Sealant Using Noninvasive And Invasive Techniques-A SEM And
Microleakage Study
HERLE G Pa, JOSEPH Tb, VARMA BC
, JAYANTHI Md
ABSTRACT
The efficacy of using invasive and non invasive techniques was assessed by Scanning electron microscopy, and by microleakage of Glass ionomer (GC VII, Fuji) and Resin based sealant ( Helioseal-F, Ivoclar Vivadent). 100 young premolars were used for this study, and they were divided into four groups : Group I: non-invasive technique GC VII, Group II: Invasive GC VII, Group III: Non-Invasive Helioseal -F, Group IV: Invasive, Helioseal-F. 5 teeth from each group were evaluated under SEM. It was seen that the flow and adaptation of GC VII was slightly better than Helioseal F, and the invasive technique provided the best flow and adaptation. For microleakage analysis 5% methylene blue was used. It was seen that minimal microleakage was seen in Group IV (P<0.01). Considering the recent controversies using resin based sealants, it can be said that GC VII can be a viable alternative for pit and fissure sealants
Key Words
GC VII, Glass lonomers, Helioseal-F, Invasive technique, Non-Invasive Technique, Pit and Fissure Sealants, Scanning Electron Microscop.
INTRODUCTION
Occlusal surfaces of molars are highly susceptible to dental decay. Hunter noticed a higher frequency of decay in pits and fissures of permanent molars1. Over the past several decades a considerable reduction in caries experience has occurred in the pediatric and adolescent population in the developed countries. Smooth surfaces and especially interproximal surfaces have benefited to the greatest extent from the caries preventive effects of various fluoride agents, but caries in pits and fissures remains a major problem.
Pit and fissure sealants are one of the best methods of preventing caries. It occludes the fissures and the pits from the accumulation of plaque and the cariogenic microflora. But caries still occurs in pits and fissures with sealant loss, and in adjacent pits and fissures or along cuspal inclines which were not initially sealed.
Fluoride containing Resin based materials are used as
a. Post graduate student, b. Professor and Head , c. Professor, d. Reader. Department of Pedodontics and Preventive Dentistry, Ragas Dental College and Hospital, Uthandi, Chennai.
sealants but Glass ionomer cement is an alternative material which can also be used as a sealant.
The penetration of sealant material into the fissures is limited by their morphology. Although fissures may penetrate deeply into the tooth, they may exhibit constrictions and variations in depth. There may also be differences in fissure morphology between the teeth. Furthermore, the deepest parts of the fissures are usually filled with organic debris including bacteria. Abrasive cleaning of the tooth surfaces in prophylaxis followed by etching removes organic materials and cleans the surface of the teeth, but does not penetrate below the visible orifice of the fissure. Thus, although the sealant may fill quite deep fissures under the best conditions, bonding to the clean enamel surface is usually confined to the inclined planes of the fissure and the contents of the fissure within the body of the tooth are sealed in2.
Before sealing it is difficult to assess and conclusively say whether caries has already been initiated in the base of the fissure. Hence, there is always a likelihood that bacteria might be sealed within the fissure, and caries formation maybe initiated below this sealed fissure3. An invasive fissure sealing technique with fissure preparation has been described and was reported to have better retention and diagnostic advantages. In this invasive protocol, preparation could also serve to ascertain whether dentinal caries is present.
Not much work has been done on evaluation of the invasive and non-invasive techniques in the manner they affect adaptability of sealants. Also, with the introduction of new fissure sealant materials, it is necessary to re-examine the physical characteristics and technique of fissure sealants. This study focuses on two fluoride releasing materials, the first being a newly introduced Glass ionomer (GC VII, Fuji) and the second being a resin based Fluoride releasing sealant (Helioseal -F, Ivoclar Vivadent)
The purpose of this study was to determine, using invasive and noninvasive techniques:
1. The amount of flow and adaptation of GC VII and Helioseal - F using SEM
2. Microleakage of GC VII and Helioseal-F
MATERIALS AND METHOD
This study was carried out in the Department of Pedodontics and Preventive Dentistry, Ragas Dental College and Hospital, Chennai and in collaboration with Indira Gandhi Centre for Atomic Research, Kalpakkam. The teeth used for the study were 100 Premolars extracted for orthodontic reasons. They were stored in saline immediately after extraction and used in the study within 30 days.
First, the surface debridement was done with ultrasonic seal-ers to make the specimens ready for use. They were then cleaned with slow speed micromotor handpiece with polish-ing brush to cleanse the fissures. No pumice was used as an abrasive along with the polishing brush. The teeth were stored at room temperature in saline.
The 100 premolars were divided into 4 groups of 25 teeth each.
The teeth in group I were conditioned using GC dentine conditioner for 20 seconds. The surface was then washed thoroughly with water for 20 seconds. Then they were dried by blotting with a cotton pellet or gently blowing with an air syringe, over-drying was avoided. The prepared surfaces appeared moist (glistening). The cement was mixed according to manufacturers instructions. A thin film of Fuji VII was applied over the occlusal surface with a microbrush and Light cured for 30seconds. Varnish was applied immediately after curing. The samples were placed in saline.
For group II, the fissures of the teeth requiring sealing were opened up with a diamond tapering fissure bur (0.5mm) in a low speed handpiece. Width of fissure preparation was equivalent to the diameter of the bur at 1.5mm mark from the tip of the bur. This was equivalent to 0.5-0.6mm. Material was placed as in Group I.
For group III the teeth were etched with 37% phosphoric acid for 20 seconds. The teeth were then rinsed thoroughly with water. The fissure was air-dried completely with oil free and moisture free air using a chip blower. Using the syringe needle tip, Helioseal F sealant was flowed into the fissures. It was
allowed to flow into the fissures for 20 seconds. The sealant was then light cured for 30seconds.
The Fissures of teeth in group IV were prepared as in Group II and Helioseal was applied as in group III. The teeth were stored in saline for 1 week at 37°C. After 1 week the teeth were thermocycled at 5°C, 37°C and 55° for 250 cycles, with a dwell time of 30s. They were then stored at 37°C for one more week. After 1 week of placing the teeth in saline, 5 teeth from each group were taken for SEM study. The teeth were sectioned longitudinally through the fissure using diamond disc with water coolant. Before SEM study the teeth were dried completely by keeping it exposed to the environment for 1 day and then keeping it under a mild heat source for 30 min, to remove the remaining moisture.
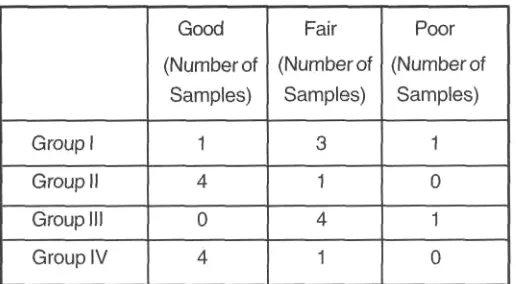
These sections were mounted on aluminum stubs with silver paint and sputter coated with gold-palladium, then examined with a Philips scanning electron microscope using an acceleration voltage of 15Kv. The structure analyzed was the complete fissure. To standardize the microscopic observations, micrographs of the fissures were taken at magnification of 50x. SEM examination was conducted to determine the amount of flow to the base of the fissure and adaptation to the walls. They were then scored as follows :
Scores give to evaluate the flow and adaptation
1 = good→ complete adaptation and penetration to all
fis-sures
2= fair→ one minor failure of adaptation or penetration
3= poor→ major failure of adaptation or penetration
The samples were then prepared for microleakage study, 20 teeth from each group were obtained. All the teeth were coated with nail varnish except 1 mm around the sealant. The apices of the teeth were sealed with sticky wax. The teeth were then immersed in 5% methylene blue solution for 4 hrs & then sectioned with a diamond disc and examined under stereobinocular microscope for microleakage.
They were scored depending upon the leakage levels 0= No dye penetration
1 = Dye penetration restricted to the outer half of the
seal-ant
2- Dye penetration to the inner half of the sealant
3= Dye penetration into the underlying fissure
RESULTS
Evaluation of flow and adaptation using Scanning electron Microscope
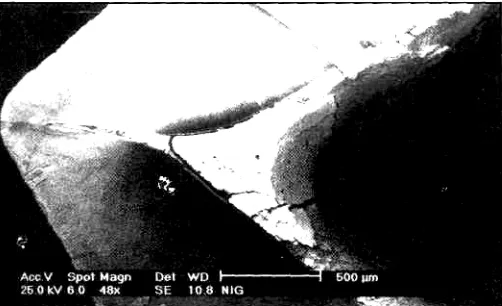
Five teeth from each group were evaluated for flow and adaptation using scanning electron microscope. Scanning electron microscope study revealed that all the groups showed some degree of flow and adaptation failure. In the group I and group II (GC VII, invasive and noninvasive) it was seen that all the specimens showed a cohesive failure. Even though a considerable gap was seen, there was still some amount of the sealant attached to the tooth. So all the samples showing thin layer of material on the tooth was considered as good adaptation. The invasive technique of both the materials showed good flow and adaptation, with 80% of samples giving a score of 1 (good). (Table 1, Fig 2,4) Group III (noninvasive Helioseal-F) showed poor scores i.e. 4 samples being fair and 1 sample being poor. Even though comparable scores were awarded to group I and group III (Fig 1,3), it was seen that there was much better flow into the depth of the fissure in group I (GC VII, Non invasive). In all the non-invasive groups it was seen that a presence of plaque and debris deep in the fissures
Evaluation of Microleakage
Twenty teeth from each group were evaluated for microleakage using stereomicroscope. It was found that 50% of the samples showed microleakage. In some samples the dye had penetrated through the material rather than the sealant tooth interface. In those cases, the amount of dye concentrated near the interface was taken into consideration and not the depth of the dye flowed through the material. Table 2 shows the statistical analysis using Pearson Chi-Square test which shows the count and the percentage of the microleakage level. The p value obtained was 0.003 which is significant, (p <0.01). Score 3, i.e. dye penetration to the depth of the fissures, was recorded in none of the samples. GC VII showed the maximum microleakage, of which invasive technique faired little better than the non-invasive technique. Helioseal-F showed the least microleakage, with invasive technique fairing little better than the non-invasive technique.
DISCUSSION
Surfaces with pits and fissures continue to provide a challenge
to caries prevention and account for the majority of the caries experience in children and adolescents.
Taking into consideration a developing country like India, the preventive measures towards oral health are imperative. Even if the initial cost of preventive measures like sealants may be higher than the cost of restorative materials like dental amalgam, in the long term sealants or any other preventive measure would be more cost effective as the tooth would be maintained in a state of health. For variety of reasons fissure sealants have not been widely accepted by the dental profession, despite over whelming evidence in support of caries prevention potential. The main problem encountered is towards microleakage leading to deterioration of the material and increased possibility of development of caries. Glass ionomer sealants have been shown to be retained in 73% of primary teeth and 78% of permanent teeth at 12 months and in 58% of permanent teeth at 24 months. Despite the lack of clinical detection of glass ionomer materials, replica studies have shown that the material was maintained within the depths of pits and fissures in 93% of cases thereby affording caries protection4.
In this study two fluoride releasing sealants were used. The first being a newly marketed Glass Ionomer Cement -Fuji VII (Fuji,GC), and the second being the tried and tested resin based fluoride releasing sealant Helioseal-F (Ivoclar Vivadent) which contains 20% fluorosilicate glass. Fuji VII has a pink shade when set and this contrast from the tooth structure, thus enabling inspection for sealant retention. Another feature of Fuji VII is the "Command Set" property of the material. After application of the material into the fissure, the setting reaction time can be reduced by 30% by light-curing (Halogen Curing Light). Unique feature regarding this material is the absence of any resin component in the material to hasten the setting reaction. It speeds up curing by absorbing the heat
MICRO GROU Cross tabluation
energy from the light. Another major advantage of using GC VII over other Glass ionomer materials is the fluoride release by the sealant which is considered to be the highest among
all Glass ionomers. Although sealant shows excellent efficacy, some dentists doubt its effects and durability and they fear sealing of carious lesions. Simonsen and Stallard's invasive placement technique (preventive resin restoration) not only provides higher retention rates of sealant but also
gives dentists more self confidence during its manipulation, especially where clinical evaluation of caries is difficult5. However, one of the prime factors governing the efficacy and life expectancy of a sealant is the marginal adaptability. Many studies reported a better efficiency of sealant when using the invasive technique. This occurs because the invasive technique widens and deepens the pits and fissures, eliminates organic material and plaque and exposes a more reactive tooth enamel, therefore enabling a thicker layer of sealant.6
In the present study, a single investigator did the preparation of the samples and evaluation was undertaken with the help of a supervisor to reduce the chances of error and avoid any bias. The use of scanning electron microscopy provides a means of direct visual observation of the adaptation of restorative materials to cavity margins, because of its magnification and depth of focus. Scanning electron microscopy specimens were scored as good, fair or poor depending upon the flow and adaptation of the sealant. This scoring technique was used by Robert Cooley et al7.
In the present study it was seen that the invasive technique showed better flow and adaptation to the fissures when compared with the noninvasive technique. But in the non invasive technique it was seen that all the samples did not flow deep into the fissure even though there was good adaptation to the walls. This result correlates to the study done by Jean Jasmin et al9 and Robert Cooley et al7 wherein, the sealant penetrated deep into the fissures, they did not consistently reach the bottom of the fissures. All the specimens in their study showed bubbles and gaps of different sizes and shapes in the base of the fissures. Fuji VII flowed deeper into the fissures when compared to Helioseal-F. This was similar to the results seen by Smales et al where in there was better flow and penetration of glass ionomer in the depth of the fissure, relative to resin based materials. In the present study it was seen that though there was a cohesive failure seen in all the glass ionomer sealant and detachment of the sealant
left a continuous layer of sealant covering the fissure enamel. The fracture of the sealant above this layer and cracks in this layer presumably occurred as a result of low cohesive
strength and preparation fault, ie, forces applied to the tooth during cutting and desiccation before SEM observation. These findings are very similar to that described by Lucia Birkenfeld et al10 wherein cohesive failure of the glass ionomer and fracture of the material was seen in all the specimens.
Helioseal-F did not show any cohesive failure as the material is resin based and unlike glass ionomer, is less moisture sensitive. From the results, it could be seen that GC VII performed equally, if not, slightly better than Helioseal F. In group I and group III (non invasive technique) It was seen that the plaque and debris was still retained in the deep portions of the fissure. This proves that simple mechanical cleaning and acid etching is not sufficient for complete cleansing of the fissure. Hence, from this study it can be seen that invasive technique is a good method of improving the flow and adaptation of the sealant. Both GC VII and Helioseal-F has shown good flow and adaptation in the invasive technique as compared to the non-invasive technique. The use of organic dyes as tracers is the most common method of detecting leakage invitro, 5% methylene blue was used as the dye, and the specimens were placed in the dye for 4 hours7. There is a distinction between microleakage and the dye leakage by which it was measured. Microleakage strictly refers to the ingress of oral bacteria, which have an approximate diameter of 0-5µm. Therefore dye leakage tends to be a severe test of microleakage.
Microleakage was scored according to the level of leakage in the interface of the sealant. This method of scoring has been followed by Hatbovic Kofman et al11, Christina Zervou et al12. From the results it can be seen that there was significant difference among the groups (P<0.01), with Helioseal-Fand invasive technique, showing the best result among all the groups. All the groups showed some amount of microleakage. This finding is in accordance to those reported by Theodoridou-Pahini et al13 and Moore et al6 who stated that microleakage can be expected in all restorative materials. The most likely explanation for this is the thermal expansion co-efficient of the sealants are significantly
amount of disintegration of the sealant due to its solubility. Since glass ionomer sealant is hydrophilic it has the tendency to absorb the dye into the material and this could give a false positive result. Hence in this study dye leakage into the material was not taken into consideration, but the presence of the dye in the interface of the sealant and the tooth was taken into consideration. This methodology was also followed by Birkenfeld et al14. Since the dye is simulating the bacteria and its products, leakage into the glass ionomer material does not have much significance, as it gets neutralized by the fluoride in the material.
Recent concerns have been raised about the possibility that estrogenic chemicals, in particular bisphenol-A (BPA), might be leached out of dental resin sealants. The potential deleterious effects of BPA and its degradation products are well documented14. Considering the potential side effects of resin based sealants, glass ionomer sealants can be
considered as a viable alternative. Partially erupted permanent molars are prone to caries. Their location and gingival covering present difficulties in cleaning and consequently might lead these teeth to become carious before they are fully erupted. Effectiveness of sealant may be jeopardized by the difficulty in obtaining ideal isolation and management of the tissue during its application15. GC VII has great advantage that can be applied in areas of minimal isolation, unlike resin based sealants where strict isolation and dry field is of utmost importance.
From this study and considering the advantages just cited it can seen that GC VII can be considered as an alternative to resin based sealants. In recent years there has been an apprehension regarding the leakage of estrogenic compound BPA from the resin based sealants. So the quest of finding an alternative to these resin-based sealants is an ongoing challenge. The glass ionomers have been considered as an alternative, but they have always been looked down upon when they are used as pit and fissure sealants. This has been due to their poor physical properties.
Considering the fact that the fluoride release by GC VII is supposed to be 6 times the release of fluoride than any other glass ionomers, we can say that GC VII does show a promising future in the usage as pit and fissure sealant. Since this is an In-vitro study, an in-vivo study should be carried out to ascertain the longevity and cariostatic effect of GC VII. Also the studies in the innovation of restorative materials could aim
for a perfect material with a good flow and also one which is free from microleakage to enhance the clinical success of the material.
REFERENCES
1. Sol E., Espasa E., Boj J. R. and Canalda C: Effect of different
prophylaxis methods on sealant adhesion: J Clin Pediatr Dent
2000; 24(3): 211-214.
2. Dennis Smith and Ray Stewart: Pediartic Dentistry: Scientific
foundations and clinical practice. 1st edition: Mosby
publication: 660-698.
3. Pereira A. C, Verdonschot E. H. and Huysmans M. C. :
Cariesdetection methods: Can they aid decision making for
invasive sealant technique : Caries Res 2000 ; 35 : 83-89.
4. John Hicks and Catherine Flaitz: Occlusal caries formation in
vitro : Comparison of resin modified glass ionomer with
fluoride sealant: J Clin Pediatr Dent 2000 ; 24(4) : 309-314.
5. Marcos Augustodo Rego and Maria Amelia de Araujo: A 2 year
clinical evaluation of fluoride containing pit and fissure
sealants placed with an invasive technique: Quint Int 1996 ;
27(2) : 99-103.
6. Marcos Augusto Rego and Maria Amelia Araujo: Microleakage
evaluation of pit and fissure sealants done with different
procedures, materials and laser after invasive technique. J
Clin Pediatr Dent 1999 ; 24(1) : 63-68.
7. Robert Cooley and James McCourt : Evaluation of a fluoride
containing sealant by SEM, Microleakage and fluoride release
: Pediatr Dent 1990 ; 12(1): 38-42.
8. Dhar Vineet and Shoba Tandon : Comparative Evaluation of
marginal integrity of two new fissure sealants using invasive
and non - invasive techniques : A SEM study: J clin pediatr
Dent 2000: 24(4): 291-297.
9. Jean Jasmin, Hubert van Waes and Vijayaraghavan T. V. :
Scanning electron microscopy study of the fitting surface of
fissure sealants Pediatr Dent 1991 ; 13(6) : 370-372.
10. Lucia H Birkenfeld and Allan Schulman: Enhanced retention
of glass ionomer sealant by enamel etching: A microleakage
and Scanning electron microscopic study: Quint Int 1999 ; 30
(10) : 712-719.
11. Hatbovic Kofman, Butler S. A. and Sadek H.: Microleakage of
three sealants following conventional, bur, and air-abrasion
preparation of pits and fissures: Int J Pediatr Dent 2001 ;11
: 409-416.
12. Christina Zervou, Eileen H. Doherty, Athanasios Zavras and
fissure sealants in the presence of occlusal forces: J Clin
Pediatr Dent 2000 ; 24 (4) : 273-278.
13. Theodoridou-Pahini, Tolidis K. and Papadogiannis Y.:
Degree of microleakage of some pit and fissure sealants: An
in Vitro Study : Int J Pediatr Dent 1996 ; 6 : 173-176.
14. Lucia H. Birkenfeld and Allan Schulman: enhanced retention
of glass ionomer sealant by enamel etching: A microleakage
and Scanning electron microscopic study: Quint Int 1999; 30
(10): 712-719.
15. Laura M. Borem and Robert J. Feigal: Reducing
microleakage of sealants under salivary contamination:
Digital image analysis evaluation : Quint Int 1994 ; 25(4)
283-289.
Reprint Requests to : Dr. Thresiamma Joseph
Professor and Head
Department of Pedodontics and Preventive Dentistry Ragas Dental College and Hospital