ANATOMIC RECONSTRUCTION OF THE DISTAL
RADIO-ULNAR LIGAMENT AND OSTEOTOMY FOR
MALUNION DISTAL RADIUS AND ULNA WITH
DISTAL RADIO-ULNAR JOINT INSTABILITY:
A CASE REPORT
Oleh :
dr. Putu Mega Wiyastha
Pembimbing :
dr. A.A. Gde Yuda Asmara, Sp. OT
PROGRAM PENDIDIKAN DOKTER SPESIALIS I
BAGIAN/SMF ORTHOPAEDI DAN TRAUMATOLOGY
ANATOMIC RECONSTRUCTION OF THE DISTAL
RADIO-ULNAR LIGAMENT AND OSTEOTOMY FOR MALUNION
DISTAL RADIUS AND ULNA WITH DISTAL RADIO-ULNAR
JOINT INSTABILITY:
A CASE REPORT
Putu Mega Wiyastha*, A.A. Gde Yuda Asmara**,
* Orthopaedic and Traumatology Resident of Udayana University, Sanglah Hospital Denpasar **Teaching Staff of Orthopaedic and Traumatology of Udayana University, Sanglah Hospital Denpasar
Introduction
Stability of the distal radioulnar joint (DRUJ) is provided by bony architecture and by soft tissues such as the triangular fibrocartilage complex (TFCC), the joint capsule, and surrounding muscles. Anatomic reconstruction of the major structures
responsible for joint stability is the most important principle for the treatment of instability of an injured joint with an intact articular surface by using a palmaris longus tendon graft.
Case
Male, 19 year old with DRUJ instability associated with distal radial and ulna malunion. Patient had history of trauma two years ago. On examination there is restricted of the Range Of Motion (ROM) wrist flexion-extension and forearm
supination. The management with corrective osteotomy of the distal radius and ulna
with the radioulnar ligament reconstruction.
Discussion
Restoration of stability and a full painless arc of pronation–supination are the goals of treatment for the posttraumatic unstable DRUJ. The reconstruction procedures
suggested by some authors using the palmaris longus tendon has been shown to be the most reliable and anatomically acceptable surgical technique. We performed distal radioulnar ligament reconstruction after osteotomy distal radius and ulna then fixation using plate and screw.
ANATOMIC RECONSTRUCTION OF THE DISTAL
RADIO-ULNAR LIGAMENT AND OSTEOTOMY FOR MALUNION
DISTAL RADIUS AND ULNA WITH DISTAL RADIO-ULNAR
JOINT INSTABILITY:
A CASE REPORT
Putu Mega Wiyastha*, A.A. Gde Yuda Asmara**,
* Orthopaedic and Traumatology Resident of Udayana University, Sanglah Hospital Denpasar
**Teaching Staff of Orthopaedic and Traumatology of Udayana University, Sanglah Hospital
Denpasar
Introduction
Stability of the distal radioulnar joint (DRUJ) is provided by bony architecture and by
soft tissues such as the triangular fibrocartilage complex (TFCC), the joint capsule,
and surrounding muscles. Anatomic reconstruction of the major structures
responsible for joint stability is the most important principle for the treatment of
instability of an injured joint with an intact articular surface by using a palmaris
longus tendon graft.1
Many authors have made various attempts to restore DRUJ stability surgically
following trauma. Some have employed indirect methods such as tenodesis using the
flexor carpi ulnaris tendon or the extensor carpi ulnaris tendon. However, these
nonanatomic procedures are not reliable in that the normal stability of the joint is not
restored and the joint motion may be restricted. Anatomic reconstruction of the major
structures responsible for joint stability is the most important principle for the
treatment of instability of an injured joint with an intact articular surface. In this
sense, some authors have tried to achieve anatomic reconstruction of the volar and
The objective of this study was to analyze clinical outcomes after anatomic
reconstruction of the distal radio-ulnar ligaments in a patient with post-traumatic
chronic instability of the DRUJ.
Case
Male, nineteen years old with DRUJ instability associated with distal radial and ulna
malunion. Patient had history of trauma two years ago and treated in bone setter.
History of fever denied by the patient. Patient was a student. On examination there is
deformity angulations and shortening on the left wrist without tenderness on
palpation. The piano key sign was positive. restricted of the range of motion (ROM)
wrist flexion-extension and forearm supination.
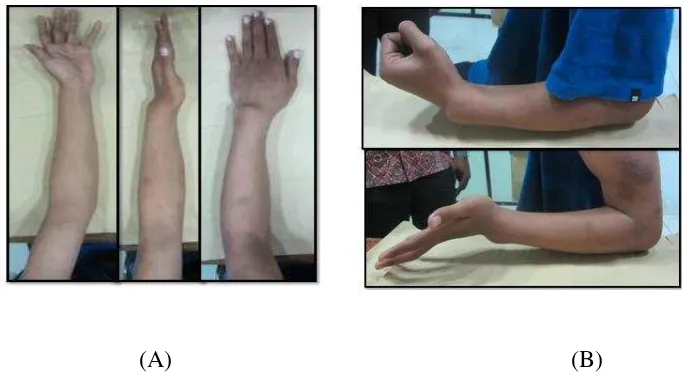
(A) (B)
Figure 1. (A) shows the clinical picture pre operative with deformity angulation and
shortening of the left wrist. (B) shows restricted flexion-extension active ROM of the
Figure 2. Shows the clinical picture pre operative with restricted supination-pronation
active ROM of the left forearm
First we correct the malunion distal radius with osteotomy and fixation with
locking small T-plate three hole, then we do osteotomy and correction deformity
distal ulna with fixation using locking one third tubular plate six hole. We use
Palmaris longus tendon as a graft for stabilization distal radioulnar joint. The site for
the tunnel in the radius is prepared, we use guidewire for a 2 mm cannulated drill bit
is driven through the radius a few millimeters proximal to the lunate fossa and radial
to the articular surface of the sigmoid notch.
The cannulated drill bit is used to create a pilot tunnel. The tunnel is
progressively enlarged with standard drill bits, if necessary, to accommodate the
tendon graft. Then we use ligament sling for stabilize the distal radio ulnar joint. In this case we didn’t do osteotomy simoid notch. The last we use K-wire 1.4 mm to stabilize the distal radioulnar joint and we plan remove after 3 weeks.
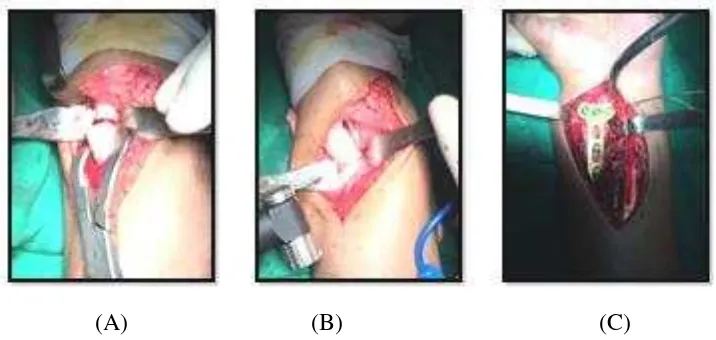
Figure 3. The clinical picture intra operative when osteotomy the radial bone (A) and
(B) clinical picture of the osteotomy distal ulna, (C) fixation distal radius using distal
radial locking plate
(A) (B) (C)
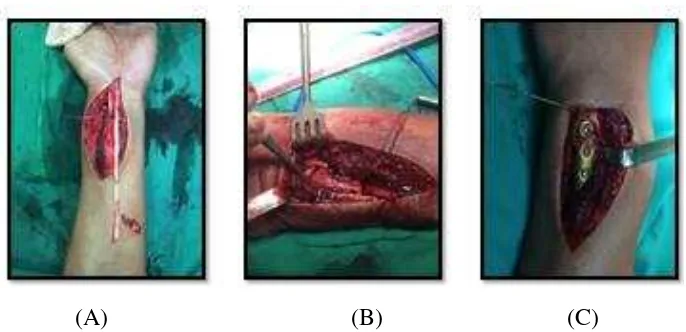
Figure 4. (A) show the Palmaris longus tendon as a graft for stabilization distal
radioulnar joint, (B) and (C) clinical picture of the radial and ulnar side with Palmaris
Figure 5. Show the X-ray post operative. We use K-wire about 3 weeks.
Figure 6. The clinical picture 4 weeks after operation, show the deformity was
reduced.
Discussion
The distal radioulnar ligaments are key stabilizers of the distal radioulnar joint
(DRUJ). When these ligaments fail to heal adequately after injury, DRUJ instability
may develop. Reconstruction of the distal radioulnar ligaments offers the best
Numerous techniques have been described, which can be classified into 3 categories:
(1) a direct radioulnar tether that is extrinsic to the joint, (2) an indirect radioulnar
link through an ulnocarpal sling or a tenodesis, or (3) reconstruction of the distal
radioulnar ligaments.1,3
In patients with radial malunion, a planned osteotomy was performed prior to
distal radioulnar ligament reconstruction to restore normal DRUJ alignment. After
proper internal fixation was applied, an anteroposterior stress test was performed to
determine the necessity of distal radioulnar ligament reconstruction. Because
instability was still observed in all patients, distal radioulnar ligament reconstruction
was performed at the same time. In one patient with radial shaft malunion, distal
radioulnar ligament reconstruction actually preceded osteotomy because the
preoperative angular deformity on the sagittal plane was not definite, but subluxation
during supination was observed requiring additional distal radius osteotomy.1,4
A palmaris longus tendon graft was harvested, and each end of the graft was
connected to a thread to facilitate easy passage through the tunnels. The periosteum
was dissected from the distal and dorsal margin of the sigmoid notch to make an
anteroposterior tunnel in the radius. A guide wire was inserted in parallel with the
articular surface of the sigmoid notch. The proper guide wire position was checked
with a C-arm followed by creation of a 3-4 mm tunnel for the graft without damaging
the subchondral bone of the radiocarpal joint and the sigmoid notch. A 2 cm
transverse incision was made over the volarly protruding guide wire to expose the
volar opening of the tunnel and the volar side of the DRUJ. A 2.0 mm drill hole was
made in the radius, then gradually enlarged with a straight curette to allow for
passage of the tendon graft . To make the ulnar tunnel, the wrist was flexed volarly
and the TFCC was pulled distally to expose the ulnar fovea. With the ulna pulled
dorsally, a tunnel was made through the ulnar fovea at a tilt angle toward the ulnar
side of the ulnar neck in the same way for the radial tunnel. The tendon graft was
passed through the radial tunnel and both of its limbs were brought to the opening in
hemostat was used to pierce the anterior capsule between the ulnar head and the
TFCC without damaging the ulnar nerves or vessels.1,5
Both limbs were passed through the ulna tunnel to the ulnar side of the ulnar
neck. The limb on the volar side surrounded the ulna and was sutured with the other
limb using 3-0 nonabsorbable sutures. During the suturing procedure, both limbs
were pulled taut with the forearm in neutral position, and care was taken not to
restrict forearm rotation by imposing excessive tension. Motion of the wrist joint and
the DRUJ was checked, and the final status of the reconstructed tendon was assessed
Reference
1. Adams BD, Berger RA. An anatomic reconstruction of the distal radioulnar
ligaments for posttraumatic distal radioulnar joint instability. J Hand Surg
Am. 2002;27(2):243-51.
2. Lawler E, Adams BD. Reconstruction for DRUJ instability. Hand (N Y).
2007;2(3):123-6.
3. Sahoo J. Anatomic reconstruction of the distal radioulnar ligament for distal
radioulnar joint instability: a case report. IJPMR June 2013; Vol 24 (2):
48-50.
4. Kyu Nam Seo, Min Jong Park, Hong Je Kang. Anatomic Reconstruction of
the Distal
5. Radioulnar Ligament for Posttraumatic Distal Radioulnar Joint Instability.
Clinics in Orthopedic Surgery 2009;1:138-145
6. Adams BD. Post-Traumatic (Chronic) Distal Radioulnar Joint Instability.