Step-by-step approach for
development and implementaion of
hospital anibioic policy
and
from Publishing and Sales, World Health Organizaion, Regional Oice for South-East Asia, Indraprastha Estate, Mahatma Gandhi Marg, New Delhi-110 002, India (fax: +91-11-23370197; e-mail: publicaions@ searo.who.int).
The designaions employed and the presentaion of the material in this publicaion do not imply the expression of any opinion whatsoever on the part of the World Health Organizaion concerning the legal status of any country, territory, city or area or of its authoriies, or concerning the delimitaion of its froniers or boundaries. Doted lines on maps represent approximate border lines for which there may not yet be full agreement.
The menion of speciic companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organizaion in preference to others of a similar nature that are not menioned. Errors and omissions excepted, the names of proprietary products are disinguished by iniial capital leters.
All reasonable precauions have been taken by the World Health Organizaion to verify the informaion contained in this publicaion. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretaion and use of the material lies with the reader. In no event shall the World Health Organizaion be liable for damages arising from its use.
This publicaion contains the collecive views of an internaional group of experts and does not necessarily represent the decisions or the stated policy of the World Health Organizaion.
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
ea
tmen
t guidelines
Contents
List of abbreviaions iv
Introducion
1. 1
Anibioic policy
2. 6
Surveillance of animicrobial resistance 1
3. 3
Cumulaive anibiogram 1
4. 8
Development of standard treatment guidelines 2
5. 1
Strategies for promoing raional anibioic prescribing 2
6. 6
A model standard treatment guideline 7.
for community-acquired pneumonia at the hospital level 30
Animicrobial stewardship 3
8. 5
Further reading 3
9. 9
Annexes
Contributors 4
1. 2
Technical resources 4
St
ep-b
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
List of abbreviaions
ABC Calc anibioic consumpion calculator AMR animicrobial resistance
AMT animicrobial team
ARIMA auto-regressive integrated moving average ATC anatomic therapeuic chemical
ATS American Thoracic Society
BSAC Briish Society for Animicrobial Chemotherapy CAP community-acquired pneumonia
CDC Centers for Disease Control and Prevenion (Atlanta) CLSI Clinical and Laboratory Standards Insitute
CWA community-wide anibiograms DDD deined daily dose
EPOC efecive pracice and organizaion of care EQAS External Quality Assessment Scheme
EUCAST European Commitee on Animicrobial Suscepibility Tesing HAI health-care associated infecion
ICU intensive care unit
IDSA Infecious Diseases Society of America KPC Klebsiella pneumoniae carbapenemase
MIC minimum inhibitory concentraion MRSA methicillin-resistant Staph aureus
NABH Naional Accreditaion Board for Hospitals NABL Naional Accreditaion Board for Laboratories PDD prescribed daily doses
SCA Science Compuing Associates
SHEA Society for Healthcare Epidemiology of America STG standard treatment guidelines
Animicrobial resistance
[image:6.499.73.373.452.618.2]Animicrobial resistance (AMR) has emerged as a major public health problem all over the world. Infecions caused by resistant microbes fail to respond to treatment, resuling in prolonged illness and greater risk of death. Treatment failures also lead to longer periods of infecivity, with increased numbers of infected people moving in the community. This in turn exposes the general populaion to the risk of contracing a resistant strain of microorganisms. When these become resistant to irst-line animicrobials, the prohibiive high cost of the second-line drugs may result in failure to treat these diseases in many individuals. Most alarming of all are the diseases caused by mulidrug-resistant microbes, which are virtually non-treatable and thereby create a “post-anibioic era” scenario.
St
ep-b
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
Animicrobial resistance in health-care associated
infecions (HAI)
AMR has assumed greater importance in health-care seings. The presence of compromised individuals in an environment with a variety of infecious agents which are coninuously under heavy anibioics pressure results in the emergence and spread of resistant organisms to other paients in the form of cross-infecion (Fig. 1). The size of the ageing populaion is also on the rise, leading to an increasing number of individuals living with immunocompromised states. Such people spend more and more amounts of ime in hospitals or long-term care faciliies. These paients will be at risk for morbidity and mortality associated with HAI. Further, there is an associaion between the development of resistance in Staphylococcus aureus, enterococci, and Gram-negaive
bacilli and an increase in mortality, length of hospitalization, and the cumulaive cost of health care. This atributes to inappropriate, inadequate or delayed therapy. Strategies to prevent the emergence and spread of health-care associated animicrobial-resistant organisms are essenial.
Health-care epidemiologists are still grappling with problems associated with prevening the spread of mulidrug-resistant aerobic Gram-negaive bacilli in health-care seings; implemening efecive strategies to ensure animicrobial stewardship; prevening the spread of mulidrug-resistant S. aureus (MRSA) infecion in health-care seings;
and developing efecive strategies to ensure adherence to hand hygiene standards.
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
ea
tmen
t guidelines
Availability of new animicrobial agents
The situaion on the development of new animicrobial agents is not very encouraging. Hardly any promising agents are in the pipeline for treatment of some common mulidrug-resistant nosocomial organisms commonly grouped under acronym of ESKAPE:
E
nterococcus faecium (vancomycin-resistant
enterococci-VRE).
S
taph aureus (methicillin-resistant Staphylococcus aureu s-MRSA).
K
lebsiella and Escherichia coli that are producing extended spec -trum beta-lactamases (ESBL) enzymes and carbapenemases.
A
cinetobacter baumannii. P
seudomonas aeruginosa. E
nterobacter sp.
The soluion to the current approaches to animicrobial resistance is to preserve the efeciveness of the drugs presently available by anibioic stewardship and to maximize hospital infecion-control pracices, to limit the spread of resistance.
Strategies against animicrobial-resistant
microorganisms in hospitals
Strategic objecives
To develop a system to recognize and report trends in
animicrobial resistance within the insituion.
To develop a system to rapidly detect and report resistant
microorganisms in individual patients and ensure prompt treatment.
To assure increased adherence to basic infecion control policies
and procedures.
To incorporate the detection, prevention and control of
St
ep-b
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
To develop a plan for idenifying, transferring, discharging and
readmitting patients colonized with specific antimicrobial-resistant pathogens.
To establish policy and practices for rational use of
microbials.
Strategic approaches
Opimizing the duraion of choice and dose of empiric therapy:
animicrobial stewardship.
Optimizing antimicrobial prophylaxis for operative proce
dures.
Developing and implemening an anibioic policy and standard
treatment guidelines (STG).
Monitoring and providing feedback regarding antibiotic
resistance.
Improving antimicrobial prescribing by educational and
administraive means.
To achieve these, a comprehensive approach through a hospital policy on the raional use of anibioics is essenial.
Scope of the document
This document focuses on the mechanism to develop a pracically applicable hospital anibioic policy and standard treatment guidelines (STG). In addition, the document contains information on various effective strategies for implementation of STG. It also discusses various aciviies and informaion required for the development of the anibiogram, anibioic policy and standard treatment guidelines, such as surveillance programmes, the cause and controlling strategies for AMR and HAI; performance measures of anibiogram, anibioic policy and standard treatment guidelines. A model hospital STG for community-acquired pneumonia in adults is included.
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
ea
tmen
[image:10.499.73.370.96.381.2]t guidelines
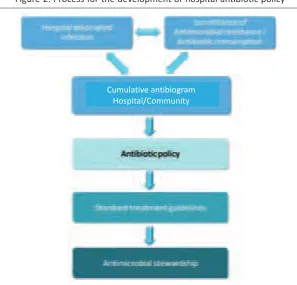
Figure 2: Process for the development of hospital anibioic policy
The document elaborates all these aciviies.
Guideline development process
The WHO Regional Oice for South-East Asia commissioned the Chrisian Medical College and Hospital, Vellore, India, to develop the irst drat of the guidelines. The objecives were to provide a tool to developing countries for establishing procedures and pracices for formulaing hospital anibioic policy and standard treatment guidelines which should lead to raional use of anibioics and minimize the emergence of animicrobial resistance. The guidelines were reviewed by several experts from Christian Medical College and Hospital, Vellore, and subsequently by Director, WHO Collaboraing Centre on Animircrobial Resistance, other experts including colleagues in the WHO Regional Oice for South-East Asia and the WHO Country Oice for India.
Guidelines development team
Anibioic policy
1,2
The primary aim of the hospital animicrobial policy is to minimize the morbidity and mortality due to animicrobial-resistant infecion; and to preserve the efeciveness of animicrobial agents in the treatment and prevenion of communicable diseases.
Scope of hospital anibioic policy
The antibiotic policy is essentially for prophylaxis, empirical and deiniive therapy. The policy shall incorporate speciic recommendaions for the treatment of different high-risk/special groups such as immunocompromised hosts; hospital-associated infections and community-associated infecions.
The hospital anibioic policy shall be based upon:
spectrum of anibioic acivity;
pharmacokineics/pharmacodynamics of these medicines;
adverse efects;
potenial to select resistance;
cost;
special needs of individual paient groups.
1 Anibioic versus animicrobial agents: An anibioic or an animicrobial is a chemical therapeuic
agent that inhibits or abolishes the growth of micro-organisms such as bacteria, fungi or protozoa. The term originally referred to an agent sourced from biological organisms; however, “anibioic” is now used commonly to refer to substances with ani-bacterial, ani-fungal or ani-parasiical acivity.
2 Policy versus guidelines: The terms policy and guidelined are used interchangeably, though they
mean diferent things. Policy should be used to refer to local, regional, or naional anibioic stewardship programmes as a whole, while guidelines should refer to speciic treatment or prophylaxis recommendaions for individual diseases, syndromes, etc.
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
ea
tmen
t guidelines
It should also set the levels for prescribing anibioics; for example, irst choice anibioics can be prescribed by all doctors while restricted choice anibioics can only be prescribed ater consuling the head of the department or the animicrobial team (AMT) representaive. Reserve anibioics, on the other hand, are prescribed only by designated experts.
Development of anibioic policy
[image:12.499.75.371.238.511.2]An overview of the key elements of the hospital anibioic policy is presented in Figure 3.
Figure 3: Key elements of hospital anibioic policy
Establish a mulidisciplinary anibioic management team to
drat policy
An eicient anibioic policy in a health-care seing shall demand from the top management their full commitment as well as their total support to the development and implementaion of this policy.
St
ep-b
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
funcions should include developing a hospital animicrobial policy, monitoring the implementation of the antibiotic policy, receiving feedback, assessing outcome and discussing with clinicians, conducing a revision of the policy every year based on the experience of prescribers and animicrobial suscepibility proiles, and seing audit targets.
The group developing the anibioic policy should be a mulidisciplinary group with 6–10 members with experise and experience in diferent subjects (usually infectious diseases, internal medicine, surgery, pediatrics, clinical microbiology, pharmacology and hospital pharmacy). At least one member should have the skills to conduct literature and systematic reviews. There should be inputs from all stakeholders, including trainees, in order to ensure “ownership” of guidelines.
The other funcions assigned to the AMT team include:
animicrobial dose and regimen alteraion;
streamlining and sequenial therapy;
disconinuaion of animicrobials;
advice on and as a result of therapeuic drug monitoring;
automaic stop orders for animicrobial prophylaxis;
restricted animicrobials;
empirical animicrobials;
approval of restricted anibioics;
assistance in interpretaion of laboratory results;
indicaion for use of speciic animicrobials;
suggesion for ordering addiional laboratory tesing and formal
educaional events.
Review available for anibioic policies and evidences
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
ea
tmen
t guidelines
broad, hence the opinion of local personnel may introduce bias into the decision-making process. However, the advantage with local guidelines is that it requires fewer resources for effective dissemination and implementaion.
The policy to be adapted for local needs with modiicaions can be chosen based on the various parameters of the animicrobial policy. This includes how informaion is gathered, cost analysis done, what was the outcome expected, the method used for analysis, how the quality and strength of evidence was assessed, how recommendaions were formulated, the strength of recommendaions and their validaion.
Drat anibioic policy based upon available evidence
The policy should be based on a systemaic review of scieniic evidence which would minimize the risk of bias. The literature should be ideniied according to an explicit search strategy and deined inclusion criteria assessed against consistent methodological standards. In addiion the search terms and period of search should be menioned.
When robust evidence is not available a hybrid of a varying degree of evidence and expert opinion may contribute to develop anibioic policy. However, this recommendaion should be done with grading according to the strength of evidence supporing them. The grading should be validated based on study design and quality and of the consistency and clinical relevance.
Atributes of anibioic policy
The policy should be simple, clear, clinically relevant, flexible and applicable to day-to-day pracice and available in user-friendly format such as a pocket guide, web-based form, etc.
The recommended anibioic should be efecive against pathogens oten seen in that locality.
Recommendaions should be provided for opimal selecion,
St
ep-b
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
Recommendation for prophylactic use should specify
procedures for which anibioic are needed, opimal agents, dosage, iming, route and duraion of administraion so that adequate anibioic concentraions are available at the ime of bacterial contaminaion. Prophylaxis recommendaion should mainly focus on clean as well as contaminated procedures. The prophylacic dose is recommended for a short duraion, free of side-efects, and should be relaively cheap. Also, the anibioics selected for prophylaxis should not be used therapeuically; as this may lead to emergence of animicrobial resistance.
Ideniicaion of gaps and research prioriies
The Policy Group should idenify evidence that is lacking and areas for further research. For example, if empiric therapy results in clinical failure, then review of cumulaive anibiogram data may be needed to change the policy accordingly. For example, an elderly male paient with cysiis seen in emergency room does not respond to empiric ciproloxacin treatment though previously the same was successful. Culture is performed and result shows E. coli resistant to ciproloxacin.
Then the research quesion would be – what percentage of urine isolates from emergency room paient are suscepible to ciproloxacin?
Monitoring and review of policy
The Policy Group should idenify sample outcome measures that would form basis for audiing both the process and outcome of the policy. For example ciproloxacin is recommended for treatment of typhoid fever, only if MIC of ciproloxacin is ≤0.25µg/ml. Audiing should include whether this recommendaion is followed? Has ciproloxacin MIC been determined for every Salmonella typhi ideniied? Furthermore, the
audit should also monitor and evaluate the quality of animicrobial prescripions for right duraion and dosage.
Policy should be reviewed by experienced peers who are not the members of the policy development group, but are experts in the relevant ield.
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
ea
tmen
t guidelines
Hospital versus naional anibioic policy
Generally, the hospital anibioic policy should concur or align with the naional anibioic policy except for a few changes as warranted by the local animicrobial resistance proiles. If there is a wide variaion from naional to hospital, and hospital to hospital then the desired purpose is defeated i.e., to minimize the morbidity and mortality due to antimicrobial-resistant infections; to preserve the effectiveness of animicrobial agents in the treatment and to prevent microbial infecions.
Important issues that may be addressed in the naional
anibioic policy
A naional anibioic policy should address all relevant issues for anibioic use, both in the community and the hospital, including veterinary and agricultural use. The important issues that need to be included in the policy are as follows:
Exising laws should be enforced to prevent non-prescripion,
over-the-counter sale of anibioics.
Guidelines for anibioic treatment and prophylaxis should be
prepared and adapted insituionally at a local level.
Consumpion of anibioics should be monitored to esimate
the naional consumpion of anibioics.
A naional animicrobial resistance surveillance system should
be established and coordinated with internaional systems. A naional control of infecions programme including a hospital
infecion control programme should be implemented. A national institute of excellence with mandate to make
recommendations on various microbiological culture and suscepibility tests and disk difusion and minimum inhibitory concentration breakpoint interpretive criteria should be established
External Quality Assessment Scheme (EQAS) to ascertain
St
ep-b
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
Educaional programmes should be elaborated for both
care workers and the public.
Collaboration with international organizations should be
established.
Appropriate funding should be made available by the
government or any other organizaion.
Limitaion of the naional animicrobial policy
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
ea
tmen
t guidelines
The anibioic policy shall depend heavily on surveillance of animicrobial resistance and antibiotic consumption in any setting. Hence, it is mandatory to establish an eicient surveillance system.
Surveillance is defined as “the ongoing, systematic collection,
analysis, and interpretaion of health data essenial to the planning,
implementation, and evaluation of public health practice, closely
integrated with the imely disseminaion of these data to those who
need to know”.
Surveillance of animicrobial resistance
Animicrobial surveillance data will help to formulate, monitor and idenify the prevailing and emerging problem, which can be contained by efecive strategy. Currently, the majority of surveillance programmes are laboratory-based. Very few clinical data are collected and the data obtained by most surveillance programmes are not useful to implement control and/or prevenion measures. One strategy to improve the collecion, collaion and disseminaion for efecive use in the hospital/ community is to integrate this function of antimicrobial resistance surveillance aciviies into the exising disease surveillance aciviies.
It is beyond the scope of this document to describe a comprehensive laboratory-based animicrobial resistance surveillance programme. This issue is addressed in other WHO documents. However, the following four features must be considered while establishing a surveillance mechanism:
Surveillance of animicrobial
resistance
St
ep-b
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
Use standards
Laboratories should use standards for reporing quanitaive resistance data (e.g. minimal inhibitory concentraions or zone diameters) that will detect decreased suscepibility. This is necessary because numerical animicrobial test results reported qualitaively (e.g., as suscepible, intermediate, or resistant) may hide an emerging resistance character in microorganisms with a small decrease in suscepibility that may sill be classiied as suscepible.
Generate reliable numerator
It is crucial to avoid including duplicate results since a paient may have either consecuive cultures obtained from the same body site or cultures from diferent body sites yielding the same organism (e.g., urine and blood culture). Therefore, only the irst posiive culture from the paient for each disease episode should be reported for surveillance purposes. This will be the reliable numerator for the animicrobial resistance surveillance.
Express resistance as incidence rate
It is important to express animicrobial resistance rates as incidence rates within a deined human populaion instead of using the number of isolates tested as denominators. This is imperaive because the submission of microbiology specimens to the laboratory is inconsistent and varies broadly. In hospital seings, it is recommended to use the number of admissions and the number of days of hospitalizaion, which are paricularly useful for inter- or intra-health-care facility comparison. It should be recognized that this process captures data only from paients admited to health facility and excludes those who atend as out door paients.
Paricipate in external quality assessment schemes
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
ea
tmen
t guidelines
The other consideraions for an efecive animicrobial resistance surveillance include:
Clinical microbiologists should be trained in health-care
epidemiology.
The choice of micro-organisms and animicrobials to survey
should be based on their relaive public health importance, using criteria such as expected numbers of cases, severity of the infecious disease as measured by its mortality rate and case-fatality raio, medical costs of such infecions, and preventability.
Microbiologists should collect not only laboratory data but also the
clinical data that is oten missing from surveillance reports.
A well-structured computer system with WHO (WHONET) open source sotware can be used for data entry and analysis (htp://www.who.int/ drugresistance/whonetsotware/en/). The analysis should be done at regular intervals and the results/observaions should be shared within the insituion, with community and collaboraive study groups.
Atributes of good surveillance systems
The atributes of a “good surveillance system” aresimplicity,
lexibility,
representaiveness,
imeliness, and
usefulness.
A surveillance system should accurately describe the occurrence of animicrobial resistance over ime and its distribuion in the populaion by place and person. This is a diicult task as the spectrum of micro-organisms under surveillance includes uneven distribuion of pathogens and opportunisic pathogens.
The surveillance system should be flexible so that changing informaion can be incorporated easily and also have room for inclusion of new diseases and health condiions. An example is the capacity of an S. aureus surveillance system to conduct special surveillance for
St
ep-b
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
The imeliness of surveillance programs should be opimal since animicrobial resistance is rapidly evolving and delay does not augur well for eicient policy. The published data usually does not relect the current state of animicrobial resistance.
Evaluaion of a surveillance system
The evaluaion of the surveillance can be measured by invesigaing the following aspects:
Does the system detect trends that signal changes in the
occurrence of diseases?
Does the system provide estimates of the magnitude of
morbidity and mortality related to the health problem under surveillance?
Does the system simulate epidemiologic research and acion
likely to lead to control and prevenion?
Does the system idenify risk factors associated with disease
occurrence?
Does the system permit assessment of the efects of control
measures?
Does the system lead to improved clinical pracice by the healthcare
providers who are the consituents of the surveillance system?
Predicion of evoluion of animicrobial resistance
To predict the short-term evoluion of resistance, the behaviour of animicrobial use, and its dynamic relaionship, ime-series analysis on anibioic resistance and consumpion data help to esimate the probability of suscepibility of the microorganism to every available anibioic. This informaion facilitates to make recommendaions about the empiric therapy, relevant to the local environment that would minimize the probability of error in the therapeuic choice.
Surveillance of animicrobial consumpion
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
ea
tmen
t guidelines
and sales. The same should be made publicly available to formulate anibioic policy and STG.
To evaluate if anibioic prescribing is raional, data on number of prescripions, indicaions, dose and duraion of treatment, as well as diferent age groups are essenial. Such data are needed in order to evaluate the impact of anibioic prescribing on resistance, morbidity, complicaions, and mortality.
However, drug consumption data with varying data collection system, ime periods, and units of measurements makes it diicult to compare trends in anibacterial usage between geographical regions. Further, in many developing countries, the lack of access to essenial pharmaceuicals, over the counter sales, and subopimal dosage are major problems in collecing reliable data.
Measurement of animicrobial consumpion
WHO Collaboraing Centre for Drug Staisics Methodology (1999) describes unit called as deined daily dose (DDD) according to the Anatomic Therapeuic Chemical (ATC) classiicaion system. This deined daily dose is a unit based on the average adult dose used for the main indicaion of the drug. To make comparisons between geographical areas possible, the number of DDDs per 1000 inhabitants and day (DID) may be calculated. This measure will be inluenced by several factors, for example, the dosage and duraion of treatment, which may vary between hospitals even for the same indicaion.
The other measure of anibioic use is the number of anibioic prescripions per 1000 inhabitants per year. This measure is probably more appropriate when evaluaing anibioic use in children.
WHO commissioned five pilot projects in different countries to ascertain community-based surveillance of antimicrobial use and resistance in resource-constrained seings. The methodology followed and observaions made can be seen in WHO document published in 2009.
Cumulaive anibiogram
The surveillance for animicrobial resistance/anibioic consumpion and preparaion of an “enhanced” or cumulaive anibiogram at the local level helps in clinical decision-making, design infecion control intervenions, and animicrobial-resistance containment strategies.
Atributes of cumulaive anibiogram
The major attributes of a reliable cumulative antibiogram (Fig. 4) include:
Analyses/presentaion of data regularly, at least annually.
Inclusion of only inal, veriied results.
Inclusion of only species with at least ≥ 30 isolates tested
(under certain circumstances, when you don’t have >30 isolates, then combine two consecuive years’ isolates into the calculaion).
Inclusion of diagnosic (not surveillance) isolates.
Informaion only on drugs rouinely
tested.
Inclusion of the irst isolate per paient in the period analyzed,
irrespecive of the body site from which the specimen was obtained or the animicrobial suscepibility patern.
Calculaion of the percentage suscepibility because clinicians
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
ea
tmen
[image:24.499.70.378.98.389.2]t guidelines
Figure 4: Overview of cumulaive anibiogram
Avoid the presentaion of potenially misleading or confusing
data, especially when presening as a table and ensure all the details are provided in the accompanying footnotes.
Providing conidence intervals and staisical signiicance of
changes in the percentage of suscepible isolates. Uilizing staisical tools to analyze the data.
Undertaking data stratification to encourage optimal
animicrobial therapy. It is oten useful to straify results by specimens type or infecion site, by nursing unit or site of care, by organism’s resistance characterisics , by clinical service or paient populaion.
Reviewing the cumulaive anibiogram data if clinical failure
occurs ater empiric therapy and, if changed, the trend has to be followed.
Ensuring the quality of the cumulaive anibiograms.
Comparing the cumulaive anibiogram with naional data.
St
ep-b
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
Anibiogram – derived radial decision trees
This type of disseminaion in the hospital helps to recognize the resistance to irst-line drugs indicate suscepibility to second-line drugs and as well understand the probability of encountering such organisms.
Challenges in cumulaive anibiogram
Variability in culture and suscepibility ordering pracices is inevitable. Usually, a signiicant number of the laboratory requests for the culture susceptibility from outpatient or inpatients are due to suspected infection with resistance organisms. Consequently, the number of requests received for suscepible infecions are less as when compared with those for resistant cases. As a result, overcall of resistance rates are always introduced into most of the cumulaive anibiograms.
Community-wide anibiograms (CWA)
Establishment of local surveillance systems improves appropriate animicrobial use and curtailing ani microbial resistance. To ensure that reliable data are presented consistent mechanism to generate, collect, and collate data at the local level is required that represents community prevalence of organisms.
Cumulaive hospital anibiograms as a quality indicator
Laboratories are oten surveyed about their tesing pracices,
but analysis of anibiograms may be a useful tool to measure whether laboratories are incorporaing changes and updates in their tesing methods.
Analysis of anibiograms may provide useful informaion when
deciding where to focus educaional eforts.
Increased compliance with standards and guidelines, paricularly
those with regard to daily veriicaion of unusual or unlikely results, should result in decreased errors on anibiograms, and thus provide more reliable data to clinicians to guide anibioic choice.
Programmes that provide and explain the antimicrobial
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
ea
tmen
t guidelines
Efecive standard treatment guidelines (STG) improve paient care while enhancing cost savings. The STG also relect data on resistance, recognizing that local patterns of resistance often differ across geographical regions. The use of the STG can be an efecive means of changing behaviour; hence the STG should be readily adaptable for local implementaion.
Prerequisites of efecive STG
The standard treatment guideline should be based on the
indings of the cumulaive anibiogram, animicrobial policy, surveillance data on animicrobial resistance and anibioic consumpion data and hospital associated infecion proile of the paricular hospital or community.
If a large number of STG documents are available from diferent
sources on the same subject, these can be compared for strengths and weaknesses in each guideline. Then a suitable guideline among the existing ones can be adapted with modiicaions for a desired local hospital, community/region. The STG should clearly specify for which disease/condiion(s)
they are sipulated, and also state who the intended users and the target populaion are, and what are the intervenions and pracices – such as evaluaion, diagnosic studies, treatment and prevenion – considered.
The guideline developers should describe methods used
to collect/select the evidence such as search of electronic databases and the number of documents sourced.
Development of standard
treatment guidelines
St
ep-b
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
All the major recommendaions should be accompanied with
levels of evidence (I–III) available and grades of recommendaion (strong, moderate and weak). The quality and strength of the evidence can be based on a raing scheme generally followed as listed below:
Level I (high):
• Evidence from well-conducted, randomized controlled trials.
Level II (moderate):
• Evidence from well-designed,
controlled trials without randomizaion (including cohort, paient series and case-control studies). Level II studies also include any large case series in which systemaic analysis of disease paterns and/or microbial aeiology was conducted, as well as reports of data on new therapies that were not collected in a randomized fashion.
Level III (low):
• Evidence from case studies and expert opinions. In some instances, therapy recommendaions come from anibioic suscepibility data without clinical observaions.
Prerequisites of STG
Should be based on local anibiograms.
Should be syndrome/diseased based.
Should specify type of clinical seing – Outpaient clinics,
Inpaient units, ICU seing.
Should specify raionale of guidelines.
Should provide evidence-based strength of
recommendaions.
Should involve treaing physicians to bring ownership to
the guidelines.
Development of STG
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
ea
tmen
t guidelines
recommendaion is a composite of the individual STG developer group members’ grades. For the inal document, a strong recommendaion require majority of the commitee members to consider it to be strong. The moderate or weak management recommendaions are usually not followed by the majority of the clinicians.
The descripion of the methods used to analyse the evidence should be stated. This could be either a review or review of published meta-analyses.
Also, evidence supporing the recommendaions, references and type of evidence supporing the recommendaions must be menioned, and a formal cost analysis should be performed and included. Likewise, if clinical algorithm(s) are useful, they could be made and included.
Recommendaions in STGs
Minor criteria and major criteria for the diagnosis are
formulated and recommended for the clinical syndrome/ disease concerned.
Recommendaions are made for pathogen-directed therapy.
Once the aeiology of the infecion has been ideniied on the basis of reliable microbiological methods, animicrobial therapy is directed at that pathogen.
Decision of admission to hospital is advised on the basis of the
severity-of-illness scores, or prognosic models. This can idenify the level of care as outpaient, in-paient non-ICU admission or direct in-paient ICU admission.
Recommendations on the empirical antimicrobial therapy
is specified separately for outpatient treatment, inpatient treatment, non-ICU treatment and in-paient ICU treatment on considering clinical condiion and presence of co-morbidiies. In addiion to the constellaion of suggesive clinical features,
St
ep-b
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
Recommendaions are generally made for a class of anibioics
rather than a speciic drug, unless outcome data clearly favours a speciic drug. Since overall eicacy remains good for many classes of agents, the more potent drugs are given preference because of their beneit in decreasing the risk of selecion for anibioic resistance. Other factors for consideraion of speciic animicrobials include pharmacokineics/pharmacodynamics, compliance, safety and cost.
Early treatment (within 48 hours of the onset of symptoms)
with appropriate animicrobials is recommended whereas for paients admited through the emergency department, the irst anibioic dose should be administered while sill in that department.
Recommendaions on the duraion of therapy for paients with
infecion should lay emphasis that therapy should coninue for a minimum of 48 to 72 hours ater the paient becomes afebrile and should have no more than one or two syndrome associated signs of clinical instability before disconinuaion of therapy.
Recommendaion on the criteria for clinical stability should be in
place. Usually this can be the minimum expected temperature; heart rate; respiratory rate; systolic blood pressure and arterial oxygen saturaion.
Recommendaion on switch from intravenous to oral therapy
can be made when the paient is haemodynamically stable and improving clinically, is fully conscious, and able to ingest oral medicaions.
Recommendaion on the use of animicrobials should take
into account the use of animicrobials within the previous three months (in which case an alternaive from a diferent class should be selected). In case the individual is from a geographical region that has a high rate (>25%) of resistant organisms reported or where high-level minimal inhibitory concentraion (MIC) is observed then, the use of alternaive agents is mandatory.
Recommendaion on paient discharge can be suggested as
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
ea
tmen
t guidelines
The locally adapted guideline should ofer suggesions about
the epidemiology and/or risk factors for alternaive or speciic addiional anibioics for the treatment.
Suggesion for the management of “non-responding infecions”
can be outlined. Non-responding infecion is deined as an inadequate clinical response despite adequate antibiotic treatment.
Monitoring the quality of animicrobial prescripions
Even with the use of STGs, one needs to monitor their applicaion. Monitoring should be done to ascertain the following:
Is the clinical picture compaible with an infecion? Is there an
indicaion for treatment with anibioics?
Is the choice of the animicrobial drug adequate?
Eicacy: Is the (suspected) agent acive? •
Toxicity/allergy: Is there a less toxic alternaive? •
Cost: Is there a less costly alternaive at equal eicacy •
and toxicity?
Broadness of spectrum: Is the spectrum unnecessarily •
broad?
Is the duraion of treatment appropriate?
Too long/too short? •
Is the dosage correct?
Dose/interval/mode of administraion •
Is the iming appropriate?
Too early/too late? •
Validaion of STG
Strategies for promoing raional
anibioic prescribing
Apart from convenional methods of communicaion, efecive strategies are found to be aimed at appropriate pracices for prescribing anibioics by changing physician behaviour such as educaion outreach (academic detailing with interacive sessions) and use of computer informaion systems and computer checks that can facilitate changes. Reminders to health-care workers have to be used sparingly; otherwise too frequent reminders will be ignored. Computer checks can be programmed into a hospital informaion system (HIS) to provide reminders, warnings and other suggesions to facilitate appropriate ordering of therapeuic and prevenive treatments. Educaional outreach is another efecive strategy. For example, in academic detailing, there is a one-on-one dialog and the exchange tends to be interacive rather than didacic. In the interacion, the provider being detailed can discuss the mater with the academic detailer unil the provider understands the issue.
Barrier-oriented intervenions
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
ea
tmen
t guidelines
Barrier Explanaion
Lack of awareness Clinician unaware that the guidelines exist.
Lack of familiarity Clinician aware of guidelines but unfamiliar with speciics.
Lack of agreement
Clinician does not agree with a speciic recommendaion made in guidelines or is averse to the concept of guidelines in general.
Lack of self-eicacy Clinician doubts whether he or she can perform the behaviour.
Lack of outcome expectancy
Clinician believes that the recommendaions will be unsuccessful.
Lack of moivaion Clinician is unable/unmoivated
to change previous pracices.
Guideline-related barriers Guidelines are not easy or convenient to use.
Paient-related barriers
Clinician may be unable to reconcile guidelines with paient preferences.
Environmental-related barriers
Clinician may not have control over some changes (e.g., ime, resources, organizaional constraints).
Adapted from Cabana et al 1999.
Using checklist as an efecive tool
St
ep-b
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
Finally, the most generally effective strategy to consider is mulifaceted intervenions. Muliple strategies are likely to be more successful than one.
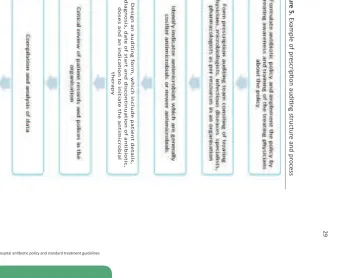
Prescripion audiing
Prescripion audiing is an indispensable and efecive tool to monitor animicrobial prescripion pracices. If properly done, it can help treaing physicians to improve their animicrobial prescripion skills and help an organisaion to adhere to, monitor and improve compliance to anibioic policy.
29
Ex
ample
of
pr
escrip
ion
audiing
structur
e
and
pr
[image:34.499.141.622.74.368.2]A model standard treatment
guideline for community- acquired
pneumonia at the hospital level
1
Purpose
This document is developed for diagnosis, management and treatment of community acquired pneumonia (CAP).
Intended use
This STG is intended to be used for adults in criical care, emergency medicine, family pracice, infecious diseases, internal medicine and pulmonary medicine. However, these guidelines should be modiied as per the need in CAP occurring in immuno-compromised paients, transplant recipients, high-dose coricosteroid recipients and human immunodeiciency virus/acquired immunodeiciency syndrome (HIV/ AIDS) paients.
The suggested reading references are considered along with the microbiology culture suscepibility data (anibiogram) for the previous ive years for developing the hospital-based STG for CAP. The quality and strength of the evidence should be followed as stated in the adult CAP guidelines.
Among the recommended anibioics (empirical or pathogen-speciic therapy) included are crystalline penicillin, macrolides, doxycycline, luoroquinolones, beta-lactam plus beta lactam and carbapenem based on the severity of illness and the causaive microorganisms oten seen in this region.
1 This STG is suggesive and health faciliies need to modify it to suit their needs, match with local
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
ea
tmen
t guidelines
Standard treatment guideline for community acquired
pneumonia
Suspect
1 if paient (not been hospitalized in the previous two weeks; not immunocompromised) has any combinaion of the following:
Symptoms: fever, cough (with or without expectoraion), (a)
pleuriic chest pain, dyspnoea).
Signs: Temp >38 °C, tachypnoea, tachycardia, impaired (b)
percussion notes, bronchial breath sounds, crackles, altered VF/VR.
Check oxygen saturaion
2 (SpO2) by pulse oximetry; start oxygen
if SpO2 <90%.
Conirm
3 with chest X-ray (to be done as soon as possible).
Severity assessment
4 based on CURB-65 score
6 point score (range 0 - 5) (a)
Gives
(b) one point each for:
(i) Confusion (abbreviated mental test score ≤ 8 or new disorientaion in person, place, or ime)
(ii) Urea >42 mg/dL
(iii) Respiratory rate ≥ 30/min Low
(iv) Blood pressure (SBP < 90 mm Hg or DBP ≤ 60 mm Hg) Age ≥
(v) 65 years
Interpretaion (c)
CURB-65 score 0 or 1: low risk of death (i)
CURB-65 score 2: moderate risk of death (ii)
CURB-65 score ≥3: high risk of death (iii)
Laboratory tests 5
Complete blood counts (a)
Urea, creainine (b)
Anibiogram (only if CURB 65 score ≥2) (c)
St ep-b y-s tep appr oach f or de velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
Sputum Gram stain & culture (opional) (e)
(i) Only if CURB 65 score ≥2 & paient can expectorate.
Specimen (expectorated sputum) should be transported (ii)
promptly to the laboratory.
Seing of care
6
CURB-65 score 0 or 1: outpaient (a)
CURB-65 score 2: inpaient (ward) (b)
CURB-65 score ≥3: inpaient (M-ICU) (c)
Anibioic management
7
All paients should receive the irst dose of anibioics as soon as the diagnosis of CAP is conirmed
CURB-65 score 0 or 1 (a)
Preferred
(i) : Amoxycillin 500 mg orally every 8 hours x 5 - 7 days
Alternaives: (ii)
Levoloxacin 750 mg orally once a day x 5 - 7days (1)
Azithromycin 500 mg orally once a day x 3 days (2)
Doxycycline 100 mg orally twice a day x 7 days CURB-65 (b)
score 2#
Preferred
(c) : Crystalline penicillin 20 L units intravenous every 4 hours x 7 days CURB-65 score ≥3#
Pref
(i) erred: Piperacillin-Tazobactam 4.5 G intravenous every 8 hours + Azithromycin 500 mg intravenous once a day x 7 – 14 days
Alte
(ii) rnaives:
Crystalline penicillin 20 L units intravenous every 4 (1)
hours + Azithromycin 500 mg intravenous once a day x 7 – 14 days
Ertapenem 1 G intravenous once a day + Azithromycin (2)
500 mg intravenous once a day x 7 – 14 days
# Change to an oral regimen as soon as clinical improvement occurs and the temperature has been
normal for 24 hours, and there is no contraindicaion to the oral route.
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
ea
tmen
t guidelines
Other recommendaions included in the hospital STG for CAP are:
If paient is criical with signs of infecion admited through the
emergency department, the irst anibioic of choice should be recommended for administraion while sill in the emergency room.
Once the aeiology of CAP has been ideniied and suscepibility
reports are available the animicrobial therapy should be either coninued or altered according to the suscepibility report. Paients with CAP should be treated for a minimum of ive
days. Paient should be afebrile for at least 48 to 72 hours, and should have no more than 1 CAP-associated sign of clinical instability before disconinuaion of therapy.
When patient is haemodynamically stable and improving
clinically (temperature <37.8 degrees C, heart rate <100 beats/ min, respiratory rate <24 breaths/min, systolic blood pressure >90 mm Hg, arterial oxygen saturaion >90% or pO2 >60 mm Hg and full conscious), able to take oral medicaions, then a switch from intravenous to oral therapy is recommended. Paients should be discharged as soon as they are clinically
stable. At discharge, paient should have no other acive medical problems, and have a safe environment for coninued care. Failure to respond to iniial therapy should raise quesions
of diagnosis, treatment adherence, and antimicrobial resistance.
Polysaccharide pneumococcal (23-valent) may be given either
at hospital discharge or during outpaient treatment.
Smoking cessaion and alcohol abstaining should be advised for
paients in whom such habits contributed to the illness. Educaing the paient regarding the hygiene measures, including
St
ep-b
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
STG performance measures to improve/track outcome
in the hospital
Antibiotics should be administered within four hours of
admission to the health-care facility.
Only the recommended anibioics should be used and not
others.
Blood cultures, if drawn, should be drawn before anibioics
are given.
The paients should receive advice or administered pneumococcal
Good antimicrobial stewardship involves selecting an appropriate drug and opimizing its dose and duraion to cure an infecion while minimizing toxicity and condiions for selecion of resistant bacterial strains.
Beneits of prescribing against non-prescribing of
anibioics
The clinical syndromes should be carefully assessed based on the beneits of prescribing against non-prescribing of anibioics as outlined below:
Paient cure/improvement against failure/mortality.
Development of resistance in pathogens infecting the
paient.
Risk for spread of resistance.
Suppression of normal lora.
Development of resistance in normal lora.
Risk for super infecion.
The other relevant issues to be considered are:
In vitro
suscepibility.
Anibioic spectrum and need for combinaion therapy.
Anibioic acivity: bactericidal / bacteriostaic.
Site of infecion and achievable anibioic concentraion.
Dosage and pharmacodynamic principles.
St
ep-b
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
Dosing and host factors like weight, immunosuppression,
hepaic/renal failure. Cost-efecive raio.
Drug interacions and poor absorpions.
Further, this can be effectively assisted by instituting various regulaions such as formula restricion, automaic stop-order, prior approval programmes, therapeutic substitution, streamlining and anibioic cycling, etc.
Maximizing clinical outcomes and minimizing selecion
of resistant organisms
What should be done
Appropriate empirical animicrobial therapy, with right dose,
for right duraion and at right ime.
Delayed therapy or modifying the initial antimicrobial •
therapy does not improve the outcome.
Mulidrug-resistance organism predisposes for inappropriate •
therapy.
Early and accurate identification of the pathogen and
suscepibility.
Combination or monotherapy chosen on the basis of the
pathogen ideniied.
Deescalaion of iniial broad spectrum therapy ater deiniive
diagnosis (generally based on microbiology reports).
What should not be done
Treat non-infecious or nonbacterial syndrome.
Treat colonizaion or contaminaion.
Treat longer than necessary.
Fail to make adjustment in a imely manner.
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
ea
tmen
t guidelines
Animicrobial stewardship, hand hygiene and STG
Hand hygiene compliance rates of 10%-40% have been observed in even the best of the units in the developed countries. Acceptability of such compliance rates and jusiicaions of intense animicrobial usage under the umbrella of “empirical therapy” has underscore the importance of increasing hand hygiene compliance eforts. In recent years, adopion by WHO of hand hygiene as the irst global challenge and the availability of robust hand hygiene compliance monitoring tools has led to an increase in hand hygiene compliance. Uniformity in monitoring hand hygiene compliance through these tools has also provided comparability and credibility to the hand hygiene compliance igures. Improved hand hygiene compliance has also led to decline in “empirical animicrobial therapy” in such units.
MRSA can be contained by acive surveillance culture, admission culture, isolaion, decolonizaion and decontaminaion. Scandinavian countries and the Netherlands efecively pracices the “admission screening” for MRSA, but nowhere outside these countries is this
implemented rouinely. Although the importance of such aciviies is well known it is yet to be appreciated fully.
Anibioic use as a cause of hospital infecion
Third-generaion cephalosporins and quinolones are implicated as a risk factor for increased MRSA / gram negaive bacilli colonizaion and infecion. There is also ample evidence that MRSA incidence rates declined following implementaion and monitoring of anibioic policies that reduced use of cephalosporins and quinolones. Similarly, reports of VRE incidence rates declined following implementaion of anibioic policies that reduced use of vancomycin and Clostridium difficile
following reduced use of clindamycin.
Studies had demonstrated the concept of ‘squeezing the balloon’
St
ep-b
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
Pifalls of pracising according to the guidelines
The anibioic stewardship achieves only “uniformity of prescribing” with
adherence to policies, guidelines and formularies. Paradoxically this may actually be at imes harmful, as the best defence against resistance is probably “diversity of prescribing”.
The other important issue is diiculty in reducing overall anibioic use, as modern medical developments seem to have no end to the immunosuppression of the paient.
American Thoracic Society. Guidelines for the iniial management (1)
of adults with community-acquired pneumonia: Diagnosis, assessment of severity, and iniial animicrobial therapy. Am J Resp Crit Care Med. 2001, 163: 1730-1754.
Cabana MD, Rand CS, Powe NR, et al. Why don’t physicians follow (2)
clinical pracice guidelines? A framework for improvement. JAMA 1999;282: 1458-1465.
Cassiere HA, Fein AM. Duraion and route of anibioic therapy in (3)
paients hospitalized with community-acquired pneumonia: Switch and step-down therapy. Semin Resp Infect. 1998, 13: 36-42. Ehrenkranz NJ, Nerenberg DE, Shultz JM, and Slater KC. Intervenion (4)
to discontinue parenteral antimicrobial therapy in patients hospitalized with pulmonary infections: Effect on shortening hospital stay. Infect. Control. Hosp. Epidemiol, 1992, 13, 21-32. European Surveillance of Antimicrobial Consumption, 2003, (5)
Results of the ESAC retrospecive data collecion (htp://www. ESAC.ua.ac.be).
Fraser GL, Stogsdill P, Dickens Jr JD, Wennberg DE, Smith RP, and (6)
Prato BS. Anibioic opimizaion. Arch. Intern. Med., 1997, 157, 1689-1694.
Gould IM. Anibioic policies and control of resistance. Curr. Opin. (7)
Infect. Dis., 2002, 15, 395-400.
Grol R and Grimshaw J. Evidence-based implementation of (8)
evidence-based medicine. Jt. Comm. J. Qual. Improv., 1995, 25, 503-521.
St
ep-b
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
Grol R and Grimshaw J. From best evidence to best pracice: (9)
efecive implementaion of change in paient care. Lancet, 2003, 362, 1225-1230.
Grimshaw JM and Russell IT. Achieving health gain through clinical (10)
guidelines. II: Ensuring guidelines change medical pracice. Qual. Health Care, 1994, 3, 45-52.
(11) Halstead DC, Gomez N and McCarter YS. Reality of Developing a Community-Wide Anibiogram. J. Clinical Microbiol, 2004, 42, 1-6.
Hindler JF, Stelling J. Analysis and presentaion of cumulaive (12)
anibiograms: A new consensus guideline from the Clinical and Laboratory Standards Insitute. Clin Infect Dis 2007; 44:867–73. Houck PM, Bratzler DW, Nsa W, et al. Timing of antibiotic (13)
administraion and outcomes for Medicare paients hospitalized with pneumonia. Arch Intern Med. 2004, 164: 637-644.
Gould IM. Controversies in infecion: infecion control or anibioic (14)
stewardship to control healthcare-acquired infecion? Journal of Hospital Infecion, 2009, 73, 386-391
Keuleyan E, Gould IM. Key issues in developing anibioic policies: (15)
from an insituional level to Europe-wide. European Study Group on Anibioic Policy (ESGAP), Subgroup III. Clin Microbiol Infect, 2001, 7(Suppl. 6), 16-21.
Mandell LA, Wunderink RG, Anzueto A, et al. Infecious Diseases (16)
Society of America; American Thoracic Society. Infecious Diseases Society of America / American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007, 44: (Suppl 2): S27-S72.
Mandell LA, Bartlett JG, Dowell SF, et al. Update of practice (17)
guidelines for the management of community-acquired pneumonia in immunocompetent adults. Clin Infect Dis. 2003, 37: 1405-1433.
Perla RJ and Belliveau PP. Anibiogram-Derived Radial Decision (18)
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
ea
tmen
t guidelines
Ramsdell J, Narsvage GL, Fink JB, et al: Management of community-(19)
acquired pneumonia in the home. Chest. 2005, 127: 1752-1763. Richet H. Beter animicrobial resistance surveillance eforts are (20)
needed. Am. Soc. Microbiol. News, 2001, 67, 1-6.
Ronning M, Salvesen Blix H, Harbo BT and Strom H. Diferent (21)
versions of the anatomical therapeuic chemical classiicaion system and the defined daily dose—are drug utilisation data comparable? Eur. Clin. Pharmacol., 2000, 56, 723-727.
Taylor GM. An audit of the implementaion of guidelines to reduce (22)
wound infecion following caesarean secion. Health Bull. (Edinb), 2000, 58, 38-44.
Thomson O’Brien MA, Oxman AD, Haynes RB, Davis DA, Freemantle (23)
N, et al. Local opinion leaders: Efects on professional pracice and health care outcomes. Cochrane Database Syst. Rev., (2), 2000, CD000125.
WHO Collaboraing Centre for Drug Staisics Methodology, 2002, (24)
St
ep-b
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
Annex 1
Contributors
Dr V. Balaji
Professor and Head of Microbiology
Chrisian Medical College and Hospitals
Vellore (Tamil Nadu), India
Dr O.C. Abraham
Professor and Head of Infecious Diseases
Chrisian Medical College and Hospitals
Vellore (Tamil Nadu), India
Dr Sujith Chandy
Professor and Head of Clinical Pharmacy
Chrisian Medical College and Hospitals
Vellore (Tamil Nadu), India
Ms Surang Dejsirilert Director
WHO Collaboraing Centre on Animicrobial Resistance Naional Health Insitute
Department of Medical Sciences Ministry of Public Health Thailand
Nonthaburi
Dr Vikas Manchanda Head of Mircobiology Chacha Nehru Bal Chikitsalya Shahdara
Delhi
Dr Sangeeta Joshi Head of Mircobiology Manipal Hospital Bangalore
Dr Anuj Sharma NPO (Laboratories) WHO Country Oice India New Delhi
Dr Rajesh Bhaia
Regional Adviser and Focal Point for Animicrobial Resistance WHO Regional Oice for South-East Asia
y-s
tep appr
oach f
or de
velopmen
t and implemen
ta
ion of hospit
al an
ibioic policy and s
tandar
d tr
ea
tmen
t guidelines
Annex 2
Technical resources
Evidence based pracice in infecion control
htp://www.nric.org.uk/integratedcrd.nsf/f0dd6212a5876e448025755 c003f5d33/7a183d3ae5edb478025702300504a1d?OpenDocument
Prudent anibioics user website htp://www.pause-online.org.uk/
Alliance for prudent use of anibioics htp://www.tuts.edu/med/apua/
Naional prescribing center htp://www.npc.co.uk/
Academy of infecion management htp://www.infecionacademy.org/
Do bugs need drugs – community educaion htp://www.dobugsneeddrugs.org/
WHONet WHO Sotware for animicrobial resistance surveillance htp://www.who.int/drugresistance/whonetsotware
Anibioic consumpion calculator
Antibiotic consumption calculator (ABC calc) is a simple
computer tool utilizing the ATC/DDD system to measure anibioic consumpion at both hospital and ward level as DDD/100 beds. ABC calc is freely available as a Microsot Excel© ile and modiied annually to incorporate any changes made to the ATC / DDD system. This can be downloaded from European study group on anibioic policies (ESGAP) page on the ESCMID. htp://www.escmid.org/research_projects/ study_groups/esgap/
ABC calc - Anibioic consumpion calculator. Version 3.1 (2006
)