i
Nepal Malaria Strategic
Plan 2011-2016
(Revised Version- December 2011)
ii
II.3 FEDERALISM AND THE HEALTH SECTOR ... 15
II.4 DEMOGRAPHIC INFORMATION:... 15
II.5 ECOSYSTEM, ENVIRONMENT AND CLIMATE ... 15
II.6 SOCIO-ECONOMIC SITUATION ... 17
III. HEALTH SYSTEM ANALYSIS ... 18
III.1 DECENTRALIZATION AND MANAGEMENT OF HEALTH FACILITIES ... 20
III.2 ORGANIZATIONAL STRUCTURE OF EPIDEMIOLOGY AND DISEASE CONTROL DIVISION ... 21
III.3 MALARIA CONTROL PROGRAM STAFFING ... 21
III.4. VECTOR BORNE DISEASE RESEARCH AND TRAINING CENTRE (VBDRTC) ... 22
III.5 PUBLIC-PRIVATE PARTNERSHIPS ... 22
III.6 HEALTH MANAGEMENT INFORMATION SYSTEM (HMIS) ... 22
IV. MALARIA SITUATION ANALYSIS ... 22
IV.1 EPIDEMIOLOGY ... 22
IV.1.1 Malaria species ... 23
IV.1.2Malaria vectors ... 23
IV.1.3 Malaria Dynamics ... 23
IV.1.3.1 Age and sex wise Distribution of Malaria Cases ... 25
IV.2 MALARIA STRATIFICATION AND MAPPING ... 25
IV.3 THE MALARIA PROGRAM PERFORMANCE DURING LAST FIVE YEARS ... 27
IV.3.1 Entomology and Vector Control ... 27
IV.3.2 Early Diagnosis and Prompt Treatment ... 30
IV.3.3 Surveillance and Epidemic Preparedness ... 33
IV.3.4 Behavior change communication (BCC) ... 33
IV.3.5 Program Management ... 34
IV.4 SWOT ANALYSIS ... 38
IV.4.1 SWOT Analysis (Vector Control) ... 38
IV.4.2 SWOT Analysis (Diagnosis and Treatment) ... 39
IV.4.3 SWOT Analysis (Surveillance, Epidemic Preparedness and Response) ... 40
IV.4.4 SWOT Analysis (Behavior Change Communication) ... 41
IV.4.5 SWOT analysis (Program Management) ... 42
V. NEPAL MALARIA STRATEGIC PLAN 2011 – 2016 ... 43
V.1 VISION ... 43
V.2 MISSION ... 43
V.3 GOAL ... 43
V.4 OBJECTIVES ... 43
VI. STRATEGIC INTERVENTION ... 43
VI.1 MICRO STRATIFICATION ... 43
iii
VI.3 DIAGNOSIS AND TREATMENT ... 47
VI.4 SURVEILLANCE, EPIDEMIC PREPAREDNESS AND RESPONSE ... 48
VI.5. BEHAVIORAL CHANGE COMMUNICATION (BCC) ... 50
VI.6 PROGRAM MANAGEMENT ... 50
VI.7 BUDGET ... 54
VII. MONITORING AND EVALUATION ... 55
VII. 1 PERFORMANCE FRAMEWORK ... 55
VII.2 TRACKING PROGRESS ... 57
VII.3 MONITORING OUTCOME INDICATORS ... 58
VIII. BUDGET FOR NMSP 2011-2016 ... 61
ANNEXES ... 65
ANNEX-1: AN OUTLINE OF THE LONG-TERM NATIONAL MALARIA ELIMINATION STRATEGY (2011/12 – 2025/26) 65 ANNEX-2: MALARIOMETRIC INDICATOR, NEPAL 2004-2010 ... 70
ANNEX-3: RANGE OF API BY VDC, 2010 (13 DISTRICTS) ... 70
ANNEX- 4: RANGE OF API BY VDC, 2010 (18 DISTRICTS) ... 70
ANNEX- 5: INDOOR RESIDUAL SPRAYING COVERAGE OF HIGH RISK AREA 2004-2009 ... 71
ANNEX-6: LLIN COVERAGE OF HIGH RISK AREAS, 2006-2010 ... 71
ANNEX-7: MALARIA PROFILE OF DIFFERENT MALARIA RISK AREAS, 2010 ... 71
ANNEX -8: STRATIFICATION OF MALARIA RISK IN NEPAL ... 72
ANNEX-9: ... 76
ANNEX-10: ENTOMOLOGY /VECTOR CONTROL CAPACITY ASSESSMENT AND DEVELOPMENT ... 78
ANNEX- 11: PLAN FOR THE DEVELOPMENT OF VECTOR BORNE DISEASE RESEARCH AND TRAINING CENTRE ... 82
iv
Foreword
Nepal has arrived at a critical junction in its fight against malaria. The country has set and exceeded targets set at the World Health Assembly and by the Millennium Development Goals to cut malaria morbidity and mortality by 2010 and the country is in a unique position to move towards eliminating the local indigenous transmission of malaria. The Ministry of Health and Population, with the support of its partners, has implemented a strong malaria control program, steadily improving the coverage and quality of indoor residual spraying, introducing long lasting insecticide-treated nets, and increasing access to rapid malaria diagnosis and new effective Artemisinin-based combination treatment.
The Ministry of health and population, through its National Malaria Control Program, has ambitious vision of a malaria-free Nepal by 2026. Over the next 5 years, our priority will be to consolidate the gains we have made and sustain the downward trend in malaria morbidity and mortality and maintain outbreak free status.
Review of the National Malaria Control Program in 2010 by a joint internal and external panel of technical reviewers concluded that the program has progressed from control to pre-elimination stage. Malaria preventive, diagnostic and curative services are free of charge in all health facilities. Malaria elimination is an achievable ambitious goal. Activities need to be reoriented according to the current epidemiology of malaria in Nepal and to fulfill gaps between control and pre-elimination program. Sensitive surveillance system and appropriate response is one of the key components and has to be strengthened to achieve this goal. Progress towards target needs to be incorporated into a strong monitoring and evaluation system synchronizing the potentials of the public sector and technical partners. As malaria is a focal disease in Nepal, activities and strategies need to focus on halting indigenous transmission of malaria. The management of our interventions must extend to the community level and household level in all malaria endemic foci. Community participation and community mobilization therefore has a key role to play in ensuring that all Nepalese own and take part in this national goal. As elimination is not possible without coordination and concerted effort with India, advocacy at regional level and migrant related malaria will receive specific focus in the strategy.
Finally, I would like to acknowledge the continuous support provided to the National Malaria Program by the Global Fund and WHO. I would also like to express my sincere thank to all stake holders including PSI. At this critical moment of embarking on the next stage in the fight against malaria, I look forward to renewed commitment from all partners and urge all stakeholders to
support our national goal of “Malaria-free Nepal by 2026”.
____________________________ ..……….
Dr Praveen Mishra Date
Secretary
v
Foreword
It is my pleasure to write a few words about the Nepal Malaria Strategic Plan 2011-2016 with a vision of malaria free Nepal by 2026. Malaria is endemic in 65 districts of Nepal and continues to be one of the national priority public health programs. Majority (73%) of the national population lives in malaria risk area. Malaria disproportionately affects the poor and socially marginalized residing in malaria clusters and mobile population. The disease mainly affects adults in productive age group and is a major cause of poverty.
Malaria burden in Nepal has declined as there has been a reduction of about 40% confirmed cases during the last five years. National Malaria Control Program assessment by international and national experts was undertaken in 2010. The experts have concluded that transmission of malaria in Nepal is low and that the program has moved forward from control to pre-elimination stage. They have suggested that it is now time for Nepal to adopt pre-elimination strategy and prepare for malaria elimination from Nepal.
As malaria is a focal disease in Nepal, activities and strategies need to focus on halting indigenous transmission of malaria. The management of our interventions must extend to the community level and household level in all malaria endemic foci. Community participation and community mobilization therefore plays a key role in ensuring that all Nepalese own and take part in this national goal. As elimination is not possible without coordination and concerted effort with India, advocacy at regional level and migrant related malaria will receive specific focus in the strategy.
National Malaria Control Program has set an ambitious vision of a malaria-free Nepal by 2026. Nepal Malaria Strategic Plan 2011-2016 has projected to reduce the number of indigenous cases by 90% of the current levels. Over the next 6 years, our priority will be to consolidate the gains we have made and sustain the downward trend in malaria morbidity and mortality and maintain outbreak free status of the country.
Finally, I would like to acknowledge the continuous support provided to the National Malaria Program by the Global Fund to Fight AIDS, TB, and Malaria, the World Health Organization and Population Services International. At this critical moment of embarking on the next stage of combating malaria, I look forward to a broad partnership from all partners and urge all
stakeholders to support our national goal of “Malaria-free Nepal by 2026”.
………
Dr. Y. V. Pradhan Date ………..
Director General
vi
Foreword
Malaria control in Nepal has been identified as priority-I public health program under the National Health Sector Program Implementation Plan-II (NHSP-II) 2010- 2015. Malaria control services are rendered free of cost and emphasize on the accessibility of services by high risk and vulnerable groups and marginalized remote populations.
The country has exceeded targets set in Millennium Development Goals (MDG) as well as the targets of Global Roll Back Malaria (RBM). A comprehensive independent External Evaluation of the National Malaria Program was conducted in June 2010. The review report recommended to consolidate and sustain the achievements of malaria control program and suggested that the country should embark upon pre elimination with an ultimate goal of elimination of malaria. During the Joint Assessment of National Disease Strategy (JANS), an external independent JANS team also suggested several actions and recommendations to improve the national strategic plan. Based on these recommendations the Malaria Program has developed an outline of a long term malaria elimination strategy.
Based on long term strategy 2011-2026, Epidemiology and Disease Control Division under the Department of Health Services has taken a lead in the development of five year Malaria Strategic Plan-2011-2016. This document has been updated through a consultative workshop attended by representatives from affected community, DHOs, civil society, RHDs, CHD, FHD, NPHL, VBDRTC, NHEICC, professional societies, health/academic institutions, External Development Partners, INGO and malaria experts. Summary recommendations of these consultative meings are provided in annexes. The draft document was also checked for appropriateness at local level. This document will provide the key strategic direction that will reorient the program to gear up for elimination. The country is in the process of restructuring the administrative setup and moving towards federalism, as a result, there will be a political stability in near future. It also considers the context in which this reorientation will occur and proposes ways in which the opportunities and constraints of the external factors can be managed to achieve the larger vision of elimination.
Main focus of pre-elimination program will be elimination of transmission foci. In this program, systems must be strengthened to identify and treat all confirmed malaria cases including the asymptomatic cases and significantly reduce human-mosquito contact. These two shifts will be facilitated by the implementation of active surveillance and targeted interventions as outlined in this Strategic Plan.
Finally, I would like to thank and acknowledge the efforts of the past and present health work force of malaria, the donors and partners for contributing to outstanding results in malaria and urge all to sustain the current momentum of malaria program to achieve further success. As we move forward to malaria elimination we will continue to advocate securing financing for the program from the government and urging for renewed commitment from partners.
……….. ……….
Dr. G.D. Thakur Date
Director
Epidemiology and Diseases Control Division Department of Health Services
vii
Executive Summary
Malaria control in Nepal has been identified as priority-I public health program under the Nepal Health Sector Program Implementation Plan-II (NHSP-II) 2010- 2015. Second Long Term Health Plan 1997-2017 has indicated disease management, vector control and epidemic prevention and control and community participation as broad strategies and Three Years Interim Plan guides implementation of malaria control. Malaria control services are rendered free of cost and emphasize on the accessibility of services by high risk and vulnerable groups like pregnant women, children and marginalized remote populations.
Malaria control program has already achieved MDGs goals, universal coverage of malaria control interventions and RBM targets of 2010. Nepal Malaria Strategic Plan 2011-2016 has a vision of malaria free Nepal by 2026 and is based on the Long Term National Strategy of Malaria Elimination. The immediate task before the program is to consolidate the gains achieved so far and reorient the program from control to elimination.
This strategic plan will steer intensified malaria control viz a viz pre- elimination phase. Micro stratification of malaria endemic areas of the country will be carried out. The impact target of this plan is to consolidate and sustain the achievement of API below 1 per 1000; 90% reduction in the incidence of indigenous malaria cases by 2016. Similarly by 2016, at least 90% vector control coverage in high risk areas, 90% parasitological diagnosis of all suspected cases; 100% effective treatment of all confirmed malaria cases; introduction of notification and active surveillance; ensure 90% of population at malaria risk adopt at least one malaria preventive measures by BCC approach by 2016 are major outcome targets of this strategic plan.
WHOPES certified quality LLIN distribution, good quality IRS, social mobilization, good quality malaria microscopy, quality bivalent RDTs, WHO prequalified antimalarials and laboratory equipment are the basic tools for strategic intervention. Intensified surveillance including notification, active case detection, and gradual elimination of active malaria foci and management of imported cases are keys to pre-elimination.
Strong administrative and technical management are key essential factors for effective and efficient delivery of services. Program management capacity will be boosted up through high level advocacy to establish key positions in National Malaria Program. Besides that, holistic package of carefully tailored technical and management training towards reorientation of the staff will be developed and implemented to strengthen the delivery of services at all levels. The program will foster partnership with WHO and other international and national organizations. Inter-sectoral collaboration with other line Ministries of the Govt. of Nepal would be further strengthened as they are crucial for program implementation.
viii
goal of elimination of malaria within the set time frame, and the program will be at risk of maintaining the achievements gained so far. To combat this issue the program will make special efforts not to let the disruption of essential services jeopardize the gains of the program; and gear up the surveillance for prevention and control of outbreaks.
High level advocacy is also expected to secure government financing for malaria at a minimum current level and increase proportionately in the future to achieve malaria free Nepal by 2026. However, it is obvious that the funds required for the implementation of the program, which are based on international principles and best practices is quite high and may not be met by current resources of the National Malaria Program. Therefore, the support of all stake holders, national and international partners (WB,GF,WHO,DFID,and others), is solicited for the implementation of the program.
ix
Abbreviations
ABER Annual Blood Examination Rate ACT Artemisinin Combination Therapy ANC Ante-Natal Care
APMEN Asia Pacific Malaria Elimination Network BCC Behavior Change Communication
CCM Country Coordination Mechanism DCS Disease Control Section
DDA Department of Drug Administration DHO District Health Office
DoHS Department of Health Services DPHO District Public Health Office
EDCD Epidemiology and Diseases Control Division EDPs External Development Partners
EHS Essential Health Care Services EWARS Early Warning and Reporting System FCHV Female Community Health Volunteer GMP Good Manufacturing Practice
GoN Government of Nepal
HFMC Health Facility Management Committee HMD Health Management Division
HMIS Health Management Information System
HP Health Post
IEC Information Education and Communication INGO International Non-Government Organization IRS Indoor Residual Spraying
ISO International Standards Organization IVM Integrated Vector Management LLIN Long Lasting Insecticidal Net LMD Logistics Management Division M&E Monitoring and Evaluation MoH Ministry of Health
MoHP Ministry of Health and Population MI Malaria Inspector
NGO Non-Government Organization
NHEICC National Health Education, Information and Communication Centre NHTC National Health Training Center
NPHL National Public Health Laboratory PHC Primary Health Center
PMU Program management Unit PSI Population Services International RBM Roll Back Malaria
RDT Rapid Diagnostic Test
x SWAp Sector Wide Approach
TA Technical Assistance TB Tuberculosis
TWG Technical Working Group
VBDRTC Vector Borne Disease Research and Training Centre VCA/I Vector Control Assistant/Inspector
VCO Vector Control Officer
VDC Village Development Committee WHO World Health Organization
WHOPES World Health Organization Pesticide Evaluation Scheme
11
I. INTRODUCTION
Nepal is a landlocked sovereign state in South Asia. It is located in the Himalayas and bordered to the north by the People's Republic of China, and to the south, east, and west by the Republic of India with an area of 147,181 square kilometers (56,827 sq mi) and a population of approximately 27 million. Nepal is divided into three physiographic areas: Mountain, Hill and Terai. These ecological belts run east-west and are vertically intersected by Nepal's major, north to south flowing river systems.
Malaria is predominantly found in Terai belt bordering India. There are altogether 75 districts and malaria is endemic in 65 districts and about 73% population of the country are at malaria risk. In 2010 indigenous transmission was reported from 40 districts, and population with indigenous transmission will be substantially reduced after micro-stratification which is starting soon. Malaria mainly affects adults in productive age group and has direct impact on national economy. Malaria is one of the first priority public health programs as explained in Nepal Health Sector Program – Implementation Plan (NHSP-IP). Government of Nepal also has prioritized malaria program in its Second Long-Term Health Plan (SLTHP) 1997-2017.
Due to successful malaria control program, malaria cases dramatically decreased over the years and there were only 2,787 malaria cases in the country in 1971. Due to resurgence of malaria in the South-east Asia Region during mid-seventies, the malaria eradication program was converted to control in 1978. During the control period highest numbers of laboratory confirmed cases- 42,321 were recorded in 1985. Over the years, due to deployment of strategic interventions, malaria cases have steadily declined with minor out breaks and during 2010, only 3,115 cases were reported.
The country has exceeded targets set in Millennium Development Goals (MDG) as well as the targets of Global Roll Back Malaria (RBM). A comprehensive independent External Evaluation of the National Malaria Program was conducted in June 2010. The review report recommended to consolidate and sustain the achievements of malaria control program and suggested the country should embark upon pre elimination with an ultimate goal of malaria elimination.
12
This document will provide the key strategic direction that will reorient program to gear up for elimination. The Strategic Plan (together with the Monitoring and Evaluation Plan) will also serve to assist with benchmarking, monitoring, and periodic evaluation of performance, based on the goals, objectives, and target areas outlined in this strategy. The country is in the process of restructuring the administrative set up and moving towards federalism, as a result, there will be a political stability in near future. It also considers the context in which this reorientation will occur and proposes ways in which the opportunities and constraints of the external factors can be managed to achieve the larger vision of elimination.
Main focus of pre-elimination program will be elimination of transmission foci. In this program, systems must be strengthened to identify and treat all confirmed malaria cases including the asymptomatic cases and significantly reduce human-mosquito contact. These two shifts will be facilitated by the implementation of active surveillance and targeted interventions as outlined in this Strategic Plan.
This Strategic Plan will answer the following key questions.
1. What is the current malaria situation in Nepal and how has it evolved over the duration of the expiring Roll Back Malaria Strategic Plan 2007 – 2011. What was the performance of the expiring Strategic Plan and what are the best practices and lessons learned?
2. What are the strengths, weaknesses, opportunities, and threats of the current approach towards malaria control, and what are the implications for elimination?
3. What factors, external to the NMCP, will affect reorientation to elimination? (Health systems – public and private delivery of health care)
4. Which evidence-based interventions will be used to achieve the strategic shift, and how will they be adapted for different transmission risk areas?
5. What are the goals, objectives, and targets of Nepal with regards to pre-elimination by 2016?
6. What are the national policies that are in place (or need to be revised) to support this strategic shift?
7. How will this strategy be managed by the MoHP and its malaria program partners? How will partnerships be coordinated?
13
II. COUNTRY PROFILE
II.1 Socio-political system
Nepal is a landlocked country having area 147,181 square kilometers. It has border with India to the south, east and west and China to the north, at the southern flank of the Himalayas. The
country’s geographic zones vary greatly and represent one of the challenges for development of
the nation. The majority of the country remains under-developed and over 80% of the population lives in rural areas. Nepal is ecologically divided into three distinct ecological zones: the Mountains to the north, the Hills, and the Terai to the south. The country is divided into 5 development regions (Eastern, Central, Western, Mid-western and Far-westerner), 14 Zones and 75 Districts. Districts are further divided into VDCs and Municipalities. There are altogether 3,912 VDCs and 58 municipalities including one metropolitan and three sub metropolitan cities. Each VDC is divided in 9 wards which sum up to 36,000 wards countrywide. Figure1 shows the main topographical features of the country.
Figure1. Transect of Nepal (Schematic) showing main topographical features
II.2 Health Policy
The Government of Nepal’s National Health Policy of 1991 has sought “to upgrade the health
standards of the majority of rural population by strengthening the primary health care system and
making effective health care services readily available at the local level.” Access to essential
14
to travel 1-4 hours to reach the nearest health or sub-health post. In the Hill Region, 30% people have to travel 1-4 hours to reach the nearest health post or sub-health post.
A large number of health institutions have been established by the private sectors to train health care professionals and the numbers of private hospitals are growing quickly thereby greatly
expanding secondary and tertiary care in urban areas. Nepal’s pharmaceutical industries also
grew in the last twenty years and now produces one-third of the national requirement for medicines.
In 2004, the Government of Nepal (GoN) introduced a “Health Sector Strategy: An Agenda for
Reform” and the first “Nepal Health Sector Program 2004-2009”. Recognizing that external
development partners finance over 40% of public-sector health expenditure, Government adopted a Sector Wide Approach (SWAp) for NHSP, to improve assistance effectiveness by coordinating the efforts of Government and External Development Partners (EDPs) in support of a single Government-owned and led program that aimed to put the country on track to achieve Millennium Development Goals for health by 2015.
With the popular people’s movement of April 2006 came a period of transition that led to an
Interim Constitution, electing a constituent assembly, and formation of a federal democratic republic of Nepal. The Interim Constitution established the right of all Nepali citizens to free basic health services, the right to a clean environment, access to education and a means of livelihood, in a social environment free of discrimination and institutionalized inequality.
During the past two decades, amidst profound political change and instability, and with a largely poor, rural population living among formidable natural barriers to public services, Nepal has taken initiatives that have achieved significantly improving equity of access to health services, beginning to reduce the extreme disparities between the poor and rich, to improve the access of the marginalized castes and ethnic groups. The improvement in the health status of the poor and marginalized people is notable because it has taken place in a context in which the incidence of poverty decreased markedly between1996-2004 from 41% to 31 %, but the overall disparity between rich and poor has increased. The wealthiest consume eight times more than the poorest, and 3 of 10 Nepali citizens remain below the poverty line.
Today, essential health care services at Health Posts, Sub-health posts and Primary Health Centers are free of charge to all. At district hospitals, outpatient, in patient and emergency services are free of charge to poor, vulnerable, and marginalized groups, including medicines, and 40 essential medicines are free of charge to all. Institutional deliveries are free of charge to all pregnant women nationwide.
15
II.3 Federalism and the Health Sector
In the present context, Nepal’s constituent assembly established by the interim constitution (2006) based on the principle of federalism, is working to have a full fledged constitution with clear structures of federalism and its operational modality.
Whatever form of federal system Nepal will adopt in its new constitution, the need for preparing the country's institutions for the transition to federalism has already arisen. Notably, the federal structure will affect every area of the health system, from planning to service delivery and overall health governance. However, basic elements of structure and function may remain same and only the governance may change, which is yet to be defined by the Constituent Assembly. Therefore, at this time the future functions of different levels of government are yet to be decided, but malaria pre-elimination with the aim of elimination by 2026 shall be in accordance with the National Malaria Strategic Plan.
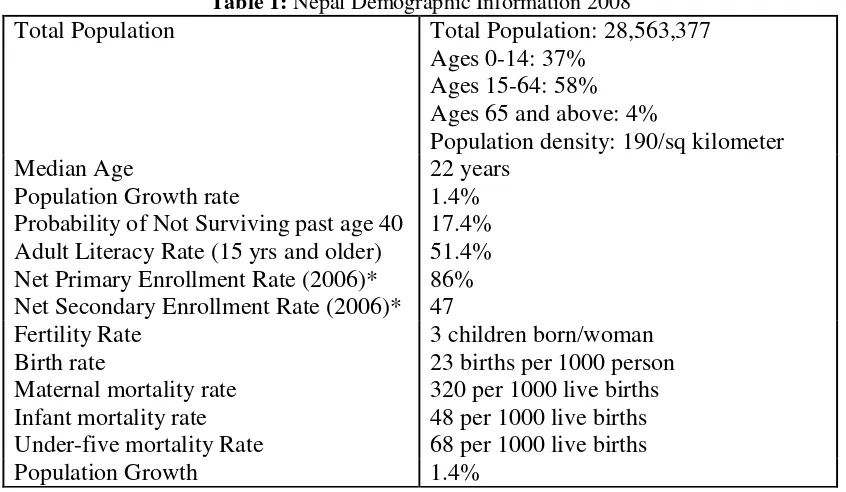
II.4 Demographic Information:
The demographic information at a glance, in the table below, clearly shows the current status in term of population growth, mortality and median ages.
Table 1: Nepal Demographic Information 2008
Sources: Human development Report 2007/2008, Country Fact Sheets * Nepal Demographic and Health Survey, 2006
II.5 Ecosystem, environment and climate
The country’s geographic zones vary greatly and represent one of the challenges to development
across the nation. The majority of the country remains under-developed and over 80% of the population lives in rural areas. Repetition
Total Population Total Population: 28,563,377 Ages 0-14: 37%
Probability of Not Surviving past age 40 Adult Literacy Rate (15 yrs and older) Net Primary Enrollment Rate (2006)* Net Secondary Enrollment Rate (2006)*
22 years
Fertility Rate 3 children born/woman
16
The Hill region, situated south of the Mountain Region, this zone ranges in altitude from between 700 and 4,000 meters. This region begins at the Mahabharata Range. These steep southern slopes are nearly uninhabited, thus an effective buffer between languages and culture in the Terai and Hill regions. Northern slopes are gentler and moderately well populated. The increasingly urbanized Kathmandu and Pokhara valleys fall within this region. Beyond microclimates suited to rice cultivation and proximity to water for irrigation, these cultivate maize, millet, barley and potatoes as staple crops. Temperate and subtropical fruits are grown as cash crops. Outside the rice-growing lower valleys, hill populations suffer chronic food deficits.
Hills comprise of 41.7% of Nepal’s land surface and contain 44.3% of the population. Although
there is malaria transmission in the valleys, but these valleys are included in the high risk areas. Transportation and communication facilities are much more developed here than in the mountain region.
Terai region in the southern part of the country can be regarded as an extension of the relatively flat gigantic plains, and comprises only 23.1% of the total land area but contains over 48.4% of the population. Terai is vital to the nation as it contains the most fertile agriculture land and forests. Because of its flat terrain, transportation and communication facilities are more developed than in the other two regions of the country. Eco-system of this belt is very favorable for breeding of mosquitoes the proven vectors of malaria, Japanese encephalitis, dengue and Lymphatic filariasis. Malaria cases are found in Terai all over including the towns. So far there was no intervention in the towns, but all towns in Terai have been included for intervention under the malaria elimination strategy.
17
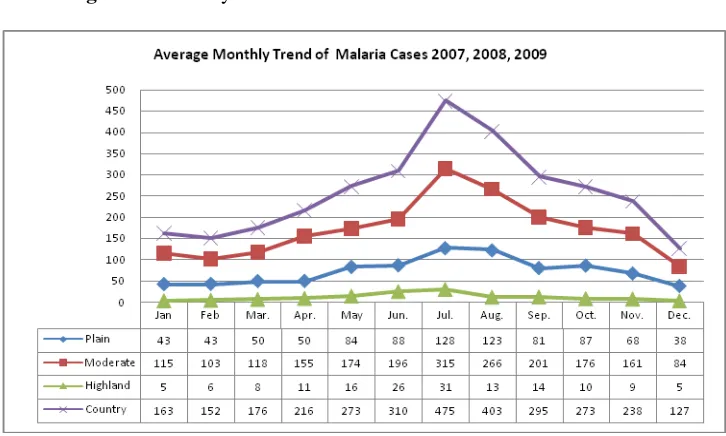
Figure 3. Monthly distribution of malaria cases in different stratum
II.6 Socio-economic situation
Nepal is among the poorest and least developed countries in the world with almost one-third of its population living below the poverty line and with an unemployment rate of 46%. It is ranked 144 out of 177 nations on the United Nation’s Human Development Index (HDI) and falls well short of recent HDI gains made by the South Asia region as a whole. The gross domestic product (GDP) per capita (PPP) was $1,100 in 2008. The total literacy rate for male is 81.0% and for female is 54.5% (Human Development Report 2009).The life expectancy at birth is 70.18 and 66.19 years for female and male respectively (HDR 2009).
It has been observed from the past that migration of the people from non- malarious region to malarious region for the development projects , migration to India for economic purposes and migration of people to endemic region for rice paddy cultivation facilitates malaria transmission. The urban housing scenario is not encouraging in Nepal. More number of people are living in rented houses, the overcrowding indices is high; the infrastructure is not meeting the need of the people whether it be water supply or sanitation. The number of squatted is increasing and the slum areas are also following the same trend.
18
Malaria is being reported from 65 districts in Nepal and continues to be one of the priority public health problems. Majority (73%) of the population live in malaria risk area. Malaria disproportionately affects the poor and socially marginalized people. Malaria and poverty are intimately connected and malaria affects mainly the ethnic minorities, poor, mobile population groups, young adults and those living in border areas. Malaria is both a cause and a consequence of poverty slowing economic growth in endemic areas.
III. HEALTH SYSTEM ANALYSIS
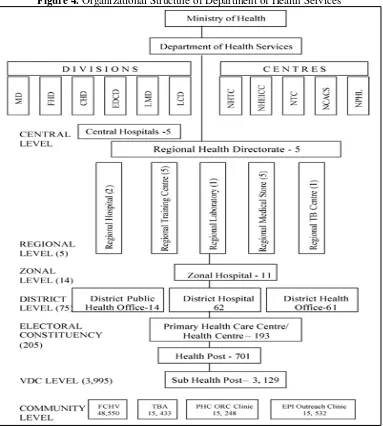
Govt. of Nepal has 22 ministries. Ministry of Health & Population is mandated with the development of policies, plan; monitoring & supervision of the activities implemented through different tiers of the health system including Department of Health Services, Regional Health Directorate, District Public Health Offices and regulating the activities related to health sector. The Department of Health Services is responsible for the implementation of preventive and curative health services throughout the country planned and budgeted by the MoHP and is one of the three departments under the Ministry of Health. All preventative health programmes are carried out by the DPHO/DOHs, headed by a Public Health Officer/Medical Officer. The other staffs in DPHO/DHO include vector-control assistant, malaria inspector, laboratory technician and laboratory assistant. DoHS, it’s Divisions, RHDs, DPHOs, Hospitals and peripheral health facilities spread throughout the country
19
Figure 4. Organizational Structure of Department of Health Services
At the district level, each Ministry has offices that manage the planning and implementation for their respective sector. The DHO co-ordinates health development activities in the district through the District Development Committee (DDC) and is responsible for all health-related activities in the district including the organization and management of district hospitals, Primary Health Care Center (PHCC), Health Posts (HP) and Sub-Health Posts (SHPs).
20
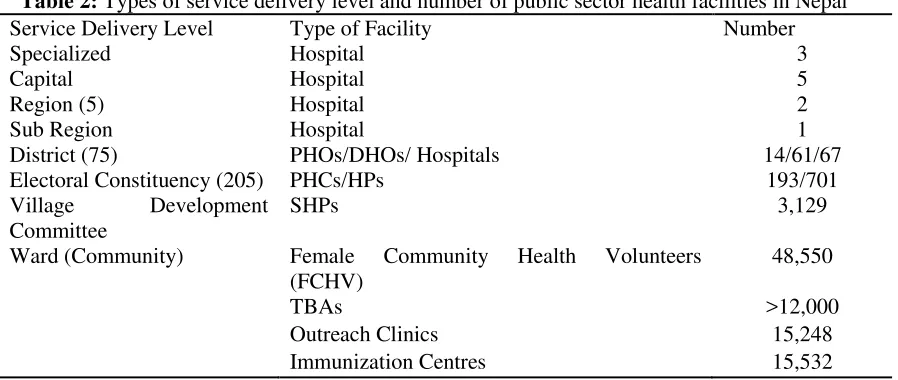
community-based health activities and as a referral point for patients to HPs and PHCs, and district, zonal and regional hospitals, and finally to the specialty tertiary care centres in Kathmandu. The referral system was designed to ensure that the majority of population has access to public health care facilities and affordable treatment. Public health facilities face constant resource constraints, poor facilities management, planning, and poorly trained staff. There is one health committee in each VDC. Recently the VDC health committee is made responsible to run the sub-health post within the VDC. The number and types of health facilities with regards to the service delivery level and the three ecological zones are demonstrated in Tables 2 and 3.
Table 2: Types of service delivery level and number of public sector health facilities in Nepal
Service Delivery Level Type of Facility Number
Specialized Hospital 3
Capital Hospital 5
Region (5) Hospital 2
Sub Region Hospital 1
District (75) PHOs/DHOs/ Hospitals 14/61/67
Electoral Constituency (205) PHCs/HPs 193/701
Village Development
Committee
SHPs 3,129
Ward (Community) Female Community Health Volunteers
(FCHV)
48,550
TBAs >12,000
Outreach Clinics 15,248
Immunization Centres 15,532
Source: DHS Annual Report 2001-2002
Table 3: Topographic distribution of the health care facilities in Nepal
Type of institution Total Mountain Hill Terai
Hospital 85 16 45 24
PHCC/HC 193 20 94 79
Health Post 701 152 379 170
Sub-Health Post 3,129 387 1,606 1,136
Source: DHS Annual Report 2001-2002
III.1 Decentralization and Management of Health Facilities
The District Health Office/ District Public Health Office manage the public health program in the district through a network of Primary Health Care center, Health Post and Sub health post. It is important to highlight that in every Village Development Committee of Nepal, there is at least one health facility serving the catchments area. The Community level health facilities are managed by the Health Facility Management Committee chaired by the VDC president. According to the category of the health facility, the number of health staff is different.
21
epidemiological situation and intervention type. For example, in the malarious areas the services concentrate to identifying malaria cases early and treating them. At the community level the district public health network is supplemented by the network of Female Community Health Volunteers (At least 9 /VDC) and mothers group. The local health facility in partnership with community participation implements all the public health programs in the community.
III.2 Organizational Structure of Epidemiology and Disease Control Division
At the Central level, Epidemiology and Disease Control Division (EDCD) under the Department of Health Services is responsible for developing strategies, guidelines, plan and monitoring of the implementation of the vector borne diseases: Malaria, Kala-azar, Dengue, Chickunguniya, Filariasis and Japanese encephalitis. In addition to the Director EDCD, Disease Control Unit of the EDCD has six sanctioned posts: Malariologist (Sr. Health Administrator-1), Public Health Officer -1, Vector Control Inspectors-2, one medical officer and a health assistant.
At the regional level, there is a disease control sub-section under the public health section of RHD. This subsection is staffed with Vector Inspector1, Entomologist1, Asst. Entomologist -1, Vector Control Inspectors/Malaria Inspectors/Entomological technicians-4, Lab.boy--1, Laboratory technician-1, Laboratory assistants-2 and Maintenance technicians-2 based in each of the five regions.
At the district level, most of the malaria endemic districts are working under the leadership of a Public Health Officer, under which one Vector control inspector or malaria inspector or both along with laboratory technicians/assistants are available for control, diagnostic/surveillance activities. The control of the Vector Borne Diseases (VBDs) is the responsibility of the public health services staff in Primary Health Centers (PHCs), Health Posts (HPs) and Sub-health Posts (SHPs) at the peripheral level.
III.3 Malaria Control Program Staffing
The Epidemiology and Diseases Control Division (EDCD) is one of the divisions under the Department of Health Services. The division has three technical sections- Disaster Management, Epidemiology and Disease Control under the supervision of the Director.
The Disease Control Section has the responsibility for the control of vector-borne diseases such as Malaria, Kala-azar, Japanese encephalitis, lymphatic filariasis, etc. This section is staffed with one Health Administrator, one Public Health Officer and two Vector Control Inspectors.
22
At the district level, Malaria and Vector Borne Disease unit is staffed with a vector control inspector and or malaria inspector plus a laboratory technician / Laboratory Assistant, responsible for conducting disease prevention and control activities. GFATM supported districts (13+18) are also supported with an additional post of Monitoring & Evaluation officer with a graduate degree in Public Health mainly mandated to support DPHO in prevention, control and surveillance of Vector borne diseases including Malaria.
III.4. Vector Borne Disease Research and Training Centre (VBDRTC)
Vector Borne Disease Research and Training Centre (VBDRTC), located in Hetauda, about 150 KM south of Kathmandu, is a semi-autonomous institute under Ministry of Health & Population is an institute developed as a Research and Training Center with the mandates of performing research in vector borne disease prevention, control, diagnostics, therapeutic drug efficacy studies, entomology and vector control works closely with the DoHS/EDCD in training public health personnel in vector borne disease management, integrated vector management, malaria microscopy (Basic & Refresher), kala-azar elimination support and conducting field level operational researches on vector borne diseases. (For details see Annexes 10 and 11)
III.5 Public-Private Partnerships
The vision of a public private partnership was to create a sector in which the Ministry of Health and Population would gradually retreat from service delivery, making more use of public private partnerships to ensure services are delivered. In practice, Government has continued the most part to deliver the services that it finances, but has used PPP approaches where they offer clear advantages. The national malaria program has been delivering its interventions with close coordination with Population Service International (PSI)/Nepal, NGO’s, CBO’s, WHO and involvement of media houses, public and private academic institutions, private medical college & hospitals, Professionals associations, councils, as suitable and available.
III.6 Health Management Information system (HMIS)
Nepal has a functional and sensitive HMIS that produces a range of detailed service delivery information unrivalled in the region. The HMIS data is regularly compiled, reported, and reviewed at regional and national level. HMIS is working on introducing GIS, which in future could be useful in mapping the services and cases.
IV. MALARIA SITUATION ANALYSIS
IV.1 Epidemiology
23
Repetion. These 65 malaria endemic districts partially or wholly have been classified as 13 high risks, 18 moderate risks and 34 low risks. The distribution of Malaria within the district itself is not homogenous. No malaria cases have been reported from 10 mountain districts including the capital Kathmandu indicating no detectable level of transmission.
IV.1.1 Malaria species
Three parasite species namely Plasmodium vivax, Plasmodium falciparum and Plasmodium malariae has been detected in Nepal till date. However, Plasmodium ovale has also been reported from private sector health care providers from the patients returning from Africa. P. malariae has not been detected since last two decades. During the last 5 years, percentage of P. falciparum remained between 17-26% of the total confirmed malaria cases, where as P.vivax has remained the predominant species. In malaria outbreak areas P. falciparum is the dominant infection.
IV.1.2Malaria vectors
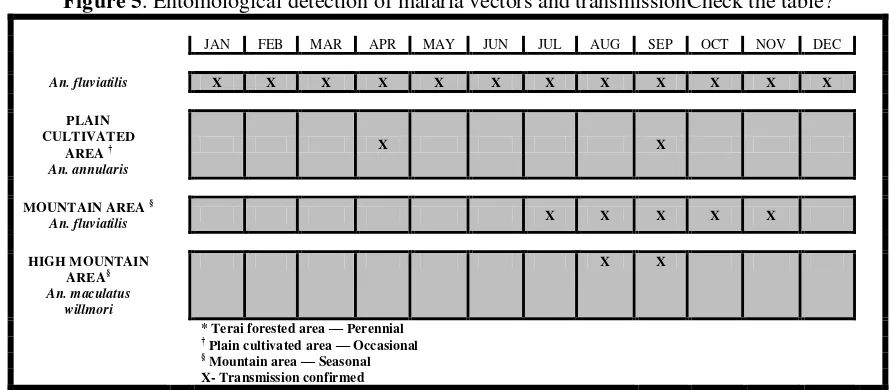
Mosquito fauna surveys done in 1968 have revealed presence of 42 Anopheles species in Nepal. Out of them, An. fluviatilis, An. maculatus, An. annularis are the vectors of malaria transmission in Nepal. An. minimus disappeared after continuous insecticide spraying during malaria eradication era. An. fluviatilis has been incriminated from the pre-eradication period and also responsible for the perennial transmission in forest fringe, foothills and inner terai. This species has been found responsible for the transmission during epidemics. An. maculatus supports to maintain the transmission in these areas. An. annularis is found in outer Terai, cultivated plains and is a weak vectordelete An. culicifacies is a suspected vector in Terai region ?.
Figure 5. Entomological detection of malaria vectors and transmissionCheck the table?
JAN FEB MAR APR MAY JUN JUL AUG SEP OCT NOV DEC
An. fluviatilis X X X X X X X X X X X X
PLAIN CULTIVATED
AREA †
An. annularis
X X
MOUNTAIN AREA §
An. fluviatilis X X X X X
HIGH MOUNTAIN AREA§
An. maculatus willmori
X X
* Terai forested area — Perennial
† Plain cultivated area — Occasional
§ Mountain area — Seasonal X- Transmission confirmed
24
Malaria in Nepal is unstable with 75% P. vivax and 25% P. falciparum. The biology of vivax malaria is poorly understood. Clinical vivax malaria cases not given 14 day Primaquine course may relapse. These vivax malaria cases are largely the cases treated by the non-health sector and self treatment. Relapses from these cases will remain a major threat for outbreaks. Since we are planning to proceed for elimination it would be advisable to protect the entire endemic population with LLINs or IRS.
Over the years, there is significant decrease in laboratory confirmed malaria cases and slide positivity rate. Malaria incidence in Nepal has decreased from 0.27 per 1000 in 2004 to 0.15 per 1000 in 2010 (Figure 9) detail data is provided in annex 2. delete. The slide positivity rate (SPR) has decreased from 3.08% in 2004 to 2.27% in 2010. The percent PF cases have more or less remained at the same level. In 2004, 65% were indigenous and 16% imported among total malaria cases reported. Imported (from India) cases are increasing gradually showing an increase up to 35.38% percent in 2010.
Population prevalence surveys conducted in Jhapa and Kanchanpur in 2008 indicated the parasite prevalence rates of 0.82% and 1.92%. There have been no outbreaks of malaria since 2006. Malaria deaths have remained less than 10 per year since 2002, whereas during the epidemic in Banke in 2006, 42 deaths were reported.
25
present malaria mortality is 0.01 per 100,000 populations.It may be noted that since the malaria incidence is very low the programme is planning to shift to total malaria cases in Nepal and not the API and relataed indices. case investigations and follow up would be introduced.
IV.1.3.1 Age and sex wise Distribution of Malaria Cases
Age wise distribution of malaria cases indicates that among the total malaria cases, 70% of cases were seen in the age group of 15 and above, while only 1% of the case were seen in infants. Sex wise distribution of malaria cases revealed that males are more affected than females (Figure 12).
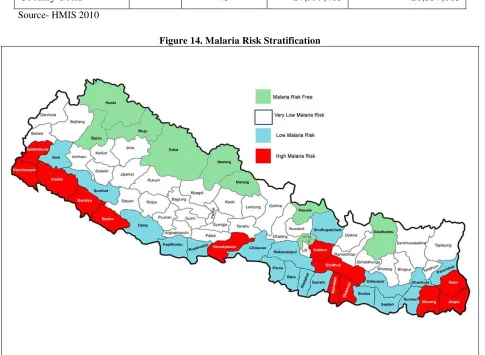
IV.2 Malaria Stratification and Mapping
26
Since 2004, with the introduction and scaling up of new interventions under GFATM supported program, the malaria endemic districts were further categorized into four categories according to API values as main determinant and vector prevalence as secondary determinant (Table 4), into four strata namely high risk, moderate risk, low risk and no risk.
Table 4. Malarious area stratification
Strata API
Value
Number of Districts
Total Population
Malaria-risk population
Stratum I (High risk)
>1 13 7,492,885 5,984,761
Stratum II (Moderate risk)
0.5-1 18 9,703,238 8,245,575
Stratum III (Low risk)
<0.5 34 8,670,360 6,126,677
Stratum IV
(No risk / malaria free)
- 10 2,132,922 0
Country Total 75 27,999,405 20,357,013
Source- HMIS 2010
27
According to the recommendation of JANS a table that illustrates the range of the API by VDC of 31 districts is provided in Annex 3.
IV.3 The Malaria Program Performance during last five years
IV.3.1 Entomology and Vector Control
IV.3.1.1 Entomology
Due to paucity of entomological staff a very few entomological studies have been carried out, however, a number of spot surveys and observations were carried out with GFATM support. delete
Because of the importance of entomology in malaria control permanent entomological teams should be appointed at the centre and regional level so that longitudinal entomological surveys can be carried out regularly to support the target vector control interventions. However, a number of susceptibility tests and bioassay tests have been carried out in past five years the result of which are included in the respective vector control operation chapter.
IV.3.1.2 Vector Control
IV.3.1.2.1 Indoor Residual Spraying (IRS)
Indoor residual spraying forms the mainstay of the vector control component. The objective of IRS is to ensure the safe and standardized application of the residual insecticide to indoor surfaces of all houses and animal shelters in selected target areas so as to obtain a marked reduction in mosquito density and consequently a sharp reduction of malaria cases.
During last five years synthetic pyrethroid insecticides viz., lambda cyhalothrin 10% WP at the rate of 25mg/sq. m; delta methrin 2.5%WP at the rate of 20mg/sq.m, and alpha cypermethrin 5%WP at the rate of 30mg/sq.m were sprayed in rotation.
Susceptibility tests using WHO test procedure showed that all anopheline were susceptible to delta methrin, per methrin, alpha cypermethrin and lambda cyhalothrin. The cost of insecticide used is US $10 per kg for alpha- cypermethrine and US $15 per kg for lambda-cyhalothrine. The first round (summer cycle) was undertaken in April/May and the second (autumn cycle) in July/August. The smallest unit for insecticidal spraying is a Village Development Committee (VDC). Criteria used for residual spraying were following:
a. High level of incidence of malaria with perennial and persistence of transmission b. High prevalence of P. falciparum and drug resistant foci
c. Malaria epidemics and focal outbreaks
d. Epidemic prone areas (due to high receptivity and vulnerability)
28
Annex-4. Maximum numbers of household covered was 116,856 in 2007 (612,409 population) where as minimum numbers of household covered were 21724 in 2004 (128,229 population). Average insecticide consumed per year was 13,051 kg and average cost per year was US $158,646 during this period. Household coverage by IRS is low in relation to the population at high risk.
IV.3.1.2.2 Long Lasting Insecticidal Nets (LLINs)
First lot of 40,605 LLINs was procured and distributed by EDCD in 2005. Thereafter, PSI an international private organization shared the responsibility of procurement and distribution of LLIN as PR2. WHOPES approved LLINs were procured and distributed. LLINs were distributed according to the existing LLIN distribution guidelines, developed by EDCD (one LLIN for 2 persons in a house, in VDCs in Stratum-I). In the beginning 56,167 LLINs were distributed through social marketing. Thereafter social marketing was stopped. LLIN campaign by PSI started in one third target VDCs per year in each district so as to cover the entire high risk VDCs by the end of 3rd year. Delivery of LLINs was supervised by EDCD and PSI jointly and distributed by national NGOs and other partners, and implemented by community-based organizations. Through this distribution system, 1,209,322 LLINs were distributed during 2006 to 2010. Nepal Government provided LLINs free of cost (supported by GFATM funds) to the people living in VDCs in high risk districts. LLINs were also provided free, through DPHO, to all pregnant women attending ANC clinics at the government facilities in targeted VDCs since 2008. A total of 73,905 LLINs were distributed by the DPHOs from 2008 to 2009.
Based on the LLIN distribution data, LLIN coverage has increased since 2006 (Figure 15) please also refer to annex 6.
The impact of LLINs on malaria transmission is shown in figure No.16. There is significant improvement in malaria situation in villages under the LLIN program.
29
30
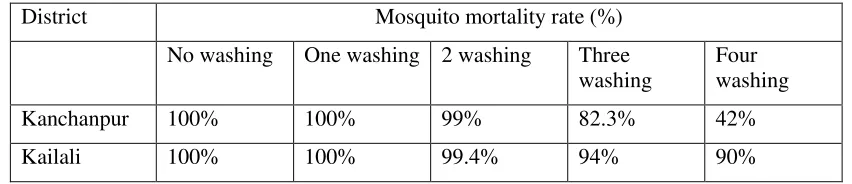
Table 5: The table should also provide the years since they were procured. The text should be written accordinglyResults of bio-assay test on LLIN 2008
District Mosquito mortality rate (%)
No washing One washing 2 washing Three
washing
Four washing
Kanchanpur 100% 100% 99% 82.3% 42%
Kailali 100% 100% 99.4% 94% 90%
IV.3.2 Early Diagnosis and Prompt Treatment
Malaria diagnosis and treatment is available free of cost in Govt. health facilities. Microscopy & / RDT based malaria diagnostic facility is available at district and up to Primary Health Care Center; some of the health posts in malaria endemic areas have also started laboratory based diagnostic facilities for malaria with local govt. support. In malaria endemic areas, where there is no microscopy facility, RDTs are made available for the diagnosis. In the past only P. falciparum specific RDTs were provided to P. falciparum prevalent health facilities but recently Combo RDTs detecting both vivax and falciparum are made available. Adequate supply of microscopy slides, reagents, RDT, ACT and Quinine has been managed in all health facilities, supported by a logistics management system and stock outs are minimal.
31
Table 6. Number of suspected cases examined and positive cases detected in different malaria risk areas
Malaria
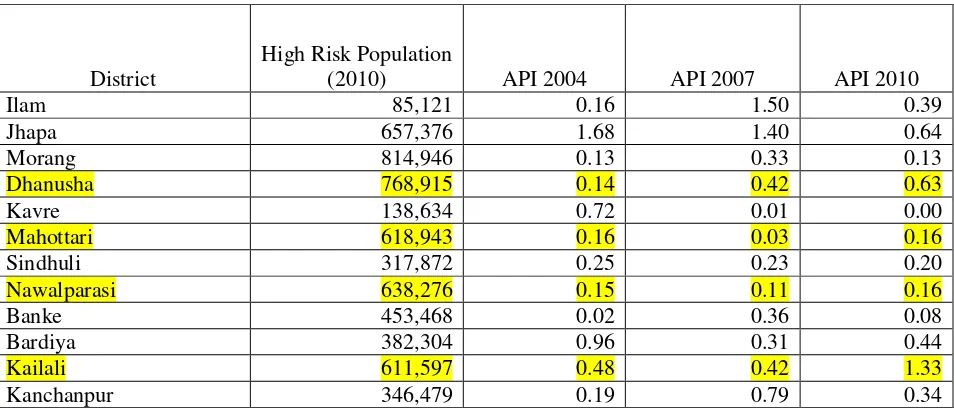
Malaria cases have substantially decreased and came down to zero in one of the district, kavre, which was highly endemic earlier. However, another endemic district Kailali on the other hand, there is fourfold increase in number of cases (Table-7). This is under investigation. Some districts like Nawalparasi, Dhanusha and Mahottari cases has shown increasing trend of malaria (Table 7). Other high risk districts have managed to maintain API below 1/1000 (Table-7). However, malaria still remains a public health problem in Kailali, Nawalparasi, Dhanusha and Mahottari districts. The high malaria risk areas still have been reporting 83% of total malaria and 92% of the total P. falciparum cases of the country (Annex 6). All deaths due to malaria were reported from these areas. An intensive malaria control efforts should be made in these areas to reduce the overall malaria burden of the country.
Table 7. Annual Malaria Incidence in high risk areas, 2004, 2007 and 2010 Please give data for all the years
District
High Risk Population
(2010) API 2004 API 2007 API 2010
Ilam 85,121 0.16 1.50 0.39
32
Please obtain bivalent quality RDTs. Read the paper on the subject. There is a great need of coordination between public health and private health facilities in order to diagnose and treat all the malaria cases according to National Protocol.
At community level FCHVs are expected to refer all suspected malaria cases to a health facility for confirmation and appropriate treatment. In remote areas they have been involved in treating the clinically suspected malaria cases, in absence of malaria microscopy / RDT facility.
Uncomplicated P. falciparum cases are treated with ACT (artemether/lumefantrine) for three days. Similarly, P. vivax cases are treated with chloroquine for three days and primaquine for five days. Recent policy change recommends treatment of P. vivax with chloroquine for 3 days followed by radical treatment for 14 days with primaquine. Similarly, P. falciparum cases are also given a single dose treatment of primaquine along with ACT. Where there is no laboratory services the suspected cases are treated with chloroquine only for three days. According to the health facility survey carried out in 2006, 70% uncomplicated laboratory confirmed malaria cases were treated with anti-malarials as per National Malaria Treatment Protocol. In recent years no health facility survey were carried out to determine the treatment coverage. In future regular annual health facility surveys shall be carried out to determine the proportion of malaria cases treated.
Quality control of diagnosis and treatment
It is of utmost importance that the quality of diagnosis and treatment of malaria cases be ensured which requires qualified and trained human resource in laboratory techniques, along with validated/calibrated equipments, quality assured diagnostics and drugs. There has been slackness in cross checking of the slides in the recent past, due to any unforeseeable reason. Country have not yet started quality assurance program for assuring the quality of malaria diagnostic services, impacting quality of diagnosis and treatment. There is an urgent need to strengthen the capacity of laboratory technicians in malaria microscopy through training, providing standard validated equipments & health products, regular time bound monitoring and supportive supervision by the experts, introduction of malaria microscopy quality assurance program.
Drug resistance monitoring
During last five years, four drug resistance monitoring trials have been undertaken as follows:
The sentinel sites Shanischare (Jhapa) and Dhalkebar (Dhanusha) under the guidance and supervision of EDCD, similarly,
The sentinel sites in Chisapani (Dhanusha) and Malakheti (Kailali) were undertaken under the guidance and supervision of VBDRTC.
33
IV.3.3 Surveillance and Epidemic Preparedness
Records of the EDCD show a satisfactory reporting system through weekly Early Warning and Reporting System (EWARS), Weekly Community Sentinel Surveillance for outbreak and monthly HMIS. Monthly HMIS gives comprehensive data for malaria indicators which are being used by EDCD since 1996. The EWARS provides weekly information on admitted malaria cases and deaths from 40 out of 85 hospitals. It also generates immediate reports (within 24 hours) for severe malaria cases. Community sentinel sites for epidemic outbreak control were established in 2009 in thirteen districts, each having two sites at PHC Centre level. Weekly reports are sent to district HMIS and monthly reports to the central level HMIS and EDCD. Essential information for epidemiology and surveillance such as: yearly data, monthly data, laboratory confirmed cases as well as clinical malaria cases, species-wise information, classification of cases according to origin of infection (indigenous, imported) is available at different levels of health services. Besides the monthly reports, quarterly and annual reports are also prepared at EDCD for performance review. FCHVs are being trained to detect fever cases among migrants in the community and refer the fever cases to the nearest health facility.
Computers with access to internet at DPHO offices and PHCC level, and telephone connection up to HP level facilitate the reporting system. Annual TRaC survey for LLIN coverage and utilization has been conducted by independent research group since 2006 on yearly basis. For record keeping at different level following register are maintained- laboratory register, malaria register, community sentinel surveillance register for epidemic outbreak control etc. Good register keeping system is not up to the mark in some of the health facilities. VDC wise mapping of malaria risk, LLIN distribution and microscopy facility are in place at the district public health offices.
HMIS does not cover unsecured areas and private sector health care. HMIS reports sometimes are not complete and timely. There is no regular data verification mechanism at district level. The annual health facility and community-based surveys for assessing coverage of outcome indicators in relation to diagnosis and treatment and vector control are in place. Population based malaria prevalence surveys are carried out time to time to compare with the regular surveillance data.
The current data collection, collation and reporting system requires strengthening to achieve the target of timely, accurately reporting and timely and appropriately responding the outbreaks and case based surveillance and identification of malaria foci in order to eliminate the indigenous malaria foci requires an analysis of current reporting system and comprehensive strengthening.
IV.3.4 Behavior change communication (BCC)
34
media and messages, planning, implementing and evaluating health education and health promotion activities at all levels. IEC/BCC activities are undertaken jointly by 5 regional health offices and district health education technicians. Health education technician functions as the focal point for all IEC/BCC activities in the district. At the VDC level FCHVs play an active role in IEC, LLIN survey and distribution.
EDCD has been supported by PSI, an important partner of malaria program, on IEC/BCC component in collaboration with NHEICC. Available data on knowledge and practices on malaria treatment and prevention in both rural and urban areas reflect achievements of the IEC/BCC. Radio (normal and FM) was found to be most powerful means of information in both rural and urban areas. IEC/BCC materials, malaria bill boards have been developed and hanged, which have played important role in improving community awareness in malaria. Although FCHVs have been reported playing active role on IEC, the availability of IEC materials is crucial. In some areas, basic knowledge on malaria, regarding mosquito breeding sites and biting habits in the community is still inadequate. Self-medication by malaria patient should be discouraged and private service providers should be encouraged to follow national treatment protocol, hence the greater emphasis on IEC/BBC materials is crucial.
IV.3.5 Program Management
IV.3.5.1 Human Resources
Human resource management has improved since 2004, but challenges still remain. A study carried out in 2006 by the Ministry showed that 76% of health personnel posts were filled in comparison to sanctioned posts. The main problem of human resources is deployment and retention of physicians, nurses and other basic health services staff in peripheral health facilities. There is problem of continuation of vector control staffs at the district level, i.e. the post of Vector Control Inspectors and Malaria Inspectors post are going to be abolished after their retirement from the government service. Monitoring and Evaluation Officers are working on yearly contractual basis and through GFATM support. There is an urgent need to make provision for key posts: Entomologist, Microbiologist, Epidemiologist and / Medical Officer, Monitoring and Evaluation Officer in disease control section of EDCD; Similarly, positions of Monitoring and Evaluation Officers at the regional and district level is crucial at least in malaria endemic districts.
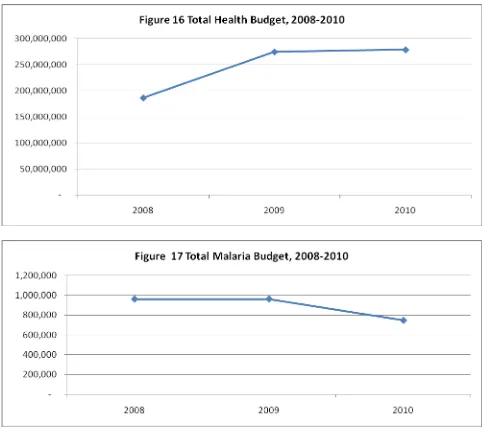
IV.3.5.2 Budget, Finance and Audit
Budget: Ministry of Finance prepares annual budget for the Govt. of Nepal, which is approved
35
diagnosis, trainings, LLINS and BCC activities. WHO has been providing technical support for guidelines/protocols development and capacity building of human resources.
Figure 16 and 17 indicate that during the last three years, health budget is increasing trend where as the malaria program budget show a slight decrease in 2010 due to unavailability of of some of the GFATM funds as grant negotiations were going on and could not be allocated to 2010 funds. GFATM has supported many activities which were also earlier under Govt. fund support. I think this para should be re-written or deleted with figures as it would be counterproductive
36
Financial management: Financial management of the malaria program is maintained as per the
guidelines of the office of the Financial Comptroller General (FCGO). FCGO releases the fund, perform internal audit, give direction and prepare accounts of central incomes and expenditures of the program. FCGO provides authority to DoHS/EDCD, RHD, DoHS (EDCD) through MoHP to operate financial transaction. During last three years, budget utilization by malaria program had remained in the rage of 75% to 90%.
Audit:
Government of Nepal follows internationally recognized both internal and external audit
system through its independent body. Office of the Financial Comptroller General (FCGO) is the main body to conduct
regular "internal audit" on periodical (trimester) basis. The internal audit of the revenue earned by the office shall have to be made by the concerned Funds and Accounts Comptroller Office in such a manner as prescribed by the Office of the Financial Comptroller General.
Office of Auditor General (AOG) is responsible to perform external audit in all
government offices where government, donor funded projects, and other means of sources have been operated. The audit is done on annual basis and the report of the audit is presented in the assembly for public notice and necessary action, through the president's office.
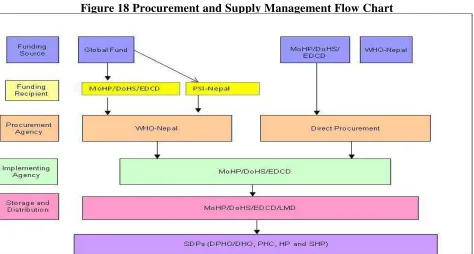
IV.3.5.3Physical Assets Management and Procurement of Goods
37
Figure 18 Procurement and Supply Management Flow Chart
38
IV.4 SWOT analysis
IV.4.1 SWOT Analysis (Vector Control)
Internal Factor External Factor
Strength Opportunities
Government commitment to malaria vector control program and sustainability of IRS; government budget has been sufficient for IRS insecticide and some equipment.
Well established and functioning vector control program at national, regional and district levels.
Vector control guidelines and training manuals are in place.
As LLIN and IRS are not sustainable during a long term period, so a
comprehensive integrated vector management (IVM strategy) can be developed and adopted as there is a government commitment to support and scale up national malaria control
interventions.
Availability of donor funding to scale up vector control
Weakness Threats
Absence of regular entomological studies and surveys often poses problem to plan suitable interventions.
Strategic plan 2007-2011 targets 80% of people in high risk areas sleeping under LLIN (last night) by 2011, however data over five years shows low coverage by IRS and LLIN (LLIN coverage 38% and IRS coverage around 8% of risk
population)
Quality of IRS compromised due to poor direct supervision.
Coverage of second cycle of IRS (July-August) is less every year.
Currently used insecticide has short duration residual effect (up to 12 weeks) of action.
No activity on larviciding and reduction of breeding sites.
Some malaria endemic regions lack in entomology, epidemiology and vector control skills.
Lack of means of transportation (bicycles, motor cycles, vehicles) hampers
supervision in checking the quality of spraying operations.
Absence of entomological teams and longitudinal entomological studies hamper the planning of vector control operations.
Natural disasters like floods are risk factors for vector control interventions from the point of accessibility.
39 IV.4.2 SWOT Analysis (Diagnosis and Treatment)
Internal Factor External factor
Strength Opportunities
Policy and guidelines on malaria case management available.
Availability of antimalarial medicines in almost all health facilities and grass root level.
Majority of health workers have received training on case management.
Laboratory has internal quality control systems in place.
National treatment protocol adopted after incorporating reports of the drug resistance studies.
The treatment protocol is being updated emphasizing on treatment of confirmed cases with radical treatment for both vivax and falciparum malaria.
High quality RDTs available at
international market that can be procured from the EDCD budget or global fund grant.
Available GFATM fund could be utilized in strengthening and lab capacity and introducing quality assurance system for malaria diagnosis and treatment.
Weakness Threats
Microscopy is limited to district health offices and some PHCCs only
RDT not available in all health facilities
Limited skills in the use of RDT by health workers
Quality control is not being carried out in some of the regional laboratories.
Treatment of RDT negatives and clinically diagnosed cases is a common practice
Inadequate IEC on case management.
There is set back in using primaqune in radical treatment of Pv due to unknown status of G6PD deficiency.
Some private institution and academic institutions are not strictly following national treatment protocol.
Treatment protocols are not available in some of the public health facilities as well.
Results of current drug resistance monitoring studies are not validated yet.
High staff turnover