and a public health issue – all sectors, including health, need to be fully engaged in responsibility, activity and advocacy for road crash injury prevention
�Common driving errors and common pedestrian
behaviour should not lead to death and serious injury – the traffic system should help users to cope with increasingly demanding conditions
�The vulnerability of the human body should be a limiting design parameter for the traffic system and speed management is central
�Road crash injury is a social equity issue – equal protection to all road users should be aimed for since non-motor vehicle users bear a disproportionate share of road injury and risk
�Technology transfer from high-income to low-income countries needs to fit local conditions and should address research-based local needs
�Local knowledge needs to inform the implementation of local solutions
FIGURE1
implementing,monitoringandevaluatingap-propriateinterventions;
• helpingtoimplement,acrossarangeofsettings, interventionsthatappearpromising,especially intheareaofhumanbehaviour,disseminating information on the outcomes, and evaluating thecost-effectivenessoftheseprogrammes;
• working to persuade policy-makers and de-cision-makers of the necessity to address in-juriesingeneralasamajorissue,andofthe importanceofadoptingimprovedapproaches toroadtrafficsafety;
• translatingeffectivescience-basedinformation intopoliciesandpracticesthatprotectpedes-trians,cyclistsandtheoccupantsofvehicles;
• promotingcapacitybuildinginalltheseareas, particularly in the gathering of information andinresearch.
Cross-sectoralcollaborationisessentialhere,and this is something the public health sector is in a goodpositiontopromote.
Roadsafetyasasocialequityissue
Studiesshowthatmotorvehiclecrasheshaveadis-proportionate impact on the poor and vulnerable in society (10, 11). Poorer people comprise the majorityofcasualtiesandlackongoingsupportin theeventoflong-terminjury.Theyalsohavelim-ited access to post-crash emergency care (12). In addition, in many developing countries, the costs of prolonged medical care, the loss of the family bread winner, the cost of a funeral, and the loss ofincomeduetodisabilitycanpushfamiliesinto poverty(13).
Alargeproportionoftheroadcrashvictimsin low-incomeandmiddle-incomecountriesarevul-nerableroaduserssuchaspedestriansandcyclists. Theybenefitleastfrompoliciesdesignedformo-torizedtravel,butbearadisproportionateshareof the disadvantages of motorization in terms of in-jury,pollutionandtheseparationofcommunities.
Equalprotectionforallroadusersshouldbeaguid-ingprincipletoavoidanunfairburdenofinjuryand deathforpoorerpeopleandvulnerableroadusers(10, 14).Thisissueofequityisacentraloneforreducing theglobalburdenofroadcrashdeathandinjury.
Systemsthataccommodatehumanerror
The traditional view in road safety has been that roadcrashesareusuallythesoleresponsibilityofin-dividualroadusersdespitethefactthatmanyother factors beyond their control may have come into play,suchasthepoordesignofroadsorvehicles.But humanerrordoesnotalwaysleadtodisastrouscon-sequences.Humanbehaviourisgovernednotonly bytheindividual’sknowledgeandskills,butalsoby theenvironmentinwhichthebehaviourtakesplace (15 ).Indirectinfluences,suchasthedesignandlay-outoftheroad,thenatureofthevehicle,andtraffic lawsandtheirenforcementaffectbehaviourinim-portantways.Forthisreason,theuseofinformation andpublicityontheirownisgenerallyunsuccessful inreducingroadtrafficcollisions(8,16–18).
Systemsthataccountforthevulnerability ofthehumanbody
Theuncertaintyofhumanbehaviourinacomplex trafficenvironmentmeansthatitisunrealistictoex-pect that all crashes can be prevented. However, if greaterattentionindesigningthetransportsystem weregiventothetoleranceofthehumanbodytoin- jury,therecouldbesubstantialbenefits.Examplesin-cludereducingspeedinurbanareas,separatingcars andpedestriansbyprovidingpavements,improving thedesignofcarandbusfrontstoprotectpedestri- ans,andawell-designedandcrash-protectiveinter-facebetweentheroadinfrastructureandvehicles.
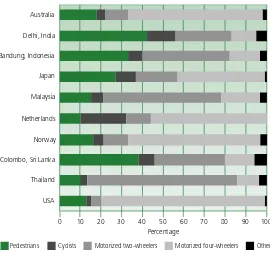
Technologytransferfromhigh-income countries
Transportsystemsdevelopedinhigh-incomecoun- triesmaynotfitwellwiththesafetyneedsoflow-incomeandmiddle-incomecountriesforavariety ofreasons,includingthedifferencesintrafficmix (19–21). In low-income countries, walking, cy-cling,motorcyclingandtheuseofpublictransport arethepredominanttransportmodes.Indeveloped countries,carownershipishigh,andmostroadus-ersarevehicleoccupants.
adaptationofprovenandpromisingmethodsfrom developed nations, and a pooling of information as to their effectiveness among other low-income countries(23).
Thenewmodel
Globally there is a need to improve the safety of thetrafficsystemforusers,andtoreducecurrent inequalitiesintheriskofincurringroadcrashin-juries.
Asystemsapproach
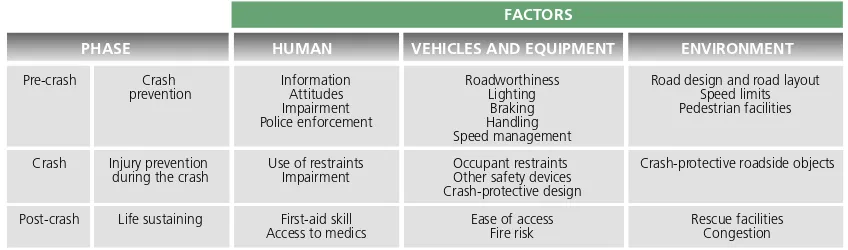
IntheUnitedStates,some30yearsago,William Haddon Jr described road transport as an ill- designed“man-machine”systemneedingcompre-hensivesystemictreatment(7).Heproducedwhat isnowknownastheHaddonMatrix,illustrating the interaction of three factors – human, vehicle andenvironment–duringthreephasesofacrash event:pre-crash,crashandpost-crash.Theresult-ingnine-cellHaddonmatrixmodelsthedynamic system,witheachcellofthematrixallowingop-portunities for intervention to reduce road crash injury(seeFigure2).Thisworkledtosubstantial advancesintheunderstandingofthebehavioural, road-related and vehicle-related factors that af-fectthenumberandseverityofcasualtiesinroad traffic.
Building on Haddon’s insights, the “systems” approach seeks to identify and rectify the major sourcesoferrorordesignweaknessthatcontrib-utetofatalandsevereinjurycrashes,aswellasto
mitigate the severity and consequences of injury by:
— reducingexposuretorisk;
— preventing road traffic crashes from occur-ring;
— reducingtheseverityofinjuryintheeventof acrash;
— reducingtheconsequencesofinjurythrough improvedpost-collisioncare.
Evidencefromsomehighly-motorizedcountries showsthatthisintegratedapproachtoroadsafety producesamarkeddeclineinroaddeathsandseri-ous injuries (8,24,25) but that the practical real-izationofthesystemsapproachremainsthemost importantchallengeforroadsafetypolicy-makers andprofessionals.
Developinginstitutionalcapacity
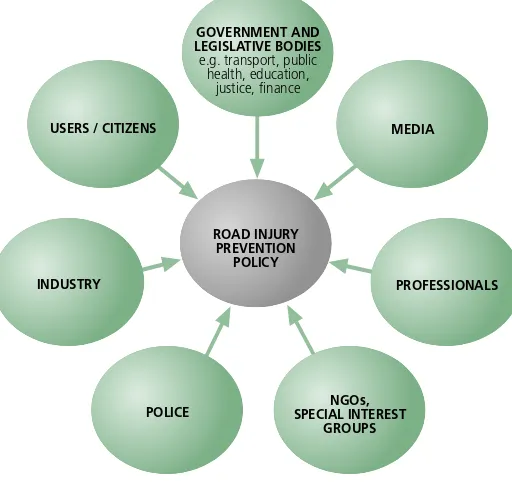
Thedevelopmentoftrafficsafetypolicyinvolvesa wide range of participants representing a diverse groupofinterests(seeFigure3).Thestructureand managementsystemsmayvary.InEuropeanUnion countries,forexample,nationalgovernmentsman-agemanyaspectsofroadsafety,buttheEuropean Unionregulatesmotorvehiclesafety.IntheUnited States, both the federal and state governments are responsibleforroadsafety.
Bogotá,thecapitalofColombia,hasapopulation of 7 million and provides an excellent example of roadsafetymanagement.Nationalandlocalauthori- ties,universitiesandcitizensworktogetheronman-agingroadsafetyandhaveachieveddramaticresults.
Pre-crash Crash Information Roadworthiness Road design and road layout
prevention Attitudes Lighting Speed limits
Impairment Braking Pedestrian facilities
Police enforcement Handling
Speed management
Crash Injury prevention Use of restraints Occupant restraints Crash-protective roadside objects
during the crash Impairment Other safety devices
Crash-protective design
Post-crash Life sustaining First-aid skill Ease of access Rescue facilities
Access to medics Fire risk Congestion
FACTORS
PHASE HUMAN VEHICLES AND EQUIPMENT ENVIRONMENT
FIGURE2
Theroleofgovernment
Historically,governmentalresponsibilitiesfortraf-fic safety fall within the transport ministry with othergovernmentdepartmentssuchaspolice,jus-tice, health, planning and education having some responsibility for key areas. Experience of several countries indicates that effective strategies for re-ducing traffic injury have a greater chance of be-ingappliedifthereisaseparategovernmentagency withthepowerandbudgettoplanandimplement its programme (8).Two examples of such agen-ciesaretheSwedishNationalRoadAdministration (SNRA) and the United States National Highway Traffic Safety Administration (NHTSA). Although stand-aloneagenciesarelikelytoincreasethepri-oritygiventoroadsafety,theyarenotasubstitute forstrongpoliticalsupportandactionsfromother agencies(26).
If the establishment of a stand-alone agency is notpossible,thenanalternativeistostrengthenthe existingroadsafetyunit,givingitgreaterpowers, responsibilityandauthoritywithinthegovernment transportministry(8).
ParliamentaryCommittees
Informed and committed politi-cians are essential to achieving government commitment to road safety,sincetheyauthorizepolicies, programmesandbudgets.Theyalso playcentralrolesindevelopingroad safetylegislation.
Two examples of this commit-mentinclude:
— theParliamentaryStandingCom- mitteeonRoadSafetyintheAustra-lianstateofNewSouthWaleswhich, intheearly1980s,wasresponsible fortheintroductionandfullimple-mentationofrandombreathtesting, which led to a 20% reduction in deaths(27);
— the Parliamentary Advisory Council for Transport Safety in the United Kingdom was responsible fortheintroductionoflegislationfor front seat-belt use in the 1980s, followed some years later by the introduction of speed humps and the use of rearseat-belts(28).
Research
Impartialresearchanddevelopmentonroadsafety isanessentialelementofanyeffectiveroadsafety programme.
Independentinstitutesthatcontributetounder-standing road safety issues include the Dutch In-stituteforRoadSafetyResearch,TRLLtd(formerly knownastheTransportResearchLaboratory)inthe UnitedKingdomandtheroadsafetyresearchunits at universities in Hanover, Germany andAdelaide and Melbourne, Australia. The United States has manyincludingtheNorthCarolinaHighwaySafety ResearchCenter,theUniversityofMichiganTrans-portationResearchInstituteandtheNationalCenter forInjuryPreventionandControlattheCentersfor DiseaseControlandPrevention.
TheTransportationResearchandInjuryPreven-tion Programme at the Institute ofTechnology in NewDelhi,IndiaandtheCentreforIndustrialand
POLICE SPECIAL INTERESTNGOs, GROUPS
PROFESSIONALS MEDIA GOVERNMENT AND
LEGISLATIVE BODIES e.g. transport, public
health, education, justice, finance
USERS / CITIZENS
INDUSTRY
ROAD INJURY PREVENTION
POLICY FIGURE3
Scientific Research and Development in SouthAf- ricahavebothcontributedtoidentifyinginterven-tions that can protect vulnerable road users, with specialattentiontointerventionsthatlow-income andmiddle-incomecountriescanafford.
Themostpracticalcourseofactionforlow-in-comeandmiddle-incomecountriesistoimportand adaptprovenandpromisingroadsafetytechnology fromothercountries.Doingthisrequireshavingthe capacity to conduct research into their own road trafficsystemsandtoidentifywhichoftheknown technologiesmaybeappropriateandwhatadapta-tionsmaybenecessary.Inaddition,uniquenational andlocalroadtrafficsituationsarelikelytorequire thedevelopmentofnewtechnologies.
Involvementofindustry
Industrysharesresponsibilityforroadsafetybyde-signingandsellingvehiclesandotherproducts,by usingroadtrafficsystemstodeliveritsproductsand byemployingpeoplewhouseroads.Recognizing thisresponsibility,industryhascontributedtoim-proving road safety. For example, Finland’s insur-ers’fundinvestigateseveryfatalroadtrafficinjury inthecountryandprovidestheresultingdatatothe Government of Finland and others with an inter- estinroadsafety.TheInsuranceInstituteforHigh-waySafetyintheUnitedStatesprovidesdataonthe crashperformanceofnewcarsandotherroadsafe-tyissuestogovernmentagenciesandindependent researchinstitutes.
Nongovernmentalorganizations
Nongovernmental organizations promote road safety by publicizing the problem of road traffic injury, identifying effective solutions, challenging ineffectivepoliciesandformingcoalitionstolobby forimprovedroadsafety(29).
TheTraumaCommitteeoftheRoyalAustralasian College of Surgeons advocates the best possible post-crashcareforinjuredpeople,propertraining in handling trauma cases for health professionals and gathering and reporting clinical data to en-hance the understanding of injuries (8). Mothers AgainstDrunkDrivingintheUnitedStateshassuc-cessfullylobbiedfortheenactmentofhundredsof
lawstocombatdrivingwhileundertheinfluence ofalcohol.TheEuropeanTransportSafetyCouncil, acoalitionofnongovernmentalorganizations,has had remarkable influence on the Road Safety and Technology Unit of the European Commission’s Directorate-General for Energy andTransport and ontheEuropeanParliament(28).
Some nongovernmental organizations in low- income and middle-income countries have difficultyinraisingfundsfortheireffortstocam-paign for road safety (26). However, several ac-tivenongovernmentalorganizationspromoteroad safety in these countries: for example,Asociación Familiares y Víctimas de Accidentes del Tránsito [Association of Families and Victims of Traffic Accidents] (Argentina), Friends for Life (India), Association for Safe International Road Travel (Kenya and Turkey), Youth Association for So-cialAwareness (Lebanon) and DriveAlive (South Africa).
Achievingbetterperformance Sharingresponsibility
Roadsafetyisbestachievedwhenallthekeygroups identifiedearlier(Figure3)shareacultureofroad safety(25,30).
Whenthereisacultureofroadsafety,thepro-vidersandenforcersofroadtrafficsystems(vehicle manufacturers, road traffic planners, road safety engineers, police, educators, health profession-als and insurers) take responsibility for ensuring that their products and services meet the highest possible standards for road safety. Road users take responsibility by complying with laws, informing themselves, engaging in safe road behaviour and engagingindiscussionanddebateaboutroadsafety issues,whetherindividuallyorthroughnongovern-mentalorganizations.
Responsibility requires accountability, and this necessitateswaysofmeasuringperformanceobjec-tively.
VisionZeroisaroadtrafficsystemwithzerofatali-tiesorsevereinjuriesthroughroadcrashes.Ithas publichealthasitsunderlyingpremise(31).
Vision Zero has a long-term strategy in which roadsafetyisimprovedgraduallyuntil,overtime,the ple of shared responsibility (32).
Launched in 1998, this strategy aimstoreduceroadtrafficdeaths by 50% and injuries by 40% by theyear2010.
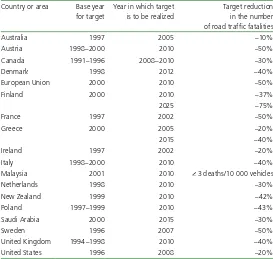
Settingtargets
Several studies (33, 34) have shownthatsettingtargetsforre-tious long-term targets are more effective than modest short-term ones(35)(Table3).
A prerequisite for setting tar-getsisgoodbaselinedataonroad trafficinjury,whichmeansthatan injurysurveillancesystemorsome other means of providing fairly complete and accurate informa- tionontheincidenceofroadtraf-ficinjurymustbeinplace.
Targets encourage people to identify all possible
interven-tions, to rank them according to the impact they areproventohaveontheincidenceofinjuryand thatinfluencesafety(36,37).Onefactortheyhave toconsideristhattheobjectiveofroadsafetyof- tenconflictswithotherobjectives,includingmo-bility and environmental conservation.They need toidentifypossiblebarrierstoimplementingroad safetymeasuresanddeterminehowthesebarriers mightbeovercome(38).
InNewZealand,theroadsafetyprogrammehas fourlevelsoftarget.
• The overall target is to reduce the social and economiccostsofroadcrashesandinjuries.
TABLE3
Examplesofcurrentfatalityreductiontargetsinusea
Countryorarea Baseyear fortarget
Australia 1997 2005 –10%
Austria 1998–2000 2010 –50%
Canada 1991–1996 2008–2010 –30%
Denmark 1998 2012 –40%
EuropeanUnion 2000 2010 –50%
Finland 2000 2010 –37%
2025 –75%
France 1997 2002 –50%
Greece 2000 2005 –20%
2015 –40%
Ireland 1997 2002 –20%
Italy 1998–2000 2010 –40%
Malaysia 2001 2010 <3deaths/10000vehicles
Netherlands 1998 2010 –30%
NewZealand 1999 2010 –42%
Poland 1997–1999 2010 –43%
SaudiArabia 2000 2015 –30%
Sweden 1996 2007 –50%
UnitedKingdom 1994–1998 2010 –40%
UnitedStates 1996 2008 –20%
aItshouldbenotedthatsomeofthesetargetsalsoincludereductionsinseriousinjury andaresupplementedbyothertargets,e.g.toreducethenumbersofcasualtiesamong children.
• Thesecondleveloftargetrequiresspecificre- ductionsinthenumbersofroadtrafficfatali-tiesandsevereinjuries.
• The third level consists of performance indi-catorsrelatedtoreducingspeed,reducingthe incidenceofdrivingwhileundertheinfluence ofalcoholandincreasingtheuseofseat-belts.
• The fourth level is concerned with institu-tionaloutput,includingthenumberofpolice patrol hours and the kilometres of high-risk crashsitestreatedtoreducerisk(37,39).
Buildingpartnerships
ThestateofVictoria,Australiahasdevelopedapart-nership between those responsible for road safety andthoseinvolvedincompensationforinjury.The TransportAccidentsCommissioncompensatesroad crashsurvivorsthroughano-faultinsurancesystem fundedbypremiumsleviedaspartofannualvehicle registrationcharges.TheCommissioninvestsheavily inimprovingroadsafety,knowingthatitsinvestment willbemorethanoffsetbysavingsinthecompensa-tion it pays out.Three government ministers – re- sponsiblefortransport,justiceandinsurance–joint-lysetthepolicyandcoordinatetheprogramme.
The province of KwaZulu-Natal, in South AfricahastransferredandadaptedtheVictoriastate model(40).
TheUnitedKingdomDepartmentforTransport encourages local partnerships in which the
de-partmentandlocalauthorities,police,courtsand sometimes health authorities work together on enforcingspeedlimitsandrecoveringthecostsof this.Overthefirsttwoyears,pilotstudieslaunched in2000havereducedtheincidenceofroadcrash by35%andtheincidenceoffatalandseriousin- jurytopedestriansby56%.Thesavingsonadmin-isteringservicestoroadcrashsurvivorshavefreed upabout£20milliontobeinvestedinotherways. Theeconomicbenefittosocietyisestimatedtobe about£112million(41).
The New CarAssessment Programme (NCAP) wasestablishedintheUnitedStatesin1978.Un-der the programme, manufacturers, buyers and governmentcooperate,subjectingnewcarmodels to a range of crash tests and rating their perfor- mancewitha“star”system.ThereisnowanAus-tralianNCAPandaEuropeanonecalledEuroNCAP. ThepartnersinEuroNCAPincludenationaltrans-portdepartments,automobileclubs,theEuropean Commissionand,onbehalfofcarbuyers,Interna-tionalConsumerResearchandTesting.InEurope, research (42) has shown that, in car-to-car colli-sions,carsratedwiththreeorfourstarsareabout 30%saferthanoneswithtwostarsorfewer.
Global,regionalandcountry estimates
Longbeforecarswereinvented,roadtrafficinjuries occurred involving carriages, carts, animals and people.The numbers grew exponentially as cars, buses, trucks and other motor vehicles were introduced and became ever more common. A cyclist in NewYork City was the first recorded case of injury involving a motor vehicle on 30 May1896,andaLondonpedestrianwasthefirst recordedmotorvehicledeathon17Augustofthe sameyear(43).Thecumulativetotalofroadtraffic
deaths had reached an estimated 25 million by 1997(44).
In2002,anestimated1.18millionpeopledied fromroadtrafficcrashes:anaverageof3242deaths perday.Roadtrafficinjuriesaccountedfor2.1%of allglobaldeaths,makingthemtheeleventhleading causeofglobaldeaths.
Inadditiontodeaths,anestimated20millionto 50millionpeopleareinjuredinroadcrasheseach year (2, 45). In 2002, an estimated 38.4 million DALYswerelostbecauseofroadcrashes,or2.6% ofallDALYslost.Thismaderoadtrafficinjuriesthe
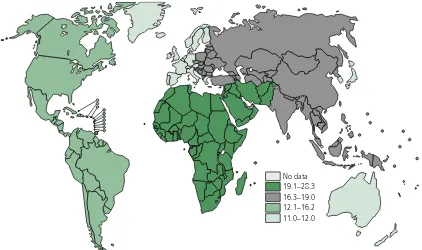
Theglobalimpact
Source:WHOGlobalBurdenofDiseaseproject,2002,Version1.
No data 19.1–28.3 16.3–19.0 12.1–16.2 11.0–12.0 FIGURE4