http://elynsgroup.com Copyright: © 2016 Swagemakers JH, et al.
Open Access Short Commentary
J Vet Res Ani Husb
Journal of Veterinary Research and Animal Husbandry
Page 1 of 2
Equine Foot MRI: Past, Present and Future
Jan-Hein Swagemakers1, Christoph Vente1 and Mahmoud Mageed2* 1Tierklinik Luesche GmbH, 49456 D-Bakum, Germany
2Dept. of Surgery and Anethesia, Faculty of Veterinary Medicine, University of Khartoum, Sudan
Since its introduction in the late 1970s, Magnetic Resonance Imaging (MRI) has become the diagnostic imaging modality of choice for the majority of musculoskeletal disorders in human medicine [1,2]. MRI is a non-invasive diagnostic tool which provides excellent soft tissue contrast and depiction of bone marrow, ligaments, tendons and cartilage without the use of ionizing radiation [3]. In veterinary medicine, MRI use was initially restricted to small animal practice due to magnet design [4]. In 1987, Park, et al. for
the first time described MRI of the equine fetlock, using cadaver
specimens. During the early 1990s MRI in the horse was limited
to cadaver studies [5,6]. MRI was first performed on live horses at
the Washington State University College of Veterinary Medicine in
1997 using a ‘high field’ MRI scanner, which is tubular in shape.
With this technology it was necessary to perform diagnostic MRI under general anesthesia [7]. In 2000, a 1.5 T MRI scanner was installed at the Animal Health Trust in New Market, UK, scanning horses as well as small animals [8]. Since the late 1990s there has
been an exponential increase in the clinical use of high field MRI in equine orthopedics. However, due to the risks of general anesthesia
(mortality rate 1%) and secondary complications are crucial considerations for the diagnostic MRI [9]. As results, this led MRI experts to adapt the open coil magnet used in human medicine in
standing, sedated horses. In 2000, Hallmarq1 developed an open coil magnet MRI scanner with U-shaped permanent magnets with field strength of 0.27 Tesla, initially installed at Bell Equine Veterinary
Clinic, UK in 2002 [8].
Since the introduction of the open coil magnet MRI scanner as
a diagnostic modality, equine orthopedics and equine practitioners have adapted quickly to this technology. It became a routine
diagnostic method as MRI provides additional insight into the anatomopathological alterations associated with lameness in comparison to other diagnostic modalities such as radiography and ultrasound. Ultrasound of the foot can provide useful diagnostic information but has not gained great acceptance [8]. In 2013, more
than 71 Hallmarq MRI scanners were installed around the world
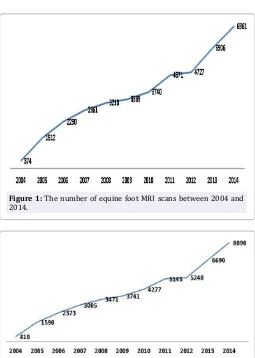
and approximately 40,000 horses examined. Comparatively, the number of horses examined during the last 15 years has increased
around 19-fold in 2014 compared to 2004 (Figure 1; www.hallmarq. net). During this period the majority of equine MRI scans (80%) were of the distal limb and foot (Figure 2; www.hallmarq.net). That is not surprising given the magnets’ design and the fact that foot pain represents the major cause of lameness in horses. The fetlock and pastern regions are more prone to motion artefact, which in
turn degrades image quality. In 2004, motion-correction software for standing equine MRI was developed. Two years later, Hallmarq released a new update (Eq2 standing scanner), which included the motion correction technique. We believe this technique advanced the use of MRI as a diagnostic tool in equine orthopedics in many ways. Firstly, the image quality of the metacarpophalangeal and proximal interphalangeal joint was significantly improved and
thus advanced the diagnostic ability. Secondly, by minimizing
motion artefacts, the need for repetition of image acquisition was avoided and thus the examination time significantly reduced.
MRI had a positive effect on our understanding of foot lameness. The high number of foot MRI resulted in further characterization
of foot pathologies/lesions and in the identification of new
conditions. For instance, lesions of the Deep Digital Flexor (DDF) tendon are now well established and recognized as one of the most important causes of foot-related lameness; which previously was
considered navicular syndrome. Deep digital flexor tendonitis is
reported in 59% of horses with foot-related lameness undergoing a MRI scan, and in 73% of horses with both DDF tendon and navicular bone lesions [10]. Moreover, the type of DDF tendon lesion can be accurately determined, which in turn allows more
accurately establish the patient’s prognosis. Accurate diagnosis has significantly improved the selection of therapeutic approaches,
which in turn has resulted in a reduction of neurectomy surgeries. Recently it has been reported that horses with core or linear lesions of the DDF tendon should not be subjected to palmar or plantar
Received Date: June 13, 2016, Accepted Date: July 28, 2016, Published Date: August 08, 2016.
*Corresponding author: Dr. Mahmoud Mageed, El-Kareb street, PO Box 32, 13314 Khartoum north, Sudan. E-mail: [email protected]
Figure 1: The number of equine foot MRI scans between 2004 and 2014.
Figure 2: Total of equine MRI scans include foot and other region. The foot MRI represent approximately 80% of the total scans in 2014
Citation:Swagemakers JH, Vente C, Mageed M (2016) Equine Foot MRI: Past, Present and Future. J Vet Res Ani Husb 1(1): 104.
Page 2 of 2 Vol. 1. Issue. 1. 34000104 J Vet Res Ani Husb
digital neurectomy as they experience residual lameness or early recurrence of lameness after surgery [11]. Magnetic resonance imaging can be used to identify horses with such DDF tendon lesions [11]. Many other lesions have been differentially diagnosed using MRI, including bone marrow injury “edema-like lesion or bone bruise” caused by repeated stressful overloading, which lead
to changes in the trabecular bone combined with fluid accumulation
due to osteoclasts activity. Treatment based on reducing the osteoclasts activity using bisphosphonates such as “clodronate disodium- Ospho2”, which is considered the drug of choice for the
treatment of edema-like injury in navicular bone have since been developed. Alongside MRI can be used as monitoring tool to assess the healing process and assist in the decision to tailor the training program, which could result in a reduction of injury recurrence.
The introduction of MRI as a therapeutic tool was tested in human medicine after patients with joint pain reported amelioration
after frequent MRI examinations [12]. It was concluded that the
MRI procedure was causing this positive effect [12]. Over several years a therapeutic MRI system was developed, which uses the same physical principle as the MRI units but with much weaker
magnetic fields and radio frequencies compared to original MRI technology. The therapy equipment from MBST3, which is one of the most popular therapeutic MRI equipment in human and equine orthopedics, uses field strengths from 0.4 to 2.35 mT for 17 to 100 kHz in the magnetic resonance frequency [12].
A clinical trial treating human osteoarthitis patients with MRI therapy appears promising [12]. General improvement ranged from 60-80%, with pain scores reduced to approximately 50% of the
initial score. Following one MBST cycle of five or nine days the pain intensity and frequency in the different condidtions significantly
decreased. Peak improvement was observed eight weeks to six months after therapy and was reported to last up to one year [12].
To the authors’ knowledge MBST has yet to be studied in horses.
In conclusion, MRI permits the diagnosis of a variety of lesions involving different structures within the foot that cannot be diagnosed using other means, thus enhancing our knowledge of the causes of foot pain. Moreover, MRI is used often for lameness originated upper limb such as carpus and tarsus.
Manufactures addresses
1. Hallmarq Veterinary Imaging Ltd, Surrey, United Kingdom.
2. Dechra Veterinary Products Ltd, Shrewsbury, United Kingdom.
3. MedTec Medizintechnik GmbH, Wetzlar, Germany.
References
1. Rothschild PA, Crooks LE, Margulis AR. Direction of MR imaging. Invest Radiol. 1990;25(3):275-81.
2. Peterfy CG, Linares R, Steinbach LS. Recent advances in magnetic resonance imaging of the musculoskeletal system. Radiol Clin North Am. 1994;32(2):291-311.
3. Reicher MA, Rauschning W, Gold RH, Bassett LW, Lufkin RB, Glen W Jr. High-resolution magnetic resonance imaging of the knee joint: normal anatomy. AJR Am J Roentgenol. 1985;145(5):895-902.
4. van Bree H, Degryse H, Van Ryssen B, Ramon F, Desmidt M. Pathologic correlations with magnetic resonance images of osteochondrosis lesions in canine shoulders. J Am Vet Med Assoc. 1993;202(7):1099-105.
5. Crass JR, Genovese RL, Render JA, Bellon EM. Magnetic resonance,
ultrasound and histopathologic correlation of acute and healing equine
tendon injuries. Vet Radiol Ultrasound. 1992;33(4):206-16.
6. Denoix J.M, Crevier N, Roger B, Lebas J.F. Magnetic resonance imaging of
the equine foot. Vet. Radiol. Ultrasound. 1993; 34(6): 405-11.
7. RK. Schneider, PR. Gavin, RL. Tucker. What MRI is teaching us about
navicular disease. American Association of Equine Practitioners. 2003.
8. Bladon B. Magnetic resonance imaging and foot lameness. Problem
solved? Or do we know we know less now that we know more? Equine
Vet J. 2014;46(3):264-66.
9. Johnston GM, Taylor PM, Holmes MA, Wood JL. Confidential enquiry of
perioperative equine fatalities (CEPEF-1): preliminary results. Equine
Vet J. 1995;27(3):193-200.
10. Dyson SJ, Murray R, Schramme MC. Lameness associated with foot pain: results of magnetic resonance imaging in 199 horses (January
2001-December 2003) and response to treatment. Equine Vet J.
2005;37(2):113-21.
11. Gutierrez-Nibeyro SD, Werpy NM, White NA, Mitchell MA, Edwards RB, Mitchell RD, et al. Outcome of palmar/plantar digital neurectomy in horses with foot pain evaluated with magnetic resonance imaging:
50 cases (2005–2011). Equine Vet J. 2015;47(2):160-4. doi: 10.1111/
evj.12262.
12. Krpan D. MBST-Nuclear magnetic resonance therapy the new possibility of osteoarthritis and osteoporosis treatment. Balneoclimatologia. 2011;35(3):61-66.
Elyns Publishing Group
Explore and Expand*Corresponding author: Dr. Mahmoud Mageed, El-Kareb street, PO Box 32, 13314 Khartoum north, Sudan. E-mail: [email protected]
Received Date: June 13, 2016, Accepted Date: July 28, 2016, Published Date: August 08, 2016.
Copyright: © 2016 Swagemakers JH, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.