PAPER • OPEN ACCESS
Higher plasma CD4 lymphocyte count correlates
with better cognitive function in human
immunodeficiency virus-acquired
immunodeficiency syndrome (HIV-AIDS) patients
To cite this article: F I Fitri et al 2018 IOP Conf. Ser.: Earth Environ. Sci.125 012030
View the article online for updates and enhancements.
Related content
Infrared Imaging: Nerve entrapment and skin temperature of the human hand
F Ring, A Jung and J uber
-Opportunistic infection manifestation of HIV-AIDS patients in Airlangga university hospital Surabaya
T P Asmarawati, A Putranti, B E Rachman et al.
-Correlation between hypertension and cognitive function in elderly
F I Fitri and A S Rambe
Higher plasma CD4 lymphocyte count correlates with better
cognitive function in human immunodeficiency virus-acquired
immunodeficiency syndrome (HIV-AIDS) patients
F I Fitri1,2, A S Rambe1 and A Fitri1
1
Department of Neurology, Faculty of Medicine Universitas Sumatera Utara, Jalan Bunga Lau No 17 ,Kemenangan Tani, Medan Tuntungan, Kota Medan, Sumatera Utara-20136, Indonesia
2
Corresponding author: [email protected]
Abstract. Neurocognitive disorders in HIV-AIDS are still prevalent despite the use of antiretroviral therapy and seem to be under-recognized. Plasma lymphocyte CD4 count is a marker for general immunology status, but its association with cognitive function remains unclear. The aim of this study was to determine the correlation between plasma CD4 lymphocyte and cognitive function in HIV-AIDS patients.This was a cross-sectional study involving 48 HIV-AIDS patients. All subjects underwent physical, neurologic examination and Montreal Cognitive Assessment-Indonesian Version (MoCA-INA) to assess cognitive function and measurement of lymphocyte CD4 counts.This study included 48 subjects consisted of 29 males (60.4%) and 19 females (39.6%). The mean age was 39.17±11.21 years old. There was a significant correlation between CD4 lymphocyte counts and MoCA-INA score (r=0.347, p=0.016).Higher plasma CD4 lymphocyte count is correlated with better cognitive function in HIV-AIDS patients.
1. Introduction
Human immunodeficiency virus (HIV) infection is an epidemic worldwide. According to estimation from the 2008 UNAIDS report on the global Acquired Immunodeficiency Syndrome (AIDS) epidemic, there were approximately 35.3 million people living with HIV worldwide.[1] In Asia the number of people living with HIV was around 5 million, with the highest and the fastest growing HIV infection levels concentrating in Southeast Asia.[1-2] There were 15,534 of people with HIV infection and 1700 AIDS cases at the end of 2014 in Indonesia, with a cumulative number from April 1987 to 2014 was 142,950 HIV cases, 55,623 AIDS cases and 9,760 mortality cases, and these numbers are predicted to continue to rise. The cumulative number of HIV-AIDS cases in Sumatera Utara province ranked tenth in Indonesia, with 8,794 HIV cases and 1,573 AIDS cases at the end of 2014, with a prevalence of 12.12 per 100,000 population.[3]
2
(MND) are still prevalent and continue to be under recognized in patients on antiretroviral therapy and remain a challenge in the treatment of HIV-AIDS patients.[5-7] Marked immune compromise, as evidenced by low CD4 lymphocyte counts, is now less frequently found among individuals with access to HAART but the milder forms of cognitive impairment are still prevalent and the association between the lymphocyte CD4 count and cognitive function remains unclear.[8-11]
The Montreal Cognitive Assessment (MoCA) has been widely used in the cognitive assessment. The MoCA assess several cognitive domains including executive function, visuospatial function, attention and concentration, memory, language, calculation and orientation.[12] The Indonesian version of MoCA, namely MoCA-INA has been developed and validated in Indonesia, and so it can be used as a cognitive tool.[13] The aim of this study was to determine the correlation between plasma CD4 lymphocyte count and cognitive function in HIV-AIDS patients.
2. Methods
This was a cross-sectional study involving 48HIV-AIDS patients in Adam Malik General Hospital Medan North Sumatera Indonesia, between June and September 2017. Inclusion criteria were: age equal or more than 18 years-old, compos mentis and fully cooperative, speak Bahasa Indonesia fluently, able to read and write, and willing to give written consent to be included in the study. Patients who were medically unstable or have other psychiatric disorders had an aphasia, history of stroke, dementia or other neurologic disorders were excluded from the study. All subjects underwent physical and neurologic examination, Montreal Cognitive Assessment-Indonesian Version (MoCA-INA) and CD4 lymphocyte measurement. All statistical procedures were performed with SPSS. The correlation between MoCA-INA Scores and CD4 count was measured using the Pearson correlation.The study was performed with approval obtained from the Health Research Ethical Committee Medical Faculty of Universitas Sumatera Utara/H. Adam Malik General Hospital.
3. Results
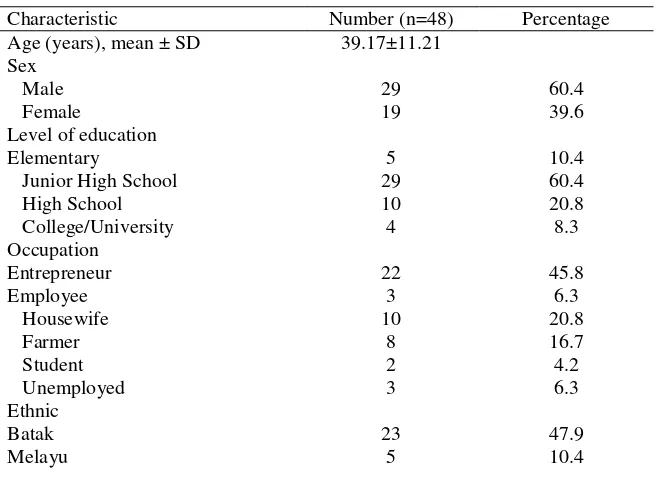
This study included 48 subjects consisted of 29 males (60.4%) and 19 females (39.6%). The mean age was 39.17± 11.21, ranging from 19 to 65 years old. The mean MoCA INA score was 23.83± 3.39, ranging from 15 to 28. The mean CD4 counts were 392.21±333.45, ranging from 5 to 1234 cells/L. Table 1 shows characteristics of subjects.
Table 1. Characteristics of subjects.
Characteristic Number (n=48) Percentage
Javanese Tionghoa Karo
7 6 7
14.6 12.5 14.6 MoCA-INA
≥ 26 < 26
17 31
35.4 64.6
MoCA-INA score, mean ± SD 23.83±3.39
CD4 counts, mean ± SD 392.21±333.45
There was no significant difference on MoCA-INA score based on the level of education. (table 2). There was also no significant correlation between age and MoCA-INA score (r=0.040, p=0.785).
Table 2. Comparison of MoCA-INA Scores based on the level of education.
Level of education Mean SD p
Elementary school 23.20 4.65 0.250
Junior high school 23.24 3.59
High school 25.70 2.16
College 24.25 0.96
There was a significant correlation between CD4 lymphocyte counts and MoCA-INA score (r=0.347, p=0.016, [95%CI 0.069-0.625]). Figure 1 shows the MoCA-INA Score plotted against CD4 lymphocyte counts.
Figure 1. MoCA-INA score plotted against CD4 lymphocyte counts.
4. Discussion
Our data show that higher CD4 lymphocyte count was correlated with better cognitive function in HIV-AIDS patients as measured by MoCA-INA score. This finding is consistent with several previous studies. A study by Childs et al (1999) found that levels of plasma CD4 count and HIV RNA were
4
predictive of HIV-associated dementia.[11] Valcour et al (2006) found that after adjusting for age and duration of HIV, CD4 nadir was related to a current diagnosis of HAD odds ratio 1.395 (1.106-1.761) Patients with CD4 lymphocyte below 200 cells/mm3 were considered highly vulnerable to neurological complications associated with infection, including cognitive impairment and the risk increased with further reductions in CD4lymphocyte count.[9]This study also found that the correlation between lymphocyte CD4 count and cognitive function was independent from age and level of education. This finding could partially reflect the effect of marked immunodeficiency in HIV patients to cognitive function. HAD generally develops in parallel with immunodeficiency and with more advanced stages of HIV.[11]
HIV-1 infects leukocytes in the periphery by way of engagement of the CD4 molecule coupled with the chemokine coreceptor CXCR4 or CCR5.[6] The infected leukocytes subsequently cross the BBB at an early stage of the infection and can persist without symptoms in the CNS for decades. [4]In the central nervous system, HIV infects infiltrating macrophages, microglia and can replicate within these cells.[4,6] Astrocytes and oligodendrocytes can be infected with HIV, but there is no viral replication. This process results in cell injury and death involving neurons, astrocytes, and neural stem cells. [6] HIV exerts its neurovirulence through two separate but linked processes. The first is a host-derived cascade of inflammatory molecules released by activated or infected macrophages, microglia, and astrocytes. The second process involves the direct neurotoxic effects of HIV-encoded proteins such as gp120, Vpr, and Tat.[6] The neuronal damage that occurs is likely caused by shed viral proteins such as gp120 and Tat or indirectly through the elevated production of neurotoxic molecules released by activated astrocytes macrophages and microglia.[5] Although neurons are not directly activation, related to the release of cytokines (TNF-), and dysfunction of various cellular channels (ie calcium, NMDA). Since neurons are not directly infected by HIV-1, the secondary mechanisms are thought to be responsible for the deterioration seen in HAD.[4] HIV infection in the brain has widespread and variable effects but appears to preferentially cause damage to the basal ganglia and deep white matter. However, damage to cortical and subcortical neurons (hippocampus and putamen), particularly dendritic pathology also are likely to play a role in CNS disease manifestations.[5]
HIV infection results in disruption of neuronal function by a variety of mechanisms that can be grouped into three general categories: viral factors, host factors and co-factors.In the nervous system, these factors converge in producing damage to the elaborate network of connections between neurons that take place at dendrites and synapses. This synapse to dendritic injury disrupts the highly integrated functioning of neural systems that is required to process information, leading to HIV-associated neurocognitive disorders (HAND), which consist of asymptomatic neurocognitive impairment (ANI), HIV-associated mild neurocognitive disorder (MND), and HIV-associated dementia (HAD). ANI describes individuals with usually mild impairment in two or more cognitive areas, demonstrated by neuropsychological testing, without a clear effect on everyday functioning. MNDrefers to the presence of mild to moderate deficits in two or more cognitive areas which create at least mild interference in everyday functioning. Finally, HAD describes individuals with documented moderate to severe deficits in two or more cognitive areas, with substantial impairment in everyday functioning making the person incapable of employment and often unable to live independently.[2,5]
executive functions, the speed of information processing, attention/working memory, motor speed, new learning and retrieval of new information, while long-term (semantic) memory, many language skills, and visuospatial abilities may remain intact. The pattern of neurocognitive dysfunction, however, is not consistent across individuals and maybe even less consistent across individuals from markedly different backgrounds.[5] HAD is characterized by impairment in a short-term memory coupled with reduced ability in mental concentration. [4] The course of dementia in HIV is highly variable from patient to patient and can present as an abrupt decline over a few weeks or a protracted course over several months. MND is often an antecedent syndrome that can precede the onset of frank dementia but presents with the clinical hallmarks HAD albeit with less-severe signs and symptoms and at higher CD4þ T-cell levels. Symptoms of HAD typically begin once an individual’s lymphocyte CD4 count drops below 200 cells/mL. Clinical risk factors for HAD include low CD4 T-cell levels, high viral load in cerebrospinal fluid (CSF) or plasma, anemia, extremes of age, injection drug use, and several host genetic polymorphisms.[6] This study did not analyze the factors that could associate with CD4 counts. A study by Li et al. found several important modifiable risk factors were associated with lower CD4 counts, including older age (>50 years), lower CD4 counts at the time of HAART initiation, the number of switches in HAART regimen in the first 5 years and hepatitis B and C virus infection.[14]
Neuropsychological assessments are the most important tools for diagnosing and categorizing HIV effects on the CNS. [5] Neuropsychologic assessment is a useful tool in confirming the diagnosis of HAD and in evaluating the response to therapy. Some of the major goals of neuropsychological evaluations in HIV-infected populations include: (1) Finding neurocognitive impairment directly attributable to HIV; (2) Determining if neurocognitive impairment is associated with co-morbid factors such as psychiatric illness, nutritional deficiencies, or co-infections; (3) Exploring relationships between neurocognitive impairment and HIV disease variables such as history of immunodeficiency (current and nadir CD4 count), viral load, biomarkers of HIV neuropathogenesis, neuroimaging, and brain pathology; (4) Determining implications for treatment including adherence and use of CNS penetrating antiretroviral regimens.[5]
The conclusion of this study is that higher plasma CD4 lymphocyte count is correlated with better cognitive function in HIV-AIDS patients. This finding could reflect that immune status as marked partly by CD4 count might contribute to the development of CNS complications, including cognitive dysfunction. Our study has several limitations. First, the design of this study was cross-sectional, so we can’t establish a causal relationship between lymphocyte CD4 count and cognitive impairment in HIV-AIDS patients. Second, this study did not measure viral load, which could be a better marker to reflect the disease progression and its effect on CNS and cognitive function.
References
[1] UNAIDS 2013 Joint united nations programme on HIV/AIDS: report on the global AIDS epidemic (Geneva, Switzerland: Joint United Nations Programme on HIV/AIDS) Available from: http://data.unaids.org/pub/Report/2013/JC1700_Epi_Update_2013_en.pdf
[2] Ellis R J, Calero P and Stockin M D 2009 HIV infection and the central nervous system: a primer Neuropsychol. Rev. 19 144-51
[3] Departemen Kesehatan RI 2014 Statistik kasus HIV/AIDS di Indonesia sampai dengan 30 Juni 2014 (Jakarta: Direktorat Jendral Pengendalian Penyakit dan Penyehatan Lingkungan Kemenkes RI)
[4] Gonzales-Duarte A, Cikurel K and Simpson D M 2006 Selected neurologic complication of HIV and antiretroviral therapy PRN Notebook 11(2) 24-9
[5] Robertson K, Liner J and Heaton R 2009 Neuropsycological assessment of HIV-infected populations in international settings Neuropsychol. Rev. 19 232-49
6
[7] Cysique L A, Bain M P, A Lane T and Brew B J 2012 Management issues in HIV-associated neurocognitive disorders Neurobehavior. HIV Med. 4 63–73
[8] Reger M A, Martin D J, Cole S L and Strauss G 2005 The relationship between plasma viral load and neuropsychological functioning in HIV-1 infection Arch. Clin. Neuropsychol. 137-43
[9] Valcour V, Yee P, Williams A E, Shiramizu B, Watters M, Selnes O, Paul R, Shikuma C and Sacktor N 2006 Lowest ever CD4 lymphocyte count (CD4 nadir) as a predictor of current cognitive and neurological status in HIV- 1 infection—The Hawaii aging with HIV cohort J. Neurovirol. 12(5) 387-91
[10] Ellisa R J, Badieea J, Vaida F, Letendra S, Heatona R K, Clifford D, Collierc A C, Gelmand B, McArthure J, Morgellof S, McCutchana J A and Granta I 2011 CD4 nadir is a predictor of HIV neurocognitive impairment in the era of combination antiretroviral therapy AIDS 25 1747–51
[11] Childs E A, Lyles R H, Selnes O A, Chen B, Miller E N, Cohen B A, Becker J T, Mellors J and McArthur J C 1999 Plasma viral load and CD4 lymphocytes predict HIV-associated dementia and sensory neuropathy Neurol. 52 607–13
[12] Nasreddine Z S, Phillips N A, Bédirian V, Charbonneau S, Whitehead V, Collin I, et al. 2005 The montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment J. Am. Geriatr. Soc. 53(4) 695-9
[13] Husein N, Lumempouw S, Ramli Y and Herqutanto 2010 Uji validitas dan reliabilitas montreal cognitive assessment versi Indonesia (MoCA-Ina) untuk skrining gangguan fungsi kognitif
Neurona 27(4) 15-22