Knut-OlafHaustein† • DavidGroneberg
Tobacco or Health?
Nikotinforschungund Raucherentwöhnung JohannesStr.85–87 99084Erfurt Germany
InstitutfürArbeitsmedizin Thielallee73
14195Berlin Germany
david.groneberg@charite.de
ISBN:978-3-540-87576-5 e-ISBN:978-3-540-87577-2
DOI:10.1007/978-3-540-87577-2
SpringerHeidelbergDordrechtLondonNewYork
LibraryofCongressControlNumber:2009931695 ©Springer-VerlagBerlinHeidelberg2010
Thisworkissubjecttocopyright.Allrightsarereserved,whetherthewholeorpartofthematerialis concerned,speciicallytherightsoftranslation,reprinting,reuseofillustrations,recitation,broadcasting, reproductiononmicroilmorinanyotherway,andstorageindatabanks.Duplicationofthispublication orpartsthereofispermittedonlyundertheprovisionsoftheGermanCopyrightLawofSeptember9, 1965,initscurrentversion,andpermissionforusemustalwaysbeobtainedfromSpringer.Violations areliabletoprosecutionundertheGermanCopyrightLaw.
Theuseofgeneraldescriptivenames,registerednames,trademarks,etc.inthispublicationdoesnot imply,evenintheabsenceofaspeciicstatement,thatsuchnamesareexemptfromtherelevantprotective lawsandregulationsandthereforefreeforgeneraluse.
Productliability:Thepublisherscannotguaranteetheaccuracyofanyinformationaboutdosageand applicationcontainedinthisbook.Ineveryindividualcasetheusermustchecksuchinformationby consultingtherelevantliterature.
Coverdesign:eStudioCalamar,Figueres/Berlin Printedonacid-freepaper
v
Dedication
vii
Thisbookcomprehensivelysummarizestheadverseeffectsoftobaccosmokingonhuman health.Thecurrentsecondeditionhasintegratedalargesetofnewdatathathavebeen publishedinnumerousscientiicstudiesandmeta-analysesoverthepastfewyears.
Unfortunately,theharmfulsequelaeoftobaccosmokingareplayeddownbytheindus-tryandpoliticiansinmanyindustrializedcountries.However,about800,000people/year intheEUdiefromtheimmediateconsequencesofsmoking.Theparticularlyinsidious featureoftobaccoconsumptionisthatsmoking-attributableharmfuleffectsonhealthdo notgenerallybecomeapparentuntilthreeorfourdecadesaftersmokinginitiation.
Althoughsomepositivechangesinthelegislativehandlingoftobaccohaveappearedin thepastiveyears,westillneedtoformapact,sealedbypoliticians,themedicalprofes-sionals,teachersandthemedia,totargettheproblemacrossnations.Inthisrespect,a minorityofcountries,includingtheUSandtheUK,havegivenpositiveexamples.
Therearefourareasthatneedtobeimprovedinfuture:(1)strictbansontobaccoadver-tisementonagloballevel,(2)bettermeasurestoprotectagainstside-stream(passive)smoke exposure,(3)establishmentofpreventionprograms,especiallyforchildrenand(4)treat-mentoftobaccoaddiction.
WhilepreparingthesecondeditionoftheGermanversionofthisbook,thefounding authorKnut-OlafHausteindeceased.AfterthefalloftheBerlinwall,hewasoneoftheirst GermanstotakeanactivepartinthebattleagainsttobaccointheunitedGermanyanditis theauthor’shopethatthepresenteditioncontinuesthethoughtsofKnut-OlafHausteinon howtoapproachthenumerousproblems.Asacomprehensivework,thebookisintended tomeettheneedsofalargereadership,includingallmedicalprofessionalsandscientists, aswellasteachers,sociologists,themediaandpoliticians.
Firstandforemost,Iamgratefultoallthescientistswhoprovidedthedata.Ialsogladly acknowledgethehelpofSpringer,Heidelberg,andtheassistanceofDr.CarolinKreiter, Dr.Julia-AnikBörger,Dr.DavidQuarcoo,Dr.AlexanderGerber,BiancaKusma,Stefania Mache,KarinVitzthumandSilvanaKölzow.Withoutthehelpofmyfamilyandthefamily ofKnut-OlafHaustein,thisbookcouldnothavebeenrealized.
Itrustthatthisbookwillmeetwithagoodreceptionbothwithinandoutsidetheieldof medicine.
ix
Contents
1. HistoryofTobacco... 1
1.1 TobaccoPlantsandTheirOrigin... 1
1.2 UseofTobaccoforReligiousPurposes... 1
1.3 TheAppropriationofTobaccobyEuropeans... 2
1.4 WorldwideSpreadofTobacco... 3
1.4.1 DevelopmentoftheCigar... 5
1.4.2 DevelopmentoftheCigarette... 5
1.5 ObjectionstoSmokingonHealthGrounds... 7
1.6 WomenWonOverbytheCigarette... 8
1.7 TheMedicalUseofTobaccointheNineteenthCentury... 12
1.8 TobaccoResearchintheTwentiethCentury... 12
1.9 ConcludingRemarks... 14
2. EpidemiologyofTobaccoDependence... 17
2.1 TobaccoConsumptionintheTwentiethCentury... 18
2.2 CigaretteSmokingintheUSAsince1965... 19
2.3 SmokingHabitsinGermany... 20
2.4 Cigarette-RelatedMortalityinDifferentCountries... 22
2.5 OtherFormsofTobaccoUse... 25
2.6 SmokersandOtherRiskFactors... 27
2.7 SmokingBehaviourandEducationalLevelintheEU... 28
2.8 ConcludingRemarks... 30
3. TobaccoConstituentsandAdditives... 35
3.1 Non-DisclosureofFindingsbytheTobaccoIndustry... 35
3.2 ConstituentsofTobacco... 36
3.3 NicotineandDependence... 40
3.3.1 TheCigaretteasaVehicleforNicotineRelease... 41
3.3.2 ModiicationsofNicotineRelease... 41
3.3.3 MaintainingNicotineDependence... 42
3.3.4 MarketingofCigaretteswitha“Reduced”HealthRisk... 43
3.3.5 CompensatoryBehaviourbySmokers... 43
3.3.7 ImportanceofAbsorptionRate... 45
3.3.8 AmmoniumandpHManipulation... 45
3.4 TobaccoAdditives... 46
3.5 CigaretteswithReducedTarYield... 48
3.6 SnuffTobacco... 50
3.7 ConcludingRemarks... 55
4. PharmacologyandPharmacokineticsofNicotine... 61
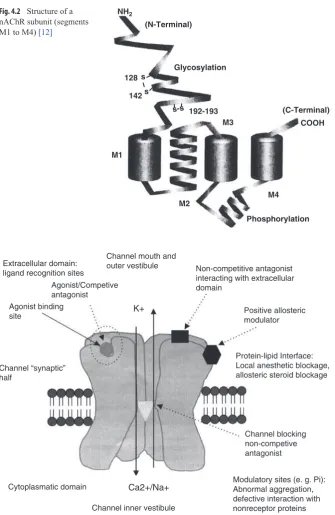
4.1 TheNicotineReceptor... 61
4.2 AgonistsandAntagonistsofthenAChRanditsSubtypes... 65
4.3 Pharmacology... 66
4.3.1 EffectsofNicotineonReceptorsinDifferentOrgans... 66
4.3.2 OrganEffectsandToxicity... 67
4.3.3 MetabolicandHormonalEffectsofNicotine... 68
4.3.4 CentralNervousSystemEffectsofNicotine... 68
4.4 PharmacokineticsofNicotine... 69
4.5 NicotineDependence... 73
4.5.1 TypesofDependence... 73
4.5.2 MolecularBiologicalAspectsofDependence... 75
4.5.3 GeneticAspects... 77
4.5.4 WithdrawalSymptoms... 79
4.6 ConcludingRemarks... 80
5. SmokingandLungDisease... 87
5.1 ImmunologicalReactionsCausedbyCigaretteSmoking... 87
5.2 CigaretteSmokingandLungCancer... 88
5.2.1 AssociationBetweenSmokingandLungCancer... 90
5.2.2 TypesofLungCancer... 91
5.2.3 GeneticFactorsThatIncreasetheRiskforBronchialCarcinoma... 93
5.3 CigaretteSmokingandCOPD... 99
5.3.1 PathophysiologyofCOPD... 100
5.3.2 ImportantRiskFactorsforCOPD... 102
5.4 CigaretteSmokingandBronchialAsthma... 103
5.4.1 CaveatsConcerningtheInformativeValueofStudies... 103
5.4.2 CigaretteSmokingandBronchialAsthmainAdults... 103
5.4.3 BronchialAsthmainChildren... 104
5.5 BronchitisandPneumonia... 106
5.6 OtherLungDiseasesInluencedbyCigaretteSmoking... 107
5.7 ConcludingRemarks... 107
6. CardiovascularDisease,DisturbancesofBlood CoagulationandFibrinolysis... 119
6.1 CoronaryArteryDiseaseandMyocardialInfarction... 119
6.2 SystemicVascularChanges... 123
Contents xi
6.2.2 ChangesinEndothelialFunction
andMicrocirculation... 129
6.2.3 MicrocirculationandO2Supply... 130
6.2.4 ArterioscleroticandInlammatoryVascularReactions... 134
6.3 BloodCoagulationandFibrinolysis... 135
6.3.1 GeneticFactors... 136
6.3.2 NicotineandIschaemicHeartDisease... 136
6.4 ConcludingRemarks... 137
7. OtherOrganSystems... 149
7.1 CentralNervousSystem... 149
7.1.1 CognitiveImpairment... 150
7.1.2 InluenceonCognitivePerformance... 151
7.1.3 IntellectualImpairmentinChildhood... 152
7.1.4 SmokerPersonalityProilesandGeneticInheritanceofSmoking... 154
7.1.5 Depression... 155
7.1.6 Schizophrenia... 157
7.1.7 EffectsofSmokinginFormsofDementia... 159
7.1.8 SmokingandParkinson’sDisease... 160
7.2 OcularDiseases... 161
7.2.1 DiabeticRetinopathy... 161
7.2.2 CataractandLensOpacity... 162
7.2.3 Graves’Ophthalmopathy... 163
7.2.4 MacularDegeneration... 163
7.2.5 Glaucoma... 164
7.2.6 Strabismus... 164
7.2.7 OcularTumours... 164
7.2.8 RetinalDetachment... 165
7.3 Ears,OralCavityandLarynx... 165
7.3.1 HarmfulEffectsontheEars... 165
7.3.2 ChangesintheOralCavity... 165
7.3.3 OralandLaryngealCancer... 166
7.4 DisordersofLipidandGlucoseMetabolism... 167
7.4.1 LipidandCholesterolMetabolism... 167
7.4.2 DiabetesandSmoking... 169
7.5 GastrointestinalTract... 173
7.5.1 OesophagealCancer... 173
7.5.2 GastrointestinalUlcers... 174
7.5.3 CancersoftheGastrointestinalTract... 175
7.5.4 PancreaticCancer... 175
7.6 UrinaryTractDiseases... 176
7.6.1 ToxicSubstancesandInducers... 177
7.6.2 KidneyCancer... 178
7.6.3 BladderCancer... 179
7.6.5 ProstaticHyperplasiaandProstaticCancer... 180
7.6.6 FertilityDisorders... 181
7.7 DisordersofMineralMetabolismandBone... 182
7.7.1 VitaminDandOestrogenMetabolism... 182
7.7.2 Osteoporosis... 183
7.7.3 HipFractures... 185
7.8 SkinandMucosa... 185
7.8.1 SkinChanges... 186
7.8.2 Psoriasis... 187
7.8.3 SkinTumours... 188
7.8.4 BreastCancer... 188
7.9 HaematopoieticSystem... 189
7.10 ConcludingRemarks... 191
8. SmokingandPregnancy... 221
8.1 EffectsofSmokingonthePlacenta... 222
8.2 ComplicationsofPregnancy... 224
8.3 MalformationsPossiblyCausedbySmoking... 227
8.4 SmokingandSuddenInfant DeathSyndrome(SIDS)... 230
8.5 FoetotoxicEffectsofCO... 232
8.6 EffectsofNicotineontheFoetus... 233
8.7 SmokingandBreast-feeding... 234
8.8 MedicalCareCostsAttributable toSmokingDuringPregnancy... 236
8.9 ConcludingRemarks... 236
9. PassiveSmoking... 247
9.1 ETSintheWorkplaceandatHome... 250
9.2 ChangesattheMolecularandCellularLevel... 252
9.2.1 Fibrinogen... 253
9.2.2 Cholesterol... 253
9.2.3 EndotheliumandPlatelets... 253
9.2.4 MarkersofInlammation... 254
9.2.5 ETSandDrugMetabolism... 256
9.3 PassiveSmokingDuring andAfterPregnancy... 256
9.4 CardiovascularDisease... 258
9.4.1 CoronaryHeartDisease... 258
9.4.2 Arteriosclerosis... 260
9.4.3 StrokeandSubarachnoidHaemorrhage... 262
9.5 RespiratoryTract... 263
9.5.1
RespiratoryTractinChildrenandTeenagers... 2639.5.2
BronchialCarcinoma... 267Contents xiii
9.7 OtitisMedia... 271
9.8 MeningococcalInfections... 273
9.9 BreastCancer... 273
9.10 PsychosocialChanges... 274
9.11 ConcludingRemarks... 275
10.Non-DrugTreatmentstoPromoteSmokingCessation... 289
10.1 IndicationsandDiagnosticConsiderations... 291
10.2 ObjectiveofTreatment... 292
10.3 Self-HelpInterventionsbytheSmoker... 293
10.4 PhysicianAdviceforSmokingCessation... 295
10.5 NursingInvolvement... 297
10.6 GroupBehaviourTherapyProgrammes... 297
10.7 AversionTherapy... 298
10.8 MassMediaCommunicationStrategies... 299
10.9 Hypnosis... 302
10.10 Acupuncture... 302
10.11 ReducedSmoking... 303
10.12 Pregnancy... 303
10.13 E-Learning,EmailandInternetforSmokingCessation... 304
10.14 ConcludingRemarks... 304
11.PharmacotherapyofNicotineDependence... 311
11.1 Nicotine... 311
11.1.1 EvaluationofNicotineProducts... 314
11.1.2NicotineChewingGum... 315
11.1.3 NicotinePatch... 316
11.1.4 NicotineSublingualTablet... 317
11.1.5 NicotineNasalSpray... 317
11.1.6 NicotineInhaler... 318
11.1.7 NicotineLozenge... 318
11.1.8 TreatmentandDosage... 319
11.1.9 AdverseEventsAssociatedwithNRT... 321
11.1.10WithdrawalSymptoms... 324
11.1.11DrugInteractionsDuringSmokingCessation... 324
11.1.12ContraindicationsfortheUseofNicotineProducts... 325
11.1.13NicotineFormulationsasOTCProducts... 325
11.2 Bupropion... 328
11.2.1 Pharmacodynamics... 328
11.2.2 PharmacokineticProperties... 329
11.2.3 TherapeuticEficacy... 330
11.2.4 Dosage... 331
11.2.5 AdverseEffects... 332
11.2.6 ContraindicationsandDrugInteractions... 333
11.3 OtherPharmacotherapies... 334
11.3.1 Varenicline... 334
11.3.2 Nortriptyline... 335
11.3.3 Clonidine... 335
11.3.4 Mecamylamine... 336
11.3.5 Tranquillisersandb-ReceptorBlockers... 336
11.3.6 Buspirone... 336
11.3.7 Rimonabant... 337
11.3.8 VariousAntidepressants... 337
11.3.9 OpioidAntagonists... 338
11.3.10Lobeline... 338
11.3.11SilverAcetate... 339
11.3.12Nicotine-Vaccination... 339
11.4 TherapeuticMonitoringinSmokingCessation... 339
11.5 SpecialTherapeuticSituations... 340
11.5.1 IschaemicHeartDisease... 340
11.5.2 Pregnancy... 341
11.5.3 WeightGain... 342
11.5.4 AlcoholConsumption... 342
11.5.5 OrganicDepressionandSchizophrenia... 342
11.5.6 Pre-operativeSmokingCessation... 345
11.6 ConcludingRemarks... 346
12.PrimaryPrevention... 359
12.1 SmokingInitiation... 360
12.2 ReasonsforSmoking... 362
12.3 PrimaryPreventionProgrammes... 363
12.3.1 PreventionProgrammesforSchools... 364
12.4 “BeSmart:Don’tStart”... 367
12.5 Class2000HealthPromotionProgramme... 370
12.6 TrierUniversityHealthProgramme... 371
12.7 Long-TermStudies... 371
12.8 RoleofTeachersinPrimaryPrevention... 373
12.9 PreventionbyRestrictingSalesofTobaccoProductstoMinors... 374
12.10 RoleoftheMassMediainSalesofTobaccoProductstoAdolescents... 376
12.11 RoleofGovernmentandCommunityinPrimaryPrevention... 378
12.12 ConcludingRemarks... 379
13.TobaccoIndustry,AdvertisingandAdvertisingBans... 387
13.1 TobaccoAdvertisingStrategies... 388
13.2 AdvertisingMessages... 392
13.3 EffectofTobaccoIndustryAdvertisingMessages... 393
13.4 TobaccoAdvertisingandAdolescentSmokingInitiation... 396
13.5 Advertisingwith“Light”Cigarettes... 398
Contents xv
13.7 EffectofAdvertisingBans... 401
13.8 SmokingBansinPublicBuildingsandPublicSpaces... 403
13.9 ConcludingRemarks... 404
14.Society,PoliticsandtheTobaccoIndustry... 411
14.1 TobaccoIndustry,GovernmentalandNon-governmentalOrganisations 412 14.2 PoliticiansandTheirAttitudetoSmoking... 414
14.3 ScientistsandtheTobaccoIndustry... 415
14.4 “Subsidised”TobaccoGrowing... 416
14.5 GovernmentalControlofToxicTobaccoConstituents... 418
14.6 TobaccoTaxes... 419
14.7 RegulationsonSmoking... 420
14.8 BansonAdvertisinginVariousCountries... 422
14.9 TobaccoIndustry:PlayingDowntheRisksofSmoking andPassiveSmoking... 423
14.10 SmokingandNon-smoking:WeighingtheBeneits... 424
14.11 ConcludingRemarks... 426
15.Appendix:Experiencesfrom aSmokerCounsellingCentre... 433
15.1 TreatmentStrategy... 433
15.2 TheCounsellingProcess... 434
15.3 ExperienceswithOutpatientSmokerCounselling... 435
15.4 SuccessinSmokingCessation... 436
15.5 ConcludingRemarks... 436
1 K.-O.Haustein,D.Groneberg,TobaccoorHealth?
DOI:10.1007/978-3-540-87577-2_1,©SpringerVerlagBerlinHeidelberg2010
1
Weliketolookinthefuture,becausetheundeterminedinit,whichmaybeaffectedthisorthat way,wefeelasifwecouldguidebyoursilentwishesinourownfavour.
(J.W.Goethe,Novelsandtales.1854)
1.1
Tobacco Plants and Their Origin
Nicotianatabacum,thetobaccoplantusedsinceancienttimesintheCentralandSouth America,doesnotoccurnaturallybutisaproductofhumancultivation[1],beingahybrid ofNicotianasylvestrisandNicotianatomentosifosa[2].Nicotianarustica(developedlater inRussiaasmachorka)wasthevarietycultivatedinNorthAmerica,andhasahighernico-tinecontentthantheothertobaccoplants.Illustrationsoftobaccoplantappearedunderthe nameofNicotianamajorintheseventeenth-centuryherbals(Fig.1.1)becausetobacco wasbelievedtopossesshealingproperties[3].Thenicotinecontentofthetobaccoleaves isincreasediftheleadingstemoftheplantanditslateralshootsareremoved(aprocess knownas“toppingandsuckering”),anddryingimprovesthelavouroftheleaves[1].The juiceoflimeisusedtoenhancethelavourofsometobaccovarieties[4] ,andinthepro-cessthenicotinereleaseasafreebaseisimproved[5].
1.2
Use of Tobacco for Religious Purposes
2 1 History of Tobacco
ina“peace-pipe”tosetthesealontreatiesandfriendships,whilethoseofCentraland SouthAmericausedtobaccoinarolledform,rathersimilartopresent-daycigarsandciga-rettes.Thesepeoplealsoattributedthehealingpropertiestothetobaccoplant(forexample, theshamanormedicinemanwouldapplytobaccoleavestowounds).InSouthAmerica, tobaccowasusedpreferentiallyformedicinalpurposes,butitwasalsotakenassnuff, chewed,andusedasaliquidbrew.Theappetite-suppressingqualityoftobaccowasrecog-nisedevenatthattime.BeyondtheAmericancontinent,tobaccoplantswerefoundonlyin Australia,andinsomepartsoftheSundaIslandsofIndonesia.
1.3
The Appropriation of Tobacco by Europeans
Forobviousreasons,untilColumbuslandedonSanSalvadorin1492,thetobaccoplant didnotattracttheinterestofEuropeans,althoughitmaybenotedthattheAmerindians usedthewordtabagotodescribethepipeusedfortobaccosmokingratherthantheplant itself.OnhissecondvoyagetotheNewWorld,Columbuswaspresentedwithabunchof tobaccoleaves,buthadnoinklingoftheirintendeduse.In1527,theirstbishopofthenew
Fig. 1.1Illustrationofatobaccoplantfromthe
colony,FrayBartolomédeLasCasas,wroteadescriptionofthepropertiesofthetobacco plant[7]. Although the Amerindians presented the Spaniards with tobacco leaves as a gestureoffriendshipanddevotion,theplantlostallitsceremonialreligioussigniicance overtheensuingcenturiesinthehandsoftheSpaniardsandotherEuropeans,andtobacco becamealuxurycommoditythatwasexploitedsolelyforcommercialpurposes.
Afterhisreturnfromseavoyages,SpaniardRodrigodeJerez–creditedwithbeingthe irstEuropeantobaccosmoker–usedtowalkthestreetsofhishomeportofAyamonte, withsmokebillowingfromhismouthandnose.Believinghewasconsortingwiththe Devil,thelocalclergyhandedRodrigoovertotheInquisition,andhewasimprisonedfor 10years!ThiswasinstarkcontrasttotheextremelyliberalattitudeoftheSpanishcolonial rulersoutsideSpainasfarastobaccosmokingwasconcerned.Afterhissecondvoyageto theNewWorld,ColumbusbroughtanumberoftobaccoplantsbacktoSpainwherethey were used initially as ornamental plants in the gardens of the aristocracy. Jean Nicot (1530–1600),FrenchambassadortothePortuguesecourt,conductedanumberof“experi-ments”whichidentiiedthehealingeffectsoftobacco.In1559,onthestrengthofthis conviction,hesentsomeplantstoParisforCatherinedeMediciwhohadthemprocessed assnuffpowder,andsuccessfullyadministeredthemtoherson,CharlesIX,asaremedy forhisheadaches[8].TheSpaniardNicolasMonardes,aphysicianattheUniversityof Seville,wroteatreatisein1571onthemedicinaluseoftobacco,andhiscompendiumwas veryrapidlytranslatedintootherlanguages[9].By1590,theplantwasalreadyknownas Nicotiana,andsince1828Nicothasgivenhisnametotheprincipalalkaloid,nicotine.
TobaccoarrivedattheEnglishcourtofQueenElizabethIin1573,andby1614therewere alreadymorethan7,000tobaccoretailoutletsinLondon[10].Beneitingfromtheextensive tradingrelationshipswiththeSpaniardsandthePortuguese,thetobaccoplantwascarriedto thePhilippines,totheSoutheastandEastAsia,aswellastoAfricaand,bythebeginningof theseventeenthcentury,evenfurtheraieldtoJapan,KoreaandChina,fromwhereitalso enteredTibet,Mongolia,andSiberia[11] .Tobaccobecameanimmenselyvaluablecom-mercialcommodity,comparablewithcocaineandotherillegaldrugsatthepresenttime.
1.4
Worldwide Spread of Tobacco
4 1 History of Tobacco
Smokingclubsbecameincreasinglycommonplace.HenryBunbury’setchingASmoking Club(Fig.1.2)depictsfourgentlemenofdifferingbuildenjoyingtheritualpleasuresofthe pipe.Theyadoptedanalmoststatuesquepose,andtheirexaggeratedlookofrapturehad somethingridiculousaboutit.Frowneduponforalongperiod,theactivityofsmokingwas condemned, and was restricted to the lower social strata (soldiers), becoming socially acceptableonlytowardtheendoftheeighteenthcentury.Normally,smokingwaspermitted only in speciically designated rooms; the ban on smoking in public persisted in many placesuntilthenineteenthcentury.
Inadditiontotobaccosmoking,thepracticeofsnufftaking(witnessedbytheSpaniards during their seafaring voyages of discovery) was also taken from the Amerindians. InFrance,snufingwaswidespreadbeforetheFrenchRevolution,withsome90%oftobacco beingconsumedinthisway.Thetabatière orsnuffboxwasthestatussymbolofthearistoc-racy.Asaresult,olfactorydisturbancesortotallossofthesenseofsmellwerewidespread intheeighteenthcentury,particularlyinFrance.Bycontrast,thechewingoffermented tobaccoleaveswaslesscommon,eventhoughitwasclaimedtoalleviatethepangsofhun-ger. In Europe, the custom of tobacco chewing survived longest among seafarers and
Fig. 1.2ASmokingClub.EtchingfromanoriginalbyBunburyEsq.(1750–1811),inS.W.Fores
mineworkers.In1742,KingFredericktheGreatofPrussiaissuedanedict“againsttobacco smokingasariskofire”whichwasnotcompletelyrepealeduntil1848.
1.4.1
Development of the Cigar
Cigarswerethecommonestformofprocessedtobaccointheeighteenthcentury,with theearliesttabacerias fortheproductionofcigarshavingemergedinSpaininthesev-enteenthcentury.IntheUSAinthenineteenthcentury,twovarietiesoftobaccowere developed which dominated the tobacco market of the future – hot-air, lue-cured Bright(orVirginia)tobacco,andair-cured,yellowish-redBurleytobaccofromother plants[11,16].Thistobaccowasthenusedforchewingbecause,owingtoitscoarse plantstructure,itcouldabsorbmoresugarsandotherlavouringagentswithoutappear-ingmoist.
TheirsttobaccomanufactorywasestablishedinSeville,andin1788theirstcigar factorybasedontheSpanishmodelwasbuiltinHamburgbySchlottmann[7].Thecigars producedbySchlottmannsoldpoorly,promptinghimtotransportthemtoCuxhavenso thattheycouldthenbefetchedbackas“imports”withgreatcommercialsuccess.Napoleon broughtthecigartoFrancefromwhereitcrossedintoGermany.Thecigarbecamethe statussymbolofthesociallyambitiousmiddleclasses,andlaterbecamethehallmarkof thecapitalist(GeorgeGrosz:“TheFaceoftheRulingClass”,1921).Thetabaceriaswhich originatedinCubawerealsoinvolvedinthemanufactureofcigars,with100–300workers beingemployedinasinglefactory.
InsomeEuropeancountries,cigarwasperceivedasthesymbolofforeigninluenceand ofoppositiontendencies,forexample,inthenineteenthcenturyPrussia.TheNeuePreussische Kreuzzeitungwrotein1848:“Thecigaristhevisiblesymbolofrecklessness.Withacigarin hismouth,ayoungmansaysanddaresquitedifferentthingsthanhewouldsayanddare withoutacigar”.DuringtherevolutionaryconfrontationsinMarch1848,themiddleclasses in Berlin demanded “Freedom to smoke in the Zoological Gardens”. The cigar was the dominanttobaccoproductforvirtually100years.
1.4.2
Development of the Cigarette
6 1 History of Tobacco
moreeasily[17].In1913,ReynoldsusedBurleytobaccofortheproductionofhisCamel cigarettes[18]. This tobacco blend became the prototype for the American cigarette, whereasBritishcigaretteswerealsoproducedwithVirginiatobacco.
Comparedwiththeacridandstrong-tastingsmokeofcigars,cigarettesmokeismore pleasant,andthiscanbeattributedtothepHofthesmoke[17].WherepHisinthealkaline range,nicotineinthesmokeispresentpredominantlyinitsfreeformbutisnotfoundin thegaseousphase.Thissmokeisdificulttoinhalebecauseoftheacridtasteofnicotine. Thefactthatnicotineisneverthelessabsorbedwhenacigarissmokedisduetoitsslower passageacrossthebuccalmucosa,themembraneliningthemouth[5].
CigarettesmokingirstbecamewidespreadduringtheCrimeanWar(1853–1856):sol-diersbecameaccustomedtosmokingstrongRussiancigarettes,andtookthehabitback withthemtotheirowncountrieswhenhostilitiesended.OneSt.Petersburgcigarettefac- tory(theYenidseCompany)openeditsirstsubsidiaryinDresdenin1862.Theirstcig-arette-makingmachine,withanhourlyoutputof3,600cigarettes,wasdisplayedbythe SusiniCompanyfromHavanaattheParisWorldExhibitionin1867.Bythe1880s,US companiesfollowedsuitwiththeirowncigarette-makingmachines.Asaresult,produc-tioncostsfelldramatically,newmarketsopenedup,andyoungpeoplearoundtheageof 18becameamajorconsumermarketfortheirsttime[19].Thus,smokingtookonanew face:smokingasaleisurelypastimewasreplacedbysmokingatshortintervals,mainly asameansofcopingwithstress.Unlikethecigarorapipe,acigarettecanbesmokedin 3–5min:thesmokingbreakcanbeequatedwith“thetimeittakestosmokeacigarette”. Thecigarettecametosymbolisemoderntwentiethcenturyliving(seeTable1.1).
Becausesmokingwasalwayssubjecttocertainrestrictions,itbothrepresentedsome-thing “special” and, in the nineteenth century, was invariably associated with political freedommovements.FollowingtheoutbreakofAsianinluenzainthesummerof1831, cigarsmokinginpublicplaceswaspermittedasaprotectionagainstinfection[7],andthe righttosmokeinpublicwasonthelistofdemandsattheHambachFestivalin1832. Duringthestudentprotestsof1968,itwasevendemandedthatthebanonsmokingin lecturetheatresbeliftedandthatsmokers’cornersbesetupinschoolsoruniversities.In wartimetoo,thesoldiersofallarmieshavealwaysbeenliberallysuppliedwithcigarettes toboosttheirightingmoraleandreadinessforbattle[8].
Within about 100 years, the cigarette industry rose to become one of the foremost branchesofindustry[20](seeTable1.1).
Country Before1914 1927 1928
Germany 195 302 499
England 201 811 –
France 96 248 326
Holland – 341 –
Italy 104 372 –
Sweden 115 233 –
USA 143 798a 840a
Table 1.1Cigaretteconsumptioninvariouscountriesduringtheirstthirdofthetwentiethcentury
Per-capitastatistics(from[7])
1.5
Objections to Smoking on Health Grounds
Inthenineteenthcentury,smokingwasnotviewedfromthestandpointofenjoyment. Aftertheprohibitiononsmokingwasabolished,therespectablemiddle-classesstartedto voicetheircriticismonsmokingwhich,eventhen,wereintendedprimarilytoprotect youngpeople.Inoneofhispaintingsfrom1885/1886(Skullwithburningcigarette,see Fig.1.3),theDutchartistVincentvanGogh(himselfapipesmoker)foreshadowedthe rolethecigarettewastoplayinthecenturytocome.Eventhen,withsmokingperceived as a speciic social problem prevalent among 10–12-year-old boys[8], there were complaintsabout“wayward”youngsmokers.Parents,teachersandeducatorsweretold thattheyhad:…“aseriousdutytomakeyoungpeopleawareofthegreatdangersof prematureuseofthenarcotictobacco,anactivitythatdestroystheirphysicalandmental well-being”[8].
Inthesecondhalfofthenineteenthcentury,bothintheUSAandinEurope(including GermanyandAustria),anti-tobaccoassociationswereformedbecausenewerinsightsinto thechemicalprocessesofnatureandofhumanlifeitselfhadraisedconcernsaboutthe health-related consequences of smoking[21]. Education was required concerning the
Fig. 1.3VincentvanGogh:
8 1 History of Tobacco
dangersoftobaccouseandmisuse[22].Asaresult,smokingperceptionshaveundergone acompletetransformation–the“sophisticated”habitofthe1930sisalethaladdictionin the new millennium. What was considered an appropriate social behaviour, frequently endorsedbythemedicalprofession(cf.Fig.1.4),hasnowbeenestablishedasanantisocial behaviour.Nevertheless,thetobaccoindustryunrestrainedlyadvertiseditsproductsinthe medicaljournals(cf.Fig.1.4)andamongyoungpeoplewhowereverysoonfamiliarwith allthemajorcigarettebrands(Fig.1.5).
In 1821, the physician Posselt and the chemist Reimann described a milky distillate obtainedfromfreshanddriedtobaccoleaves[24]andin1828,theyisolatednicotineasthe principalalkaloidoftobacco[8,25].Trommsdorffalsostudiedextractsfromtobaccoplants [26],buthisresearchwasnotasfruitfulasthatofPosseltandReimann.Atthattime,this (poisonous)alkaloidfuellednumerousdebatesabouttheharmfulnessofsmoking,basedon evidencefromvariousexperimentsonanimalswithnicotinedatingbacktotheseventeenth century[8]:ConradGesnerhadobservedthatdogsvomitedwhentheywereadministereda smallquantityofpowdered,driedtobaccoleaves.TheirstBocarmepoisoningtrialbefore aBelgiancourtin1850attractedgreatinterest,particularlywhenthechemistStasdetected thealkaloidnicotineinthecorpse[8].Thiscasepromptednumerousanimalexperiments withnicotinetopermitfurtherelucidationofitseffects.Theanimalexperimentsdescribed byTiedemann,workinginconjunctionwiththeanatomistBischoffinGießen,werecon-ductedinfrogs,rabbits,anddogsafterhehadreceivednicotinebasefromDr.Merckof Darmstadt[8].Theseexperimentsdescribedthehightoxicityandrapidonsetofpoisoning followedbythedeathofanimals.InalettertoTheodorZwinger,ConradGesnerdescribed thepatternofpoisoningfollowingexcessivetobaccoconsumptioninthefollowingterms: “foliiparticulafumumhaurientemsubitoinebriat,utipsenonsemelexpertussum”[8].
Conceptssuchasacuteandchronicnicotinepoisoningwereintroduced.Symptoms describedinhumansincludedagitation,stupor,cough,acceleratedbreathing,nausea,and vomitingetc.[8].Long-termdamage(chronicglossitis,pharyngitis,tonsillitis,andcancer ofthetongue)wasalreadybeingreportedasearlyas150yearsago[8,27].
By1927,morethan50%ofthetobaccousersintheUSAwerealreadysmokingciga-rettes(97,000million,risingto106,000millioninthefollowingyear,Table1.1);even thensuchconsumptionwasassociatedwithillnessonafairlylargescale.Statisticsonthe incidenceoflungcancerwerecollectedinGreatBritainasearlyas1920.Atthattimeit wasstillunclearwhetherathird(genetic)factorwasinvolvedalongsidesmokingandlung cancer.Despiteevidencetothecontrary,thetobaccoindustrycontinuedtodisputethisfact intothe1950s[28].Thetobaccoindustrydidnotshyawayfromadvertisingitsproducts evenwhendiseasescausedbycigaretteswerereported(Fig.1.6).
1.6
Women Won Over by the Cigarette
10 1 History of Tobacco
Fig. 1.5Exampleofthe
tobaccoindustry’scovertyet obviousadvertisingtargeted atyoungpeople
Fig. 1.6Thetobacco
asprestigiousasthatofchewingtobaccoorthecigar.Cigarswerethoughtofasmaledomain. In1904,aNewYorkwomanwasarrestedforsmokingandsimultaneouslydrivinghercar[29]. AftertheFirstWorldWar,cigarettesalsobecameincreasinglypopularwithwomen.The dancerLolaMontezandthewriterGeorgeSandmaybecitedasprominentexamplesof womenwhosmoked.IntheUSA,thehabitwasobservedmainlyamongwell-to-dowomen, especiallyinNewYork.Thecigarettebrandsoftheday,suchasHerbedelaReine,were aimedmainlyatafemaleclientele.TheLondontobaccohousePhilipMorrisdevelopedacork tipforthecigarette,andadvertisedthismodiiedcigaretteforwomen.However,sincethese cigaretteswererolledbyhand,theyweretooexpensivetocapturebroadsegmentsofthe market. This situation changed again when it became customary for women also to take employmentand,astheybecameincreasinglyemancipated,tosmokeinpublic.TheUSirm AmericanTobaccoproducedLuckyStrike,whichbecamethebestsellingcigarettebrand. Usingtestimonialsfromfemalecelebrities,suchastheaviatrixAmeliaEarhart,sloganslike “Tokeepaslenderigure–reachforaLuckyinsteadofasweet”,orendorsementsfromilm stars Constance Talmadge and Jean Harlow, who appeared from 1929 onwards smoking LuckyStrikecigarettesinpublic,advertisementsforcigarettesmokingweresystematically targetedatwomen.Eveninthosedays,advertisingusedslogansextollingthevirtuesofmild smoking:“Easieronyourthroat”,“IpreferLuckies,andsodoesmydaughter”,“Foryour digestion–smokeCamel”or“Camelsneverjangleyournerves”[2,30].Initsadvertising,the Chesterieldcompanydirectedthefollowingsloganatolderwomen:“Tohelpthecountry,I thinkI’lltryone”.
Withtheseadvertisingpractices,theUScigaretteindustrysucceededinthe1930sand 1940sinstylisingthecigaretteasanintegralpartoflife.DuringtheFirstWorldWar,the USGeneralPershinghadstated:“Tobaccoisasindispensable(tothesoldiers)asthedaily ration(offood)”[31]andPresidentRooseveltlaterdeclaredthecigarettetobejustas essentialasfood.SmokingwasaconspicuouslycommonfeatureincountlessHollywood movies(e.g.HumphreyBogartandhisfemaleco-stars).MarleneDietrichandGretaGarbo werefurtherprimeexamplesforthisadvertisingcampaignwhichinluencedcountless womentobecomesmokers[32].
12 1 History of Tobacco
1.7
The Medical Use of Tobacco in the Nineteenth Century
Inthenineteenthcentury,tobaccowascultivatedformedicinalpurposesintheAlsace andthePalatinate,andwassoldintheformofextracts,powders,ointmentsandaqueous solutions[10] .BartholinfromCopenhagenusedtobaccoasanenemaandintothenine-teenth century tobacco preparations were occasionally prescribed as remedies for strychninepoisoningandtetanus(lockjaw).InthemonographbyMüller[34],tobacco anditsformulations(decoctions,ointments,tinctures,wine,vinegar,pills)wererecom-mendedfordropsyinthelowerabdomen.Fowler[34]claimedtohavecured18outof 31patientsthisway.However,thedosewasselectedinsuchawaythat,asfaraspos-sible,neithersalivationnordizzinessoccurred.Otherphysiciansintheseventeenthand eighteenth centuries also used tobacco preparations for the treatment of oedema. Nicotinepreparationswerefurtherprescribedfor“spasticdysuria”(acategorywhich includedgonorrhoea).Otherauthorsfromthisperioddescribeditsusefuladministration asaremedyforneurosesandtetanus,forstrangulatedhernias(primarilyintheformof enemas)aswellasfordisordersofthelowerabdomenassociatedwithconstipation, spasticcolitisandspasticileus(inthiscaseusingtheso-calledsmokeenemas),and manyotherconditions[34].
Aslateas1837,aninfusionoftobaccoleaveswasrecommendedasanantidotetoarse-nicpoisoning,andthiswastestedindogs.Theeffectoftobaccopreparationwasachieved byinducingvomitingseveralhoursafterarsenicpoisoning[34].Inthemid-nineteenth century, Tiedemann[8] was credited with publishing a comprehensive monograph on tobaccoanditshistoryfromtheearliestbeginnings.
1.8
Tobacco Research in the Twentieth Century
propertiesinacomprehensivemonographthatisstillavailable[22].Hewasalsooneof theirstclinicianstopublicisetheconnectionbetweensmokingandthedevelopmentof bronchialcarcinomainhisnumerouslectures,astatethathedescribedindetailinhis book.Hisdemandsattheendofthebookforstemmingtheconsumptionoftobaccoare understandableeventoday,withoneexception(cultivationoflow-nicotinetobaccovariet-ies)(Table1.2 ).BecauseoftheSecondWorldWar,Germanresearchintothecausalrela-tionshipbetweensmokingandthedevelopmentofbronchialcarcinoma[36–40]couldnot besharedwiththeinternationalscientiiccommunity,andwasalsoignoredaftertheend ofthewar.ThetextofthearticlebySchairerandSchöningerwasnotpublishedinEnglish translationuntil2001whenitappearedintheInternationalJournalofEpidemiology[41], togetherwithseveralcommentaries[42,43].
All countries, irrespective of the prevailing form of government, “encouraged and promotedineveryconceivablewaytheirpeople’spassionforsmokingsimplyforthe sakeofthenationalpurse”[7].FollowingthefailureofthebansonsmokingintheUSA inthe1920s,withKansasthelaststatetoliftsuchprohibitionin1927,theEuropean countriesneverseriouslyconsideredsimilarregulations;intheviewofthoseinpower, suchactionmighthaveanadverseifnotdisastrouseffectontheeconomicandpolitical situation. After the Second World War this attitude continued, with cigarettes being rationedon“stamps”forthemanysmokersinGermany(seeChap.14).Intheimmediate post-warperiod,theAmericansofferedaidintheformoftheMarshallPlan,butatthe sametimetheygavetheGermans97,000tonsoftobacco[44]–agiftwithimmense potentialforharm.
0
14 15 16 17 18 19 20
10 20 30 40
Frequency (%)
Age [years] Boys Girls
50 60 70
Fig. 1.7Agedistribution
forcigaretteconsumption among1,058students attendinghighereducational establishments(datafroma 1933survey)[22]
Banontobaccoconsumptionforyoungpeoplebelowtheageof18 Strongwarningsagainsttobaccoconsumptionbywomen
Cultivationofnicotine-freeorlow-nicotinetobaccofor“lesstoxicsmoking” Protectionofnon-smokers
Creationofcounsellingcentresfortobaccoaddictsinmajorcities Government-sponsoredinformationcampaign
Governmentsupportforthe“GermanLeaguetoCombattheDangersofTobacco”fundedby revenueraisedfromtobaccoduty
14 1 History of Tobacco
1.9
Concluding Remarks
•
Aswithotherluxurycommodities(opium,alcohol),tobaccohasdevelopedoverthe courseof500yearsfrombeingadrugwithreligiousandceremonialconnotationstoa product of mass consumption (in the case of opium, only the Law on Anaesthetics blocksitsillegalspread).•
Ifthetobaccoplanthadnotcontainednicotine,itwouldneverhaveattaineditsworld-widesigniicance.However,sinceitdoes,thetobaccocompaniesinasmallnumberof countriesearnanestimatedhundredsofbillionsattheexpenseofthehealthofbillions ofsmokersthroughouttheworld.•
Even200–300yearsago,attitudeofEuropeanstowardstobaccowereclearlyambiva-lent,asrelectedintheactionsofmonarchs(e.g.JamesofEngland)andstatesmen.On theonehand,economiccontrolswereusedtobantobacco,whileontheotherregula-torymechanismsweresuccessfullyexploitedtomakecapitalfromthesaleoftobacco. IntheEuropeofpastcenturies,avarietyofmethodswereselectedtoachievethese ends:importandexporttaxes,monopoliesonthemanufactureoftobaccoproducts, leasingoffactoriesbythestateortransferofrightstothese,taxationoflandsetaside fortobaccocultivation,etc.Fig. 1.8Anexamplefor
•
TheGermangovernmentanditspoliticianshaveadoptedthisambivalentattitudefrom thepastandhavedeniedprotectionfromthedangersofsmokingtothemajorityofits electorate,thenon-smokers.Theyhavealsofailedtoprotectthemajorityofsmokers fromtheincreasinglyapparentdangersofsmoking.•
Inmostcountriesintheworld,cigarettesmokingisthenumber1killer.Worldwide, more people die from the consequences of cigarette smoking than from any other disease.Despitetheseproblems,thetobaccoindustryhasbeenabletoincreaseits annualturnoverbywooingnewsmokersofbothsexes(Fig.1.8 ).Underthesecircum-stances,itisexpectedthatintheyear2025morethan2millionpeopleintheEuropean Unionalonewilldiefromtheconsequencesofcigarettesmokingifthistrendisnot haltedsoon.References
1.AkuhurstBC(1981)Tobacco.Longman,London
2.JapanTobaccoPlantBreeding&GeneticResearchLaboratory(1994)ThegenusNicotiana illustrated
3.TabernaemontanusDIT(1664)NewvollkommenKräuter-Buch.JohannKönigs,Basel 4.WilbertJ(1987)TobaccoandShamanisminSouthAmerica.YaleUniversityPress,NewHaven 5.TravellJ(1940)Theinluenceofthehydrogenionconcentrationontheabsorptionofalkaloids
fromthestomach.JPharmacolExpTher69:23–33
6.RobicsekF(1978)Thesmokinggods.TobaccoinMayaart,historyandreligion.TheUniversity ofOklahomaPress,Norman
7.CortiECC(1930)DietrockeneTrunkenheit:Ursprung,KampfundTriumphdesRauchens.Insel, Leipzig
8.TiedemannF(1854)GeschichtedesTabaksundandererähnlicherGenussmittel.H.L.Brömmer, Frankfurt
9.MonardesN(1970)JoyfulNewesOuttotheNeweFoundeWorlde.London.1577(reprint). DaCapoPress,Amsterdam
10.Laufer B (1924) Introduction of tobacco into Europe. Field Museum of Natural History, Chicago
11.BrooksJE(1952)Themightyleaf.In:LittleB(ed)Tobaccothroughthecenturies.LittleBrown, Boston
12.SandgruberR(1994)Genussmittel.IhrerealeundsymbolischeBedeutungimneuzeitlichen Europa.In:JahrbuchfürWirtschaftsgeschichte.Akademie,Berlin,pp73–88
13.Jacob.(1603)MBR.Misocapnusseudeabusutabacilususregius.London
14.PrechtK,BaumgartnerHJ(1993)Tabak.Gewohnheiten,Konsequenzen.Editiondiá,St.Gallen 15.BunburyH(1794)ASmokingClub.S.W.ForesNo.3,Piccadilly
16.Tilley NM (1948) The bright-tobacco industry, 1860–1929. University of North Carolina Press,ChapelHill
17.SladeJ(1993)Nicotinedeliverydevices.In:OrleansCT,SladeJ(eds)Nicotineaddiction: principlesandmanagement.OxfordUniversityPress,NewYork,pp3–23
18.TilleyNM(1985)TheR.J.ReynoldsTobaccoCompany.UniversityofNorthCarolinaPress, ChapelHill
19.KlugerR(1996)Ashestoashes.America’sHundred-YearCigaretteWar,thePublicHealth, andtheUnabashedTriumphofPhilipMorris.AlfredA.Knopf,NewYork
16 1 History of Tobacco
21.GoodmanJ(1993)Tobaccoinhistory.Theculturesofdependence.Routledge,London 22.LickintF(1939)TabakundOrgnaismus.In:HandbuchdergesamtenTabakkunde.Hippokrates,
Stuttgart,pp1232
23.(1938–1939)PennsylvaniaMedJ42:471
24.PosseltWH,ReimannKL(1821)BemerkungenNicotinaninundseineEigenschaften.Schweigger uMeinickeNeuesJournalfürChemieundPhysik,pp1–442
25.PosseltWH,ReimannKL(1828)ChemischeUntersuchungdesTabaksundDarstellungdes eigenthümlichen wirksamen Prinzips dieser Planze. Geigers Magazin f Pharmacie 6(23): 138–161
26.Trommsdorff JB (1829) Beiträge zur chemischen Kenntnis des Tabaks. Neues Journal der Pharmacie(Leipzig)19:129–155
27.HartwichC(1911)DiemenschlichenGenußmittel.IhreHerkunft,Verbreitung,Geschichte, Bestandteile,AnwendungundWirkung.Tauchnitz,Leipzig
28.BentleyHR(1997)ReportonvisittoUSAandCanada,17April–12May1958.TobProd LitigationRep12:383–389
29.GoodmanJ(1993)Tobaccoinhistory.Routledge,London
30.KelloggJH(1946)Tobaccoism.BattleCreek/Mich.TheGoodHealthPublishing,Michigan 31.HamiltonAE(1927)Thesmokingworld.Century,NewYork
32.BlumD(1997)AufleichtenFlügelninsLandderPhantasie.TabakundKultur–Columbusbis Davidoff.Transit,Berlin
33.HurtRD,RobertsonCR(1998)Pryingopenthedoortothetobaccoindustry’ssecretsabout nicotine:theMinnesotaTobaccoTrial.JAMA280:1173–1181
34.Müller J (1842) Der Tabak in geschichtlicher, botanischer, chemischer, medicinischer und diätetischerHinsicht.vonGebrüderDaams,Emmerich
35.RedmondDEJr(1970)Tobaccoandcancer:theirstclinicalreport,1761.NEnglJMed282: 18–23
36.Glinski von (1939) Untersuchungen über die Zunahme des primären Lungenkrebses unter BerücksichtigungderPathogenese.DtschArchklinMed185:75–88
37.MüllerFH(1939)TabakmissbrauchundLungencarcinom.ZschrKrebsforsch49(1):57–85 38.HausteinKO(2004)FritzLickint(1898–1960)–EinLebenalsAufklärerüberdieGefahren
desTabaks.Suchtmed6(3):249–255
39.SchöningerE(1944)LungenkrebsundTabakrauch.Inaugural-Dissertation,UniversitätJena, pp1–25
40.SchairerE,SchöningerE(1943)LungenkrebsundTabakverbrauch.ZschrKrebsforsch54: 261–269
41.SchairerE,SchonigerE(2001)Lungcancerandtobaccoconsumption.IntJEpidemiol30(1): 24–27
42.ErnstE(2001)Commentary:TheThirdReich–Germanphysiciansbetweenresistanceand participation.IntJEpidemiol30:37–42
43.ProctorRN(2001)Commentary:SchairerandSchoniger’sforgottentobaccoepidemiology andtheNaziquestforracialpurity.IntJEpidemiol30(1):31–34
17 K.-O.Haustein,D.Groneberg,TobaccoorHealth?
DOI:10.1007/978-3-540-87577-2_2,©SpringerVerlagBerlinHeidelberg2010
2
Thetwentiethcenturyhaswitnessedthebirthanddevelopmentofanewepidemic-tobacco dependence[1–3].Inthelast40years,duetotheriseintobaccoconsumption(Fig.2.1; Table2.1),tobaccousehasbecomeaparticularhealthhazard,asdocumentedinnumerous reports[2,3,7–13] .Ithasbecomeclearthatthenicotinedependence(nicotinebeingpro-ducedthroughthetobaccoplant),afactnowconirmedbytheWorldHealthOrganization (WHO),isresponsiblefortheadverseeffectsonhealth[14].Nicotineitselfisknowntobe apowerfulpoison–similartoprussicacid[15] .Nevertheless,mosthealth-relatedconse- quencesareattributabletothe2,500toxinsinthetobaccoplantandtosome4,000sub-stancespresentintobaccosmoke[16–18].IntheUSAandmanyEuropeanUnion(EU) countries,tobaccocausesmoredeathsthananyotherdependence-producingsubstance (Table2.2)[4,19].Thedevelopingcountrieswillbesufferingthisiftheycontinueto increasetheirtobaccoconsumption[20].
InEurope,morethan30%ofthepopulationsmokecigarettes;cigarandpipesmoking andtheuseofchewingorsnufftobaccoareofsecondaryimportance.InGermany,where morethan17millionpeoplecurrentlysmoke,309peopledieeachdayfromthedirect consequencesofsmoking,whereasroadtraficaccidentsclaima“mere”21deaths/day.If anairlinerwith309passengersonboardcrasheseverydayinGermany,therewouldbea
1925 0 1,000 2,000
Great Depression
Postwar demobilization
Korean War
Increased marketing of filter cigarettes begins
Broadcast ads end
Federal excise tax doubled
Rotating package warnings Nonsmokers begin
to demand rights Fairness
Doctrine
First surgeon general’s report Early reports
linking smoking and cancer
World War II 3,000
4,000
Cigarettes per Year
5,000
[image:30.439.54.380.429.570.2]1930 1935 1940 1945 1950 1955 1960 1965 1970 1975 1980 1985 1990
Fig. 2.1AnnualpercapitacigaretteconsumptionintheUSAduringtheperiodfrom1925to1990
18 2 Epidemiology of Tobacco Dependence
nationaloutcryandthegovernmentwouldbecompelledtotakeaction.Duringtheperiod from1925tothe1960s,tobaccoconsumptionintheUSAshoweda4.2-foldincrease, beforefallingagainto2.5timesthe1925levelbythestartofthe1990s(Fig.2.1).
In the USA, cigarette smoking is responsible for one in every ive deaths (400,000 deathsperannum,seeTable2.2),chielyasaresultofcoronaryheartdisease,lungcancer andotherrespiratorytractdiseaseswhichwouldbeavoidableinprinciplebysmokingces-sation[21].Asanexoticcommodity,therefore,thecigarettehasadvancedtobecomethe commonestcauseofdeath.TheproblemhasreachedsimilardimensionsinEurope[4].
2.1
Tobacco Consumption in the Twentieth Century
Theirsttwodecadesofthetwentiethcenturylaidthefoundationforhugegrowthinthe cigaretteindustry,withcigarettesinthe1920snotsomuchproducingdependence,butrather beinghighlytoxicfortherespiratorytract.Inthe1920sand1930s,cigaretteconsumption wasboostedparticularlywhenwomenwereincludedastargetsoftheincreasinglysuccess-fuladvertisingeffortsofthetobaccoindustry,withCamelcigarettesgainingwidespread popularity[5,22].Followingtherecognitionevenduringtheseyearsoftheadverseeffects ofcigarettesonhealth[7,9,13,23],thecigaretteindustrydevelopedtheiltercigaretteasa kindofsafety“guarantee”inthe1950sandthe“low-tar”cigaretteinthe1960s[2,5].The percentageshareofiltercigarettesincreasedfrom0.3%in1949to97%in1992[24].
Inmenbornbetween1911and1930,theprevalenceofcigarettesmokingintheUSA reachedpeaklevelsof67%inthe1940sand1950s[25],withamaximumprevalenceof
Tobaccotype 1900 1952 1991
Tobaccoingeneral(kg/person) 3.4 5.9 2.3
Cigarettes(%) 2 81 87
Snuff,chewingtobacco(%) 4 3 5
Cigars(%) 27 10 4
Pipeorhand-rolled(%) 19 1 1
Table 2.1Methodsof
tobaccoconsumption intheUSAfrom 1900to1991[5,6]
Deathdueto Deaths Percentage
Tobacco 400,000 19
Poordiet,sedentarylifestyle 300,000 14
Alcohol 100,000 5
Bacterialinfections 90,000 4
Poisoning 60,000 3
Firearms 35,000 2
Sexualdeviancy 30,000 1
Roadtraficaccidents 25,000 1
Illicitdrugs 20,000 <1
Table 2.2Avoidable
44%recordedforwomeninthe1960s.Thenumberofsmokersfellonlyinresponsetothe massive anti-smoking campaigns of the 1970s, with a greater decline among men than amongwomen[26] .SmokingprevalenceinGermanywasconirmedinthelatestMicrocen-susStudy(Fig.2.2).ThenationalYouthRiskBehaviorSurvey(YRBS)2003oftheUnited Statesindicatesthattheprevalenceofcurrentcigaretteusehasdeclinedsubstantiallysince thelate1990sandisatthelowestlevelsinceYRBSwasinitiatedin1991[28].
2.2
Cigarette Smoking in the USA Since 1965
Overtheperiodfrom1965to1993,smokersintheUSAandtheirtobacco-usebehaviour weremonitoredinasurveyofallsmokersabovetheageof18yearswithaminimumannual consumptionof100cigarettes[6].Witheffectfrom1991and1992,thesurveyincludedall thosewhosmokeddaily[29,30].Deinedintheseterms,theannualprevalenceofcigarette smokingintheUSAwas42%in1965and25%in1993[6,30].Smokingcessationwas achievedby24%in1965comparedwith50%in1993[30].Inthe30–39-year-oldcategory, 89%irsttriedsmokingbeforetheageof18and71%becameregularsmokers[21].The averageageatwhichsmokingwasirsttriedwas14.6yearsandtheageatwhichsurvey respondentsbecameregularsmokerswas17.7years[21].Incontrast,after1980,thesurvey revealedthatthetransitiontoregularsmokingdidnotoccuruntilaftertheageof20[31].
Smokingwasinitiallyamalepreserve;however,from1965to1993,smokingprevalence amongmendeclinedfrom52to28%.Smokingprevalenceamongwomenwas34%in1965, fallingto22%in1993.Overall,theprevalenceofcessationamongex-smokersin1993was 52%formenand47%forwomen[30].Nevertheless,theprevalenceofmalepipeandcigar smoking,chewingtobaccoandusingsnuffrosecontinuously[3,32].Amongadolescent smokers,therewasgenderequality.From1967onwardsinparticular,therewasanincrease inthenumberoffemalesmokersfollowingtheintroductionof“femalecigarettes”[31], whereassmokingprevalenceamongyoungwomenwithacollegeeducationdeclinedover theperiodfrom1983to1991[6].
50
% Male Smokers % Female Smokers
Frequency [%] 45 40 35 30 25 20 15 10 5 0 <15 16-20 21-25 26-30 31-35 36-40 41-45 46-50 51-55 56-60 61-65 66-70 71-75 >75
Fig. 2.2Smokingprevalence
20 2 Epidemiology of Tobacco Dependence
Differencesineducationallevelarealsoapparentamongsmokers:37%ofindividuals ineducationfor9–11yearsweresmokerscomparedwithonly14%ofthosewhowerein educationfor16years[30].Highereducationallevelswerecorrelatedwithawillingness toquitsmoking[6,33] .Willingnesstoquitsmokingalsoincreasedwithage,witheduca-tionallevelalsobeingadecisivefactorinthiscontext[21,34,35].
Smokingprevalencewashighestamongpeoplelivingbelowthepovertyline[30] ,blue-collarworkers[2,36],singleordivorcedpeople[13]andmilitarypersonnel[37,38].Tobacco usedeclinedmostrapidlyamongthemedicalprofessionals;atthebeginningofthe1990s, only3%ofdoctorsintheUSAweresmokers[35],comparedwithsome20%ofdoctorsin Germany[27].However,thereseemstobearethinkingofsmokinghabitsintheUnitedStates. TheprevalenceofcigarettesmokingamongUSadultshasdeclinedbyalmosthalfsince 1965,withpositivetrendsobservedamongpeopleinalmostallsociodemographicgroups andeffortstoreducedisparitiesrecognizedasanimportantgoalinpublichealth[39].
2.3
Smoking Habits in Germany
InGermany,inpeoplebetweentheageof21and50years,smokingprevalenceisabout 33%inwomenand44%inmen(Fig.2.2 ).Simultaneously,asdirectconsequencesofciga-rette smoking, approximately 80,000–90,000 new cases of cardiovascular disease and 30,000newcasesofbronchialcarcinomaarerecordedeveryyear.Abovetheageof35, tobacco-attributablemortalityratesinthefederalGermanstatesrangefrom5.6to13.2% forwomenandfrom24.3to29.2%formen.Thehighestmortalitystatisticsarerecorded forwomeninHamburg,BerlinandBremen[27].WithanoverallmortalityrateinGermany of17%,smokingrepresentsthecommonestavoidableandexclusivelybehaviour-related causeofdeath[40].
AccordingtotheMicrocensusStudy,arepresentativesurveyconductedin1995among the population in Germany, interesting conclusions can be drawn concerning smoking behaviourasafunctionofgrossincomeandeducationallevel(seeFig.2.3).Similarresults arealsoevidentfromthelatestMicrocensusStudy[27] withregardtothepostulatedcon-nectionbetween�
![Fig. 2.1AnnualpercapitacigaretteconsumptionintheUSAduringtheperiodfrom1925to1990(from[4])](https://thumb-ap.123doks.com/thumbv2/123dok/1068241.938059/30.439.54.380.429.570/fig-annual-capita-cigarette-consumption-usa-during-period.webp)
![Fig. 2.4Correlationsbetweensmokingbehaviourandaveragegrossmonthlyincomeformen.ResultsoftheMicrocensusStudy[42]](https://thumb-ap.123doks.com/thumbv2/123dok/1068241.938059/34.439.60.384.59.396/correlations-between-smoking-behaviour-average-monthly-results-microcensus.webp)
![Table 3.1Constituents(aselectlistfromsome4,000compounds)offresh,undilutedmainstreamtobaccosmoke,producedusingasmokingmachine(1puff/min,puffduration2s,35mlsmokevolume,i.e.10puffs/cigarette)[106]](https://thumb-ap.123doks.com/thumbv2/123dok/1068241.938059/48.439.57.390.364.566/constituents-compounds-undiluted-mainstream-produced-machine-duration-cigarette.webp)
![Table 3.7Selectlistoftobaccoconstituentsusedincigaretteproductionandtheireffectsonthesmoker[80]](https://thumb-ap.123doks.com/thumbv2/123dok/1068241.938059/59.439.52.381.88.583/table-select-tobacco-constituents-cigarette-production-effects-smoker.webp)