1
MODERATE SLE WITH LUPUS NEFRITIS
Blondina Marpaung, Faisal Sinurat Rheumatology Division
Departement of Internal Medicine University of North Sumatra
Medical Faculty of University of North Sumatra
PENDAHULUAN ABSTRAK
Lupus nephritis is one of the most serious manifestations of systemic lupus erythematosus (LES) and usually appear within 5 years after diagnosis. Lupus nephritis is histologically evident in most patients with SLE, even those who do not show clinical manifestations of kidney disease. Symptoms of lupus nephritis is generally associated with hypertension, proteinuria and renal failure.
Reported a case of systemic lupus erythematosus (SLE) with severe lupus nephritis in a man 23-years old boy in the hospital Haji Adam Malik attending with a swollen face since 2 weeks ago accompanied by abdominal enlargement and swelling in the extremities. Patients also complained pallor and fatigue, joint pain, sores in the mouth and gums encountered, red rash on the arms and legs encountered.
On physical examination found vital signs within normal limits, encountered anemia, weakened vesicular breath sounds in both lower courts of the lungs, additional sound not found. Ascites was found, discoid rash was found on both arms and legs, accompanied by edema in both arms and legs.
On blood examination discovered hemoglobin level 9.7 mg / d, leukocytes 1,560 /uL; platelets 50,000 /uL. Urinalysis results obtained proteinuria 2 Positive, erythrocyte sediment 2-3 / LPB, leukocytes 2-5 / LPB, urine protein 545 (+++) mg%, 24-hour urine protein 5,450 mg, urea level 71 mg / dl, creatinine 1.31 mg / dl, uric acid 8.7 mg / dL, albumin 2.1 g /dL, CRP qualitative: negative, ANA test 161 , anti ds-DNA: 409 ng / ml. On chest x-ray found bilateral pleural effusion and bronkhopenumonia. In renal ultrasound examination was found in accordance with nephrotic pattern.
Patients treated by injection of methylprednisolone puls therapy at a dose of 500 mg / day for 3 days, followed by administration of a dose of methyl prednisolone tablets from 0.5 to 0.6 mg / day with Cellcef (Mycophenolate Mofetil) 2 x 500 mg, furosemide injection, Captopril 2 x 6.25 mg. Diets high in protein (an extra egg white), and fluid balance - 500 mL. After administration of methylprednisolone pulse therapy for 3 days followed by administration of a cortico-steroid-sparing agent (MMF), proteinuria was reduced, edema is reduced and the patient's condition improves.
2 Lupus nephritis is one of the most serious manifestations of systemic lupus erythematosus
(SLE) and usually appear within 5 years after diagnosis. Lupus nephritis is histologically
evident in most patients with SLE, even those who do not show clinical manifestations of
kidney disease. Symptoms of lupus nephritis is generally associated with hypertension,
proteinuria and renal failure.
In America, the prevalence of SLE is 1 case per 2000 inhabitants in the general
population. Because of the difficulty of diagnosis and likely many cases go undetected, most
researchers suggest that the prevalence may be closer to 1 case per 500 -1,000 population.
There is stil no prevalence data of SLE in Indonesia until now. Number of patients with SLE
in Indonesia according to the Lupus Foundation of Indonesia (YLI) up to 2005 is estimated at
5,000 people. 1,2
CASE REPORT
A man - 23-year old came to Haji Adam Malik Hospital Medan on April 16th 2014
with the main complaints is a swollen face (myxo-oedema ), This is experienced since 3
weeks before admission to the hospital. Swollen face, especially in the morning and
decreases in the afternoon. accompanied by swelling in the legs. Since two weeks ago the
patients also complained of enlargement of the abdomen. The patient complained of joint
pain, especially in the shoulders, arms and knees. The pain is constantly moderate intensity,
relieved by pain-killers, but reappeared when the patients stopped taking medication. Patients
also complained reddish spots on both of his arms, hands and fingers, and became evident in
the first week. Rash on the face was not found, hair loss was not found. Complaints of pain
in the face and skin with redness if exposed to the sun was not found. History of pain in the
mouth with sores on both corners of the lips was found. Pallor experienced since 3 months
ago and more pronounced in the next 2 weeks. The history of Melena, haematochezia,
History of Haematuria, bleeding gums, epistaxis denied by the patient. Bruises history -
bruises on the skin was not be found. Pale in the face accompanied with fatigue and dizziness
was found, especially during activity. History of disease like this before was denied by the
patient, history of family members who suffer from the diseases was not found.
On physical examination found sensorium compos mentis, blood pressure of 120/60
mmHg, pols 84 x / min, frequency of breathing 22 x / min. Anaemia was found, weakened
vesicular breath sounds in both lower field of the lungs, additional sound not found. In
3 both hands and tenderness in both of knee joints was found. Discoid rash found on both arms
and legs, accompanied by edema in both arms and legs.
Routine blood examination found : hemoglobin level 9.7 mg / dL, hematocrit 28%, leukocytes 1,560 / uL, platelets 50,000 / mm3, MCV: 81 fl, MCH: 27.7 ρg, MCHC: 34.4 g%, counts (%): Neutrophils 51.3; Lymphocytes 35.3; Monocytes 12.8; Eosinophils 0; 0.6
basophils. Peripheral blood morphology suggest: Anemia normokrom + Leukopenia +
Thrombocytopenia. Hemostatic function; Bleeding Time: 3'30 "minutes, Fibrinogen 100.0
mg / dL, D-dimer was 352 ng / mL, Ferritin 1517.91 ng / mL, Iron 25μg / dL, TIBC 195 mg /
dL. Hepatitis Immunoserology test, non-reactive for HBsAg, Anti-HCV Non-Reactive, Anti
HIV (3 Methode) Non-Reactive, Anti HIV (Rapid I) Non-Reactive, Auto immune
examination of ANA test 161, Anti-ds DNA 409, Qualitative CRP <0.7 mg / dL.
Examination of Bone Marrow Puncture suggest: Myelodysplastic Syndrome (WHO
Classification: RCMD).
Urinalysis examination: protein obtained positive 2, the reduction (-), bilirubin (-),
sediment 2-3 leukocytes / LPB, erythrocyte 2-3 / LPB, Epithelium: (-); Crystal (-); Casts: (-).
The Urinary volume : 1.000 mL / 24 hours, urine protein: 545 (+++) mg%, 24-hour urine
protein: 5450 mg. Level of Ureum 71 (19-44) mg / dL, Creatinine: 1,31mg / dL, Uric Acid:
8.7 mg / dL. Liver function tests: Total Bilirubin 0.40 mg / dL, Direct Bilirubin 0.10 mg / dL,
alkaline phosphatase (ALP) 73 U / L, AST / SGOT 95 U / L, ALT / SGPT 87 U / L, Gamma
- GT 149 U / L, Total Protein 4,1g / dL, Albumin 2,1g / dL, Globulin 2.0 g / dL. Examination
of electrolytes: sodium 137 mEq / L, potassium 4.2 mEq / L, chloride 106 mEq / L, total
cholesterol 121mg / dL, triglycerides 299 mg / dL, HDL cholesterol 21 mg / dL, LDL
cholesterol 36 mg / dL, levels random blood glucose: 61.7 mg / dL. In the chest x – ray
examination found bilateral pleural effusions and Bronkhopneumonia. In renal ultrasound
examination was found in accordance with nephrotic picture pattern.
Patients diagnosed with moderate SLE with lupus nephritis + hipoalbumin. Patients
treated by injection of methylprednisolone puls therapy at a dose of 500 mg / day for 3 days,
followed by administration of a dose of methyl prednisolone tablets from 0.5 to 0.6 mg / day
with Cellcef (Mycophenolate Mofetil) 2 x 500 mg, furosemide injection, Captopril 2 x 6.25
mg. Diets high in protein (an extra egg white), and fluid balance - 500 mL. the patient's
condition improved, edema is reduced, discoid rash reduced, reduced of joints pain, and
proteinuria was reduced and planned to discharge from the hospital, with medication of
methylprednisolone 3 – 2 - 2, Cellcef (Mycophenolate Mofetil) 2 x 500 mg, Captopril 2 x
4 DISCUSSION
Renal involvement in LES is a manifestation of a common disease and is a strong
predictor of a poor outcome. The prevalence of kidney disease in 8 large cohort study
consisted of 2649 patients LES varies between 31-65%. A study analyzed the annual
incidence of lupus nephritis in 384 patients at Johns Hopkins Medical Center between 1992
to 1994, and found the incidence of acute kidney disease by 10 percent.3 Based on data from
Asia, renal involvement ranges from 6-100% overall. 3
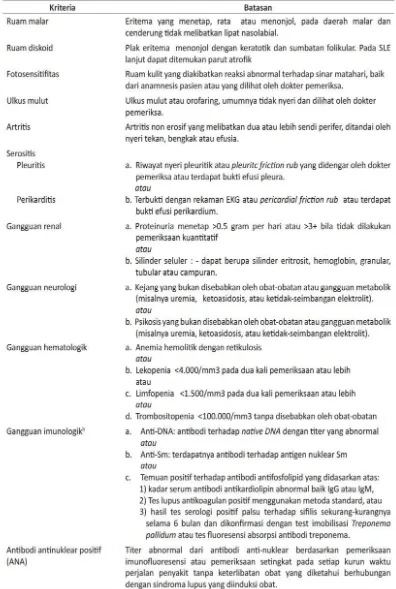
The diagnosis of SLE is made when we found more or equal to 4 criteria among the
11 criteria of the American Rheumatism Association (ARA). Hypertension in LES can occur
as a complication of renal disease or as a side effect of steroid. 3-5
In these patients the diagnosis of LES is made based on the criteria of ARA are
discoid rash, a history of joint pain on waist and knees, pleural effusion, abnormal Renal
function, proteinuria settled 5,450 mg / 24 hour, hematologic abnormalities such as anemia,
leukopenia and thrombocytopenia, immunological disorders such as anti ds-DNA positive
a nd the ANA test is increased.
Diagnosis of Lupus nephritis clinically can be enforced if found renal abnormalities
such as proteinuria with or without hematuria, hypertension, acute glomerulonephritis,
nephrotic syndrome, decreased renal function and rapid decline of renal function.
Proteinuria, or pathological urinary sediment on urinalysis examination, indicate the presence
of lupus nephritis.
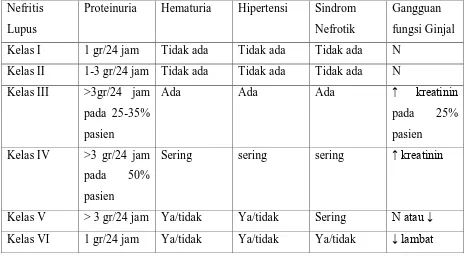
Renal biopsy is needed to reveal the anatomical pathology of the kidneys to determine
the classification of lupus nephritis to decide the treatment and the prognosis after treatment.
If the patient is not willing to be biopsied or not allowed to be biopsied because of the
physical situation, it would require an assessment of clinical symptoms are as follows:
6
In these patients found proteinuria positive 2 and 24 hours proteinuria 5,450 mg, and
mild renal impairments, so that clinically diagnosed as lupus nephritis class III / IV. Although
without a renal biopsy examination, the patient is clinically severe cases that require more
aggressive treatment. This patients renal biopsy examination was done, but the results are
inadequate biopsy sampling.
Treatment of lupus nephritis is within a class like this:
a. Class I Lupus Nefritis
Does not require any specific treatment. Treatment is directed to extra renal symptoms.
b. Class II Lupus Nefritis
If it is not accompanied by significant proteinuria and urinary sediment is not active, it
does not require specific treatment. If accompanied by Proteinuri, anti ds DNA titers were
high with hematuria , given prednisone 0.5-1 mg / kg / day for 6-12 weeks. Then slowly
reduced (titrate) the doses (5-10 weeks) every 1-3 weeks, and dose adjustment to suppress
the lupus activity.
c. Class III and IV Lupus Nefritis Induction therapy
The purpose of induction therapy is to achieve remission state of lupus activity
characterized by a resolution of the symptoms of extra renal manifestations serologic
7 creatinine concentration is reduced or at least settled. The drugs used for induction therapy
are:
a. Pulse dose glukokortikoid
For induction therapy can be administered glucocorticoid puls dose therapy, such as
methylprednisolone at dose of 500-1000 mg iv / day to induce rapid inflammatory
effects. After 3 days of administration, followed by oral prednisone at a dose of 0.5-1.0
mg / day. Prednisone can be delivered with immunosuppressant drugs to another.
b. Siklofosfamid
Given at a dose of 750 mg / m2 every month for 6 months. Supplied with prednisone at
a dose of 0.5mg / kg / day, which then lowered slowly until a dose of 0.25 milligrams /
kg / day, especially for controlling the of extras renal symptoms.
c. Mikofenolat mofetil
Mycophenolate mofetil is used for induction therapy of lupus nephritis class III and IV.
For induction therapy recommended dose of 1 g 2x a day given up to 6 months.
d. Azatioprin
Given at a dose of 2 mg / kg / day in combination with prednisone 0.5 mg / kg / day.
Prednisone dose then lowered slowly - land up to 0.25 mg / kg / day. Given for 6
month.
e. Rituximab
Used to induce remission in patients with severe lupus nephritis, who did not respond
with siklosfamid or MMF.
The basic principle of treatment is to suppress the lupus inflammatory reaction,
improve renal function, or at least maintain renal function from getting worse. With such
treatment, lupus nephritis mortality decreases.8-10 As well as hemodialysis for renal disorders
and improve existing clinical circumstances.
In these patients given induction therapy with pulse dose methylprednisolone 500 mg
iv / day for 3 days. After 3 days of administration, followed by prednisone at a dose of
0.5-1.0 mg / day. Furosemide injection, Captopril 2 x 6.25 mg. Diets high in protein (an extra egg
), and fluid balance - 500 mL. the patient's condition improved, edema is reduced, discoid
rash is reduced, joints pain decreases, and decreases proteinuria and planned discharge from
the hospital, and prescribe with methylprednisolone 3-2-2, Cellcef (Mycophenolate Mofetil)
8 CONCLUSSION
Reported a case of systemic lupus erythematosus (SLE) is with lupus nephritis +
hipoalbumin. Diagnosis based on anamnesa / history, physical examination, laboratory and
other investigations. On physical examination found vital signs within normal limits,
encountered anemia, weakened vesicular breath sounds in both lower field of the lungs,
additional sound was not found.
In abdominal examination, ascites was found, discoid rash found on both arms and legs,
accompanied by edema in both arms and legs. I Routine blood examination found : hemoglobin level
9.7 mg / dL, leukocytes 1,560 / uL; platelets 50,000 / uL. Urinalysis examination results obtained
Positive 2 proteinuria, erythrocyte sediment 2-3 / LPB, leukocytes 2-5 / LPB, urine protein 545 (+++)
mg%, 24-hour urine protein 5,450 mg, urea level 71 mg / dl, creatinine 1.31 mg / dl, uric acid 8.7 mg /
dL, albumin 2.1 g / dL, CRP qualitative: negative, ANA test 161 , anti ds-DNA: 409 ng / ml. On
chest x-ray examination found bilateal pleural effusion and bronkhopenumonia. In renal ultrasound
examination was found in accordance with nephrotic picture pattern.
Patients treated by injection of methylprednisolone puls therapy at a dose of 500 mg
/ day for 3 days, followed by administration of a dose of methyl prednisolone tablets from
0.5 to 0.6 mg / day with Cellcef (Mycophenolate Mofetil) 2 x 500 mg, furosemide injection,
Captopril 2 x 6.25 mg. Diets high in protein (an extra egg white), and fluid balance - 500 mL.
After administration of methylprednisolone pulse therapy for 3 days followed by
administration of a steroid-sparing agent kortiko (MMF), proteinuria was reduced edema is
reduced and the patient's condition improves.
REFFERENCE
1. Setiadi S, Idris A, Buku ajar ilmu penyakit dalam, edisi VI, penerbit Interna Publishing,
Jakarta, 2014 .
2. Maureen A, Hahn B, American college of rheumatology guide lines for screening,
treatment and management of lupus nephritis, Arthritis care and research, American college
of rheumatology, vol 64 p: 797-808.
3. Perhimpunan rheumatologi Indonesia, Diagnosis dan Penatalaksanaan Lupus Ertitematosus
Sitemik 2011, Interna Publishing, Jakarta, 2011.
4. Contrea G, Appel G, Mycophenolate Mofetil versus Cycloposphamide for induction lupus
9 5. Tellingen A, Voskuyl A, Dutch guidelines for diagnosis and t heraphy of proliferative
lupus nephritis, Departments of Nephrology VU university, Van Zuiden communications,
2012 p: 199-206.
6. Choi SJ, Woo JH, Induction and maintenance theraphy for lupus nephritis: a systemic
review and meta analysis. National institute of Kidney disease, 2010 p: 703-710.
7. James PA, Oparil S, Evidence based guidelines for the management of lupus nephritis in
adults. The journal of the American Medical Association, Desember 2013.
8. Ortega LM, Schultz DR. Lupus Nephritis: pathology feautures, epidemiology and a guide
to theapetic decisions, 2010;19 p: 557-574.
9. Saxena R, Mahajan T, Lupus Nephritis: current update, Biomed central, 2012.
10. Austin HA, Boumpas DT, Improved clinical outcome of lupus nephritis during the past