Paediatrica Indonesiana
VOLUME 48 July NUMBER 4
Original Article
The value of urinalysis in presumptive diagnosis of
urinary tract infection in children
Dedi Rachmadi, Andaningrum Setyastuti
Abstract
BackgroundDefinite diagnosis of urinary tract infection (UTI) should only be established based on culture of urine specimen, otherwise it would be considered presumptive. Since urinalysis provides more rapid information than urine culture, clinicians should consider to utilize urinalysis as a decision-making tool for initiating treatment of UTI.
ObjectiveTo determine the sensitivity, specificity, predictive val-ues, and accuracy of several urinalysis parameters, namely the ni-trite, leukocyte esterase (LE), Gram staining, and methylene blue reductase (MBR) tests, in supporting the diagnosis of UTI.
Methods7KLVGLDJQRVWLFWHVWZDVGRQHRQVXEMHFWVZLWKS\XULD
GXULQJWKHSHULRGRI$SULOWR-XQH7KHVHQVLWLYLW\VSHFLILF -ity, positive predictive value (PPV), negative predicitve value (NPV) as well as the accuracy were calculated for each urinalysis parameter with urine culture as the gold standard. The relation-ship between categorical variables was analyzed by Fisher’s exact test or chi square test.
ResultsThe sensitivity, specificity, PPV, NPV and accuracy for nitrite test, leukocyte esterase (LE) test, Gram staining, and MBR
WHVWZHUHUHVSHFWLYHO\DVIROORZVQLWULWHWHVWVKRZHG DQG/(WHVW\LHOGHG DQG*UDPVWDLQLQJDQG DQG0%5WHVWDQG
ConclusionsThe MBR, among other urinalysis routine tests, has the highest specificity and accuracy as well as high sensitivity in establishing a presumptive diagnosis of UTI[Paediatr Indones 2008;48:199-203].
Keywords: presumptive diagnosis, urinalysis, UTI
)URP WKH 'HSDUWPHQW RI &KLOG +HDOWK 0HGLFDO 6FKRRO 3DGMDGMDUDQ
University, Dr. Hasan Sadikin Hospital, Bandung, Indonesia.
Request reprint to: Dedi Rachmadi, MD, Department of Child Health,
0HGLFDO6FKRRO3DGMDGMDUDQ8QLYHUVLW\'U+DVDQ6DGLNLQ+RVSLWDO-O 3DVWHXU 1R %DQGXQJ ,QGRQHVLD 7HO )D[
T
he term urinary tract infection (UTI) denotes infection within the urinary tract and encompasses both renal parenchyma and urinary bladder infection. This infection is important in childhood because of its symptoms that may be either troublesome or overlooked and the potential risk of renal involvement. Early recognition and appropriate treatment of such patients are essential in order to preserve renal function and prevent permanent damage.3The symptoms of children with UTI depend on the level of the infection as well as the age of the child. In classical acute pyelonephritis, patients have high fever and other systemic symptoms accompanied by back or flank pain and renal tenderness. However, symptoms of lower urinary tract such as dysuria, frequent voiding and incontinence are usually not detected in infants but it might be identified in pre-school and pre-school-age children.
is relatively expensive and requires several days to find out the results. Urinalysis might be very helpful in providing immediate information to support the diagnosis of a UTI, hence prompt initiation of treat-ment is possible. Several urinalysis parameters for making a presumptive diagnosis of UTI are leukocyte esterase (LE), nitrite, Gram staining and methylene blue reductase (MBR) tests. To our knowledge no
VXFKVWXG\KDVEHHQSXEOLVKHGKHQFHWKHSXUSRVH
of the study was to obtain the sensitivity, specificity, positive predictive values, ,and accuracy of the nitrite, LE, Gram staining and MBR tests in the diagnosis of UTI in children.
Methods
A cross-sectional study on all children with pyuria who were admitted to Pediatric Outpatient Department and Pediatric Emergency Department of Hasan Sadikin Hospital was performed during the period April to
-XQH3DUHQWDOLQIRUPHGFRQVHQWZDVREWDLQHG
and parents were interviewed regarding the history of illness and symptoms. Gender, age, physical findings, and laboratory results were recorded. The specimens for urinalysis were obtained by clean-catch mid stream
XULQHPHWKRGH[FHSWIRUFKLOGUHQXQGHUPRQWKVRI
age whose samples were taken by suprapubic aspiration. All urine specimens were collected in sterile containers without urine preservatives, transported immediately to the laboratory, and processed for urinalysis and culture.
Quantitative cultures were performed by the microbiology laboratory with pour plate method. A positive urine culture was defined as growth of
D VLQJOH SDWKRJHQ DW D FRQFHQWUDWLRQ RI ! &)8PO /DERUDWRU\ SHUVRQQHOV SHUIRUPHG GLVSWLFN
nitrite and LE test (Ames Multistix reagent strip read
ZLWKD&OLQLWHNDQDO\]HU0LOHV/DERUDWRULHV,QF
Elkhart, Ind) on unspun urine. The results of LE and
QLWULWHWHVWVZHUHUHDGDIWHUPLQXWHVDQGVHFRQGV
respectively, and reported as positive or negative. Smears were prepared using centrifuged urine that were air dried, and Gram stained. It was considered positive when bacteria were seen on any of the ten oil-immersed microscopic fields. MBRT test was done
E\ DGGLQJ PO RI PHWK\OHQH EOXH VROXWLRQ WR
ml of urine and watching for the discoloration. This
test was considered positive if discoloration occurred within 6 hours.
Sensitivity, specificity, positive and negative predictive values, and the accuracy were calculated for each test with a positive urine culture as the gold standard. Relationship between categorical variables were analyzed by Fisher’s exact test or the chi square test.
Results
8ULQH VSHFLPHQV ZHUH FROOHFWHG IURP FKLOGUHQ FRQVLVWLQJRIER\VDQGJLUOV7KHPHDQDJHRI WKHSDWLHQWVZDVPRQWKV6'PRQWKVWKH \RXQJHVWZDVILYHPRQWKVROGDQGWKHROGHVWZDV
months old. Age and sex distribution of the subjects is shown in Table 1.
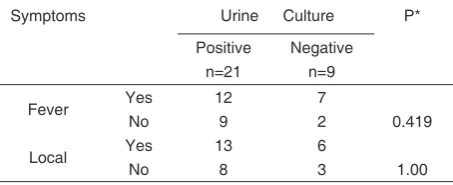
)HYHUZDVIRXQGLQRXWRIFKLOGUHQZLWK PHDQGXUDWLRQRIGD\V6'GD\VUDQJH
days). Local symptoms of UTI, i.e., dysuria, frequency,
XUJHQF\RUHQXUHVLVZHUHIRXQGLQVXEMHFWVZLWK WKHPHDQGXUDWLRQRIGD\V6'GD\VUDQJH GD\V Table 2 shows that neither fever nor local symptoms of UTI had statistically significant
associa-WLRQZLWKSRVLWLYHXULQHFXOWXUH3!5HVXOWVRI
urine culture showed that Escherichia coli was the
FRPPRQHVWSDWKRJHQIROORZHGE\.OHEVLHOOD 0LFURFRFFXVDQG3VHXGRPRQDV
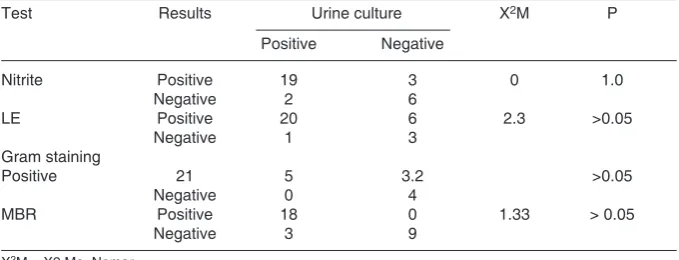
Thirty urine specimens were tested for nitrite and LE dipsticks t, Gram staining, and MBR. The
Table 1#IGCPFUGZFKUVTKDWVKQPQHVJGUVWF[UWDLGEVU
#IGITQWR $Q[ Girl 6QVCN
OQPVJU
ŌOQPVJU
OQPVJU
6QVCN
Table 2%QTTGNCVKQPDGVYGGPU[ORVQOUQH76+CPFWTKPGEWNVWTG
5[ORVQOU 7TKPG %WNVWTG 2
association of of each test and urine culture is shown in Table 3. Sensitivity, specificity, predictive values and accuracy of each test were calculated using urine culture as the gold standard as shown in Table 4.
Discussion
Our study showed that boys were more affected by UTI than girls in infancy, whereas girls were the predominant proportion in older children. This result was similar with the study of Winberg et al5 which
stated that with increasing age, there was a progressive increase in the incidence among females compare to males.5,6 The reasons were that male infants are
more sensitive to infection due to immaturity of the immunologic defense mechanisms7 and higher ratio
of urinary tract obstructive malformations.8 The
increasing incidence of UTI in girls compared to boys has been attributed to the shorter length of the female urethra providing easy access to the bladder. Aside from that, older girls have high susceptibility for periurethral colonization with Gram negative bacteria.9
Table 2 shows that neither fever nor local symp-toms of UTI had statistically significant association with positive urine culture. Positive urine culture
ZDVIRXQGLQRIVXEMHFWV7KLVZDVKLJKHUWKDQ
that reported by LohrIRXQGSRVLWLYHFXOWXUHVRI
WKHVXEMHFWVDQG:HLQEHUJDQG*DQ
ZKRIRXQGIURPVXEMHFWV7KHGLIIHU
-ent results were caused by the differ-ent designs of the studies. In our study, urine samples were taken from subjects with pyuria, whereas those studies involved subjects with symptoms suggestive for UTI. Specimens for urinalysis in our study were obtained by midstream urine method and suprapubic aspiration for children
XQGHUPRQWKVZKLOH/RKU Winberg and Gan
studies used various collection methods except with urine bag.
In this study, we found no statistically significant associations between either nitrite, LE, Gram staining, or MBR tests and the results of urine culture. The calculated sensitivity, specificity, and PPV of fever in
GLDJQRVLQJ87,ZHUHDQGUH
-VSHFWLYHO\ZKLOHWKRVHRIORFDOV\PSWRPVZHUH DQG UHVSHFWLYHO\ /RFDO V\PSWRPV KDG
better diagnostic value than fever in diagnosing UTI. All of those values were lower than those reported by
Table 45GPUKVKXKV[URGEKſEKV[RTGFKEVKXGXCNWGUCPFCEEWTCE[QHPKVTKVGVGUV.'VGUV)TCOUVCKPKPICPF/$4YKVJWTKPGEWNVWTGCU
XCNKFCVKPIUVCPFCTF
6GUV 5GPUKVKXKV[%+ 5RGEKſEKV[%+ 2TGFKEVKXGXCNWG%+ #EEWTCE[
2QUKVKXG 0GICVKXG
0KVTKVG
.'
)TCOUVCKPKPI
/$4
%+EQPſFGPEGKPVGTXCN
Table 3#UUQEKCVKQPDGVYGGPPKVTKVG.')TCOUVCKPKPIQT/$46CPFWTKPGEWNVWTG
6GUV 4GUWNVU 7TKPGEWNVWTG :/ 2
2QUKVKXG 0GICVKXG
0KVTKVG 2QUKVKXG
0GICVKXG
.' 2QUKVKXG
0GICVKXG
)TCOUVCKPKPI
2QUKVKXG
0GICVKXG
/$4 2QUKVKXG
0GICVKXG
7RNDQDQG.DULH[FHSWIRUWKHVSHFLILFLW\IRUORFDO V\PSWRPV YV 6LQFH TXDQWLWDWLYH
urine culture is the gold standard of UTI diagnosis, both fever and local symptoms should not be used as a diagnostic tool, but only as supporting tools in making presumptive diagnosis of UTI.
Escherichia coli were the most common organ-isms growing in urine culture. This finding was similar to that of previous studies. Predominance of E. coli was mainly attributed to some characteristics that was not found in other organisms, such as p-fimbriae, adherence to uroepithelium in O and K serotype, hemolysin production, and the resistance to the bac-tericidal action or normal human serum.
For many years clinicians have used Gram– staining urine for screening test of UTI in symptom-atic outpatients. In an extensive review, Jenkins et al concluded that examination of a Gram-staining smear of uncentrifuged specimen provided the best microscopic method for detecting bacteriuria. Several previous studies in adults howed that LE and nitrite tests could be used for screening test of UTI, but only the study by Goldsmith and Campos had addressed this issue in pediatric patients.
Table 4 shows that the test with highest sensitiv-ity was Gram staining of urinary smear. This result was similar with that of Olsonet al The test with lowest sensitivity was MBR. The sensitivity of nitrite test in this study was higher than that reported by Goldsmith and Campos, Weinberg and Gan, and Hoberman and Wald. The sensitivity of LE test was also higher than that of previous studies.
The test with highest specificity was MBR,
IROORZHGE\QLWULWHWHVW*UDPVWDLQ
-LQJDQG/(WHVWV,QWKLVVWXG\WKH
specificities of nitrite, LE test, and Gram staining were lower than those reported by others.
+LJKHVW 339 ZDV FRPH IURP 0%5 IROORZHGE\WKHQLWULWHWHVW*UDPVWDLQLQJ DQG/(7KH339RIQLWULWHDQG/(
tests were lower than those reported by Hoberman and Wald. The PPV of Gram staining was higher than that reported by Weinberg and Gan.
The highest NPV was obtained from Gram
stain-LQJIROORZHGE\%05WHVWDQGQLWULWHRU/(
tests. The NPV of Gram staining was similar to that of Weinberg and Gan study,while the NPV of dipstick tests was lower than that of another study.
The MBR test in this study has sensitivity of
VSHFLILFLW\RI339RI139RI DQGDFFXUDF\RI7KHDFFXUDF\ZDVKLJKHVWWKDQ
theother tests. The accuracy of nitrite test, LE test and
*UDPVWDLQLQJZHUHDQGUHVSHF
-tively. Hence, the MBR test was the best for detecting significant bacteriuria. This result was similar as that reported by Supardi. It was concluded that among other urinalysis routine tests, MBR has the highest specificity and accuracy, as well as high sensitivity in establishing a presumptive diagnosis of UTI.
References
.KHU../HLFKWHU+(8ULQDU\WUDFWLQIHFWLRQ,Q.KHU..
Makker SP, editors. Clinical pediatric nephrology. New York:
0F*UDZ+LOO,QFS
+REHUPDQ$:DOG(58ULQDU\WUDFWLQIHFWLRQVLQ\RXQJ
/RKU-$8VHRIURXWLQHXULQDO\VLVLQPDNLQJDSUHVXPSWLYH
diagnosis of urinary tract infection in children. Pediatr Infect
'LV-4. Shaw KN, Gorelick MH. Urinary tract infection in the
pediat-ULFSDWLHQW3HG&OLQ1RUWK$P6XSSO
5. Winberg J, Andersen HJ, Bergstorm T, Jacobsson B, Larson H, Lincoln K. Epidemiology of symptomatic urinary tract
LQIHFWLRQ LQ FKLOGKRRG $FWD 3DHGLDWU 6FDQG 6XSSO
6. Elder JS. Urinary tract infections. In: Behrman RE, Kliegman
50-HQVRQ+%HGLWRUV1HOVRQWH[WERRNRISHGLDWULFVth
HG3KLODGHOSKLD:%6DXQGHUV&RPSDQ\S
7. Hanson LA, Ahlstedt S, Jodal U. The host-parasite
relation-VKLSLQXULQDU\WUDFWLQIHFWLRQV.LGQH\,QW6
8. Bergstorm T. Sex differences in childhood urinary tract
infec-WLRQ$UFK'LV&KLOG
9. Hansson S, Jodal U. Urinary tract infection. In: Barratt TM, Avner ED, Harmon WE, editors. Pediatric nephrology 4th
HG %DOWLPRUH /LSSLQFRWW :LOOLDPV DQG :LONLQV S
:HLQEHUJ $* *DQ 91 8ULQH VFUHHQ IRU EDFWHULXULD LQ
symptomatic pediatric outpatients. Pediatr Infect Dis J
7RNDQ +% .DUL . &OLQLFDO DVSHFWV DQG ZKLWH EORRG FHOO
count in children with urinary tract infection. Pediatr Indones
*ROGVPLWK%0&DPSRV-0&RPSDULVRQRIXULQHGLSVWLFN
microscopy, and culture for the detection of bacteriuria in
FKLOGUHQ&OLQ3HGLDWU
2OVRQ/06KDQKROW]HU&-:LOODUG.(3HWHUVRQ/57KH
slide centrifuge gram stain as an urine screening method. Am
-&OLQ3DWKRO
6XSDUGL , .HVHSDGDQDQ YDOLGLWDV PHWRGH PLNURVNRSL
kimiawi dan biakan air kemih untuk diagnostik