28 Can Health Education Change The Behaviour About Prevention of Infection?
Luh Mira Puspita1, Eddy Supriyadi2, Fitri Haryanti3 1
Nursing Program Faculty of Medicine Universitas Udayana 2
Pediatric Hemato-Oncology Faculty of Medicine, Universitas Gadjah Mada- Sardjito Hospital Jogjakarta
3
Magister of Nursing Program Faculty of Medicine Universitas Gadjah Mada 1
[email protected], [email protected], [email protected]
Background: Infection is the major cause of death in children cancer. Implementation of infection prevention can be implemented by applying hand-washing, using antiseptic bath, oral care, visitor restrictions, application isolation, and use of barrier precautions. The problem faced is the lack of awareness and understanding of families how to prevent infection. Intervention of health education showed effectiveness to increase awareness and promote health behavior. This research aimed to analyze the effect of health education on the behavior of parents in the prevention of infection in children with cancer.
Methods: This research was the Pre Experimental with One Group Pretest-Posttest Design. The population in this study were all parents who have children with cancer are treated in a pediatric cancer ward Dr. Sardjito Hospital Yogyakarta. Sampling was performed by Consecutive Sampling with minimum sample size is 68 respondents. Analysis data using Paired Sampel t-Test for attitude and using Wilcoxon Test for knowledge and practices. The predictive value used was α=0,05 and CI= 95%.
Results: The average score on knowledge, attitude, and practices before given health education was 75.75, 82.21, and 46.26. The average score after given health education was 90.69, 86.23, and 70.09. There was an increase in the average scores before and after health education. P-value in the variable knowledge, attitude, and practide of each of the 0.000 so that there are significant differences between before and after health education.
Conclusions: Health education given for parents can change the behavior of parents about prevention of infection in children with cancer.
29 BACKGROUND
Cancer is a disease with complex manifestations depending on the type and location of the cells grow. In children, the incidence of cancer is about 1 in 600 people and be the cause of death is about 14% in children aged between 1-15 years. In the period of 2000-2009, of 1,124 children diagnosed cancer patients in Hospital Dr. Sardjito, patients diagnosed as much as 40.6% ALL, AML 13.9%, 6.7% retinoblastoma, neuroblastoma 5.5%, nephroblastoma 4.5%, and non-Hodgkin
lymphoma is about 4.4% (1). The
prevalence of leukemia that occurs in children showed the majority of children diagnosed with ALL is about 68.9% of all cases of leukemia and 23.6% are cases of AML of all cases of leukemia. As for CML occurs approximately 4.2% of cases of the total of all cases of leukemia in children (2).
Chemotherapy is one of the management for patients with cancer. Effects of chemotherapy will damage the cells that has a high proliferation activity such as bone marrow and mucosal epithelial cells that chemotherapy will cause bone marrow depression, alopecia, and mucositis (3). Treatment in patients
who are received chemotherapy to reduce the side effects of chemotherapy one of which is the occurrence of infection. Infection is the most frequent cause of death in patients leukemia (4). Prevention of infection is very important because it can reduce the risk of infection and complications of the disease that can cause death and improve quality of life (5).
Implementation of infection prevention can be implemented by applying the hand washing, using antiseptic bathing, oral care, visitor restrictions, application isolation, and the use of barrier precautions (6,7). Prevention of infection which is can be done either at home or in the hospital to wash their hands properly, the setting of food and drink with caution, as well as the child's environment settings (8).
30 monitoring conducted by the parents
against her condition provision of health education interventions showed effective results to the increased awareness of disease control and support the health seeking behavior (9). The research conducted by Sherman and Koelmeyer (2011) indicates that the provision of information by nurses about lymphedema can change the behavior of the patient in minimizing the risk of lymphedema (10).
Parents with children who suffer from leukemia requires the support of information to help make decisions. Information needs required by parents throughout the period of the child's treatment and can always be changed so that the necessary provision of continuous information (11). Health education is given regularly will help meet the needs of information needed by parents for caring for children.
This study aims to analyze the effect of health education on the behavior of the parents that knowledge, attitudes, and practices in the prevention of infections in children with cancer.
METHOD
The place of research and study design
The study was conducted in a ward childhood cancer treatment of Dr. Sardjito Hospital within the period from August to October 2014. Ward childhood cancer treatment consists of two rooms those are Wards Kartika 1 and Kartika 2 with each of bed capacity of 13 and 23 beds. The type of study is the Pre Experimental. The study design used one group pretest-posttest
design that aims to determine the
differences in the parental behavior in preventing infection in children with cancer before and after given treatment. This study was approved by the Medical and Health Research Ethics Committee (MHREC) Faculty of Medicine, Gadjah Mada University and Dr. Sardjito Hospital the number KE / FK / 849 / EC.
The population in this study were all parents who has children with cancer are treated in a pediatric cancer ward Dr. Sardjito Hospital. Sampling was performed by consecutive sampling technique that is based on the research subjects to hospital arrival. Hospital Dr Sardjito within a period of study with a minimum sample size is 68 respondents.
31 nurse who served in the room. Any parent
who has a child aged 1-12 years, diagnosed with cancer, and is being treated at Kartika Space 1 and 2 are invited to participate in the study. Parents who are work as health professionals such as doctors, nurses, or midwives are not included in the study. All parents who have been willing to participate in the study will be given an explanation of the study and performed the procedure for awarding a contract for health education.
Intervention
The provision of health education in this study using the media booklets that contain material about how to prevent infection do parents at home or in hospital. Measurement of the parents's behavior and attitude that knowledge using a questionnaire compiled in Indonesian and had previously tested the validity and reliability. The questionnaire contains 21 questions where as knowledge of the attitude questionnaire contains 18 statements. Measurement practices of parents using observation sheet that contains 9 items observable actions by nurses who served in the wards. The health education is given after the pretest questionnaire for knowledge and attitudes,
while for observation made 1 day before given health education. Observations for the posttest was performed 1 day after health education and observed for 3 days in a row. Posttest knowledge and attitudes by using a questionnaire carried out 7 days after the health education given. Respondents who had given health education booklet that can be read back.
Statistical analysis
32 the bivariate analysis, the data normality
test to determine the distribution of normal data or not. Normality test data using the Kolmogorov-Smirnov test because the sample size of more than 50 respondents. Normality test was also performed to qualify the use of parametric statistical test of Paired Samples T-Test to analyze changes in behavior before and after health education. However, the data in this study only attitude that is normally distributed variables, while for knowledge and attitude variables not normally distributed so as to test the non-parametric Wilcoxon test to analyze the behavioral changes that knowledge and practices before it is given health education (pretest) and after given health education (posttest). The predictive value used was α = 0.05 and CI = 95%. All analyzes were performed using the computer program package.
RESULTS
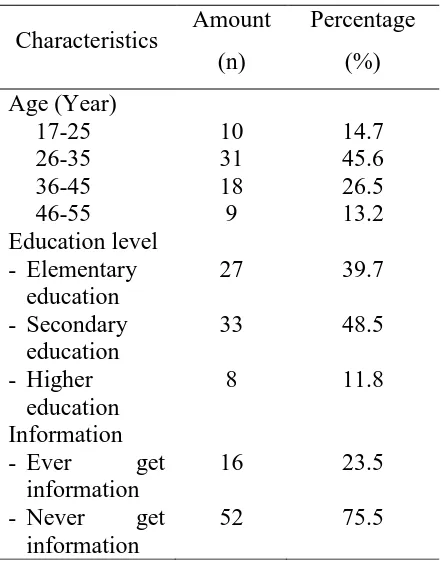
[image:6.612.327.549.110.391.2]Respondents in this study amounted to 68 people and 3 of them do not follow the posttest. Distribution characteristics of the respondents as follows:
Table 1 Characteristics of respondents (N = 68)
Characteristics Amount (n)
Percentage (%) Age (Year)
17-25 26-35 36-45 46-55
10 31 18 9
14.7 45.6 26.5 13.2 Education level
- Elementary education - Secondary
education - Higher
education
27 33 8
39.7 48.5 11.8 Information
- Ever get information - Never get
information
16 52
23.5 75.5
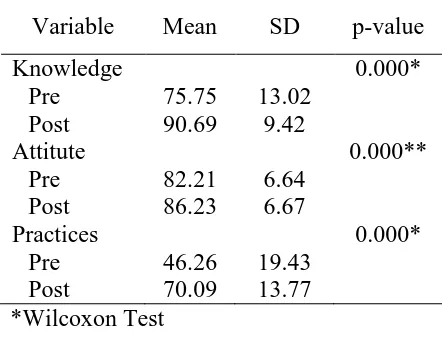
33 Table 2 Parents' behavior before and after
intervention
Variable Mean SD p-value Knowledge
Pre Post
75.75 90.69
13.02 9.42
0.000*
Attitute Pre Post
82.21 86.23
6.64 6.67
0.000**
Practices Pre Post
46.26 70.09
19.43 13.77
0.000*
*Wilcoxon Test
**Paired Samples T-Test
From Table 2 it was found that there is an increase in the average value on knowledge, attitudes, and practices of the respondents before and after health education. The analysis showed significance for knowledge, attitudes, and practices 0.000 each smaller than the value of α = 0.05 so that there are significant differences between the scores of knowledge, attitudes, and practices before and after given health education.
DISCUSSION
The provision of health education on the prevention of infection to the parents in children with cancer showed a significant difference between knowledge, attitudes, and actions of the respondents before and after health education given. The provision
of health education have been carried out in service at the hospital with a variety of health conditions. Health education can improve knowledge, attitudes, and practices of parents. Research on the provision of health education in nursing mothers showed that mothers who received health education demonstrate the knowledge, attitudes, and practices better about breastfeeding early, giving colostrum, and sustained breastfeeding. Health workers have an important role in enhancing the knowledge and motivate mothers to breastfeed (12). Brief educational intervention on asthma and healthy home showed positive changes in older people who feel they have the opportunity to realize a healthy home environment. Education is given increasing parental knowledge specifically and assist parents in changing behavior to implement changes in the family environment (13).
[image:7.612.80.301.114.287.2]34 environment. The practices is a response to
the stimulus in the form of tangible and observable (14). The results of this study showed no changes in knowledge, attitudes, and practices of parents in preventing infection. Changes in behavior that occurs as a result of the learning process. Learning is a process of change in behavior due to the interaction between individuals and individuals with the environment so as to interact and adapt to its environment (15). Parents who have given health education has increased in knowledge, attitudes, and practices so that there has been a learning process in their parents. This is consistent with the characteristics of a learning activity that results in a change in the individual, both actual and potential, and the changes are not caused by a temporary condition such as fatigue or the influence of drugs (14).
Based on Health Promotion Model theory raised by Nola J Pender stated that someone would do that behavior change is expected to bring benefits to themselves. Health promotion will increase a person's ability to perform certain actions and deeds. The influence of the external environment can also affect the desire to participate in health-promoting behaviors
(16). The provision of health education on how to prevent infection provide additional knowledge to parents so that parents tend to change behavior because they feel such action will bring benefits to themselves. Health workers who showed support infection prevention measures also affect the behavior of the parents to behave to prevent infection. Given health education increases the ability of parents to implement infection prevention. Sustainability and compliance measures are closely related to confidence in the effectiveness of actions taken. In addition, health professionals must have an agreement in action so that the actions taken by the health workers become uniform. It is important to ensure patients and families about the benefits of the actions recommended (17).
35 infection prevention application also
influence the actions of parents in preventing infection. The results show a change in behavior after the infection prevention education is given. Changes in behavior can also occur because of the support facilities provided by the hospital. Practices of parents to hand washing is good because there are adequate facilities for the realization of the action of washing hands. But to act the use of masks and special clothes visitors still lacking due to insufficient availability of such facilities. Reinforcing factors are reflected in the attitudes and actions of a role model, which in this case the nurse, and the action of the surrounding environment affects the behavior of the parents in the prevention of infection (18).
Availability and ease of access to facilities affect a person's behavior to execute an action. Health worker adherence to hand washing higher internsif care unit than non-intensive care room is connected with the ease of access using handrubs to always perform hand hygiene (19). Ease of access using handrubs contribute to the desire to perform hand hygiene (20).
The level of acceptance of the information provided is influenced by the
media used. Media used will greatly assist in the delivery of the information provided and the recipient will receive information information more clearly and precisely (14). This study uses the booklet as a medium for the provision of health education. Selection of the use of print media in this study because the print media has the advantage can be well designed, easy to read, and can reach out to all people because of a relatively low cost (21). Research on the provision of information through the booklet can increase the knowledge of children and parents of children with heart transplant recipients (22). Continuous provision of information and ease of access to information will increase knowledge (23). Information needs required by parents throughout the period of the child's treatment and can always be changed so that the necessary provision of continuous information (11).
36 information that is sustainable so that the
behavior shown may be permanent.
LIMITATIONS
This study uses only one group alone did not use a control group that did not note the difference in behavior between parents who are given and not given health education. In addition, researchers can not control the possibility of respondents interact with prospective respondents who do not get health education, to the extent possible candidates respondents had little exposure on infection prevention material of the respondents who had received health education. It would negatively affect the results of the posttest.
CONCLUSIONS
There is the effect of health education provision on parenting behaviors such as knowledge, attitudes, and actions in the prevention of infections in children with cancer. Recommendation that can be given is the health worker in hospital especially nurses is expected to provide health education on an ongoing basis by using the media as a booklet in the delivery of health education materials. The hospital is expected to provide the facility in
accordance with applicable regulations relating to the prevention of infection such as the provision of hand washing facilities dominated and availability of special clothes visitors. Research using control groups can be done to further research.
LIST OF ABBREVIATIONS
Abbreviations are used in the text : LMH (Luh Mira Puspita), ES (Eddy Supriyadi), and FH (Fitri Haryanti)
COMPETING INTERESTS
The authors declare that they have no competing interests.
AUTHORS’ CONTRIBUTION
The research was conducted by LM and supervised by ES and FH. The ethical approval was obtained by LM. Data collection done by LM. All authors read and approved the final manuscript.
ACKNOWLEDGEMENTS
The authors would like to thank for the nurses at the pediatric cancer ward Dr. Sardjito Hospital for their support in this study and also the parents who agreed to participate in this study
REFERENCES
1. Ali K, Purwanto I, Mulatsih S, Supriyadi E, Widjajanto H, Nurse J: Yogyakarta Pediatric Cancer
Registry : An International
37 Asian Pac J Cancer Prev,
2010;11:131–6.
2. Supriyadi E, Widjajanto PH, Purwanto I, Cloos J, Veerman AJP, Sutaryo S: Incidence of childhood leukemia in Yogyakarta, Indonesia, 1998-2009. Pediatr Blood Cancer, 2011 Oct;57(4):588–93.
3. Permono B, Sutaryo, Ugrasena, Windiastuti E, Abdulsalam M. Buku Ajar Hepato-Onkologi Anak. Jakarta: IDAI; 2010.
4. Chindaprasirt J, Wanitpongpun C, Limpawattana P, Thepsuthammarat K, Sripakdee W, Sookprasert A, et al: Mortality, length of stay, and cost associated with hospitalized adult cancer patients with febrile neutropenia. Asian Pac J Cancer Prev, 2013 Jan;14(2):1115–9.
5. Biswal S, Godnaik C: Incidence and management of infections in patients with acute leukemia following chemotherapy in general wards. Ecancermedicalscience, 2013 Jan 7:310.
6. Nirenberg A, Parry Bush A, Davis A, Friese CR, Wicklin Gillespie T, Rice RD: Neutropenia: state of the knowledge part I. Oncol Nurs Forum, 2006 Nov;33(6):1202–8.
7. Livadiotti S, Milano GM, Serra A, Folgori L, Jenkner A, Castagnola E, et al: A survey on hematology-oncology pediatric AIEOP centers: prophylaxis, empirical therapy and nursing prevention procedures of infectious complications. Haematologica, 2012 Jan;97(1):147– 50.
8. Hawkins J: Supportive care: managing febrile neutropenia. Paediatr Nurs, 2009 May;21(4):33–7. 9. Ramsey LS, Watkins L, Engel ME:
Health education interventions to
raise awareness of rheumatic fever: a systematic review protocol. Syst Rev, 2013 Jan; 2(1):58.
10. Sherman KA, Koelmeyer L: The role of information sources and objective risk status on lymphedema risk-minimization behaviors in women recently diagnosed with breast cancer. Oncol Nurs Forum, 2011 Jan;38(1):E27–36.
11. Kilicarslan-Toruner E, Akgun-Citak E: Information-seeking behaviours and decision-making process of parents of children with cancer. Eur J Oncol Nurs : 2013 Apr ;17(2):176– 83.
12. Hanafi MI, Hamid Shalaby SA, Falatah N, El-Ammari H: Impact of health education on knowledge of, attitude to and practice of breastfeeding among women attending primary health care
centres in Almadinah
Almunawwarah, Kingdom of Saudi Arabia: Controlled pre–post study. J Taibah Univ Med Sci, 2014 Sep;9(3):187–93.
13. Carrillo Zuniga G, Kirk S, Mier N, Garza NI, Lucio RL, Zuniga M a: The impact of asthma health education for parents of children attending head start centers. J Community Health, 2012 Dec;37(6):1296–300. 14. Notoadmodjo S: Promosi Kesehatan
dan Perilaku Kesehatan. Jakarta:
Rineka Cipta; 2012
15. Rogers A: What is the Differences? a New Critique of Adult Learning and
Teaching. Leicester: NIACE; 2003.
16. Tomey AM, Alligood MR: Nursing
Theorists and Their Work. Missouri:
Mosby Elsevier; 2006
38 preventive measures: A multicentre
survey among paediatric oncology patients. Eur J Cancer, 2008 Sep;44(13):1861–5.
18. Green LW, Kreuter MW: Health promotion planning: an educational
and ecological approach. Mountain
View, CA: Mayfield Pub. Co.; 2000 19. Almaguer-leyva M, Mendoza-flores L,
Medina-torres AG, Salinas-caballero AG, Vidaña-amaro JA, Garza-gonzalez E, et al: Hand hygiene compliance in patients under contact precautions and in the general hospital population. Am J Infect Control, 2013;41(11):976–8. 20. Sharma R, Sharma M, Koushal V:
Hand washing : a critical measure in prevention and infection control. Antimicrob Resist Infect Control, 2013;2(Suppl 1):134.
21. Campo S, Askelson NM, Routsong T, Graaf LJ, Losch M, Smith H: The Green Acres Effect : The Need for a New Colorectal Cancer Screening Campaign Tailored to Rural Audiences. Heal Educ Behav J, 2008;35(6):749–62.
22. Lawrence KS, Stilley CS, Pollock JA, Webber SA, Quivers ES: A family-centered educational program to promote independence in pediatric heart transplant recipients. Prog Transplant, 2011;21(1).