INTERNATIONAL EDITORIAL ADVISORY BOARD 1. Dr Nuwadatta Subedi(In Charge) Dept of Forensic Med and
Toxicology College of Medical Sciences, Bharatpur, Nepal 2. Dr. Birendra Kumar Mandal(In charge) Forensic Medicine and
Toxicology, Chitwan Medical College, Bharatpur, Nepal
3. Dr. Sarathchandra Kodikara (Senior Lecturer) Forensic Medicine, Department of Forensic Medicine, Faculty of Medicine, University of Peradeniya,Sri Lanka
4. Prof. Elisabetta Bertol(Full Professor) Forensic Toxicology at the University of Florence, Italy
5. Babak Mostafazadeh (Associate Professor) Department of Forensic Medicine & Toxicology, Shahid Beheshti University of Medical Sciences, Tehran-Iran
6. Dr. Mokhtar Ahmed Alhrani (Specialist) Forensic Medicine & Clinical Toxicology, Director of Forensic Medicine Unit, Attorney General’s Oice, Sana’a, Yemen
7. Dr. Rahul Pathak (Lecturer) Forensic Science, Dept of Life Sciences Anglia Ruskin University, Cambridge, United Kingdom 8. Dr. Hareesh (Professor & Head) Forensic Medicine, Ayder Referral
Hospital,College of Health Sciences,Mekelle University, Mekelle Ethiopia East Africa
SCIENTIFIC COMMITTEE
1. Pradeep Bokariya (Assistant Professor) Anatomy Dept. Mahatma Gandhi Institute of Medical Sciences, Wardha, Maharashtra
2. Dr Anil Rahule (Associate Professor) Dept of Anatomy, Govt Medical College Nagpur
3. Dr Yadaiah Alugonda(Assistant Professor) Forensic Medicine, MNR Medical College, Hyderabad
4. Dr Vandana Mudda (Awati) (Associate Prof) Dept of FMT, M.R.Medical College,Gulbarga, Karnataka,
5. Dr. Lav Kesharwani (Asst.Prof.) School of Forensic Science, Sam Higginbottom Institute of Agriculture Technology & Sciences, Allahabad U.P,
6. Dr. NIshat Ahmed Sheikh (Associate Professor) Forensic Medicine, KIMS Narketpally, Andhra Pradesh
7. Dr K. Srinivasulu (Associate Professor) Dept of Forensic Medicine & Toxicology, Mediciti Institute of Medical sciences, Ghanpur, MEDCHAL Ranga Reddy. Dist.AP_501401.
8. Dr. Mukesh Sharma (Senior Scientiic Oicer) Physics Division, State Forensic Science Laboratory, Jaipur, Rajasthan
9. Dr. Amarantha Donna Ropmay (Associate Professor) NEIGRIHMS, Shillong
10. Dr Basappa S. Hugar (Associate Professor) Forensic Medicine, M.S. Ramaiah Medical College, Bangalore
11. Dr. Anu Sharma (Associate Prof) Dept of Anatomy, DMCH, Ludhiana (PB)
EDITOR
Prof. R K Sharma
Formerly at All India Institute of Medical Sciences, New Delhi E-mail: [email protected]
“Indian Journal of Forensic Medicine & Toxicology” is peer reviewed six monthly journal. It deals with Forensic Medicine, Forensic Science, Toxicology, DNA ingerprinting, sexual medicine and environment medicine. It has been assigned International standard serial No. p-0973-9122 and e- 0973-9130. The Journal has been assigned RNI No. DELENG/2008/21789. The journal is indexed with Index Copernicus (Poland) and is covered by EMBASE (Excerpta Medica Database). The journal is also abstracted in Chemical Abstracts (CAS) database (USA. The journal is also covered by EBSCO (USA) database. The Journal is now part of UGC, DST and CSIR Consortia. It is now ofical publication of Indian Association of Medico-Legal Experts (Regd.).
NATIONAL EDITORIAL ADVISORY BOARD
1. Prof. Shashidhar C Mestri (Professor) Forensic Medicine & Toxicology, Karpaga Vinayaga Institute of Medical Sciences, Palayanoor Kanchipuram Distric, Tamil Nadu
2. Dr. Madhuri Gawande(Professor) Department of Oral Pathology and Microbiology, Sharad Pawar Dental College, Sawangi, Wardha.
3. Dr. T.K.K. Naidu(Prof & Head) Dept of Forensic Medicine, Prathima Institute of Medical Sciences, Karimnagar, A.P.
4. Dr. Shalini Gupta(Head)Faculty of Dental Sciences, King George Medical University, Lucknow, Uttar Pradesh
5. Dr. Pratik Patel(Professor & Head) Forensic Medicine Dept, Smt NHL Mun Med College, Ahmedabad
6. Devinder Singh (Professor) Department of Zoology & Environmental Sciences, Punjabi University, Patiala
7. Dr. Pankaj Datta(Principal & Head) Department of Prosthodontics, Inderprasth Dental College & Hospital, Ghaziabad
8. Dr. Mahindra Nagar (Head) Department of Anatomy, University College of Medical Science & Guru Teg Bahadur Hospital, Delhi 9. Dr. D Harish (Professor & Head) Dept. Forensic Medicine &
Toxicology, Government Medical College & Hospital, Sector 32, Chandigarh
10. Dr. Dayanand G Gannur (Professor) Department of Forensic Medicine & Toxicology, Shri B M Patil Medical College, Hospital & Research centre, Bijapur-586101, Karnataka
11. Dr. Alok Kumar (Additional Professor & Head) Department of Forensic Medicine & Toxicology, UP Rural Institute of Medical Sciences and Research, Saifai, Etawah. -206130 (U.P.), India. 12. Prof. SK Dhattarwal, Forensic Medicine, PGIMS, Rohtak,
Haryana
13. Prof. N K Aggrawal (Head) Forensic Medicine, UCMS, Delhi 14. Dr. Virender Kumar Chhoker(Professor) Forensic Medicine and
Toxicology, Santosh Medical College, Ghaziabad, UP
Website: www.ijfmt.com Print-ISSN:0973-9122 Electronic - ISSn: 0973-9130
Frequency: Quarterly, © All Rights reserved The views and opinions expressed are of the authors and not of the Indian Journal of Forensic Medicine & Toxicology. Indian Journal of Forensic Medicine & Toxicology does not guarantee directly or indirectly the quality or eficacy of any products or service featured in the advertisement in the journal, which are purely commercial.
Editor
Dr. R.K. Sharma Institute of Medico-legal Publications 4th Floor, Statesman House Building, Barakhamba Road, Connaught Place, New Delhi-110 001 Printed, published and owned by
Dr. R.K. Sharma Institute of Medico-legal Publications 4th Floor, Statesman House Building, Barakhamba Road, Connaught Place, New Delhi-110 001 Published at
Institute of Medico-legal Publications 4th Floor, Statesman House Building, Barakhamba Road,
Contents
Volume 12, number 2 April-June 2018
I
Indian Journal of Forensic Medicine & toxicology
1. Socio-demographic Proile of Pattern of Solvent Abuse among Street Children in Bengaluru ... 01
Murali Mohan MC,Yadukul S,Satish KV
2. A Retrospective Analysis of Mandibular Fractures: An Autopsy Study - 2012-2016 ... 06
Ajay Kumar T S, Deepa C
3. Infection Control in Orthodontics: A Review ... 10
Mithun K, Ashith M V, Harshitha V, Valerie Anithra Pereira, Deesha Kumari
4. A Study on Demographical and Clinical Proile and the Outcome of Snake Bite Victims in a Rural
Tertiary Care Hospital ... 16 Shreedhara K C, Sidramappa Gouda
5. A Chemical Safety Intervention Program Designed to Reduce Occupational Exposure among Vector Control Operators in Bangkok, Thailand ... 21 Paitoon Ngammuk, Thanach Pojpisuthipong, Robert S. Chapman
6. The Efectiveness of the Schema Therapy with the Group Method on the Women with
Social Anxiety ... 28 Anahita Arbabi
7. A Prospective Study of Pattern of Skull Fractures and Intra-cranial Hemorrhages in Relation with Fatal
Head Injury Cases Brought for Autopsy of SSG Hospital, Vadodara ... 33 Hardik G Prajapati, Bhargav Oza, V R Patil
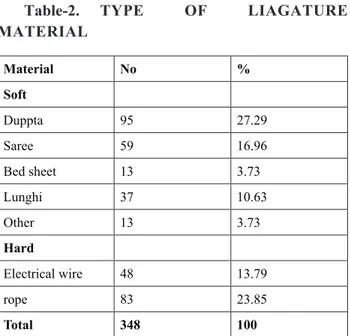
8. Study of Knot and Proile of Ligature Materials used in Asphyxial Deaths caused by Hanging in Kanpur; a Metropoliton City of India ... 38 Alok Arya, Alok Kumar, Puneet Awasthi, Rahul Sachan, Motoki Osawa, Archana Verma
9. Electrocution Deaths – A 6 Year Retrospective Study ... 44 Biradar Gururaj, B S Satish Babu, V Yogiraj,Pavanchand Shetty
10. Estimation of Stature from Head Length of Adults Belonging to Soligas- A Genetically Isolated Tribe from Southern India ... 48 Chandrakant M Kokatanur, Vinay R Hallikeri, K H Manjulabai
11. Study of Deaths due to Firearm Injuries in Tribal Region of Bastar ... 54 Pawan Tekade, Dhaval J Patel, Suwarna Chahankar, Prachi Parach
12. Naphthalene Poisoning – A Case Report ... 58 Sanjith Saseedharan, Suyash Kulkarni, Edwin Pathrose, Paritosh Baghel
13. Factors Inluencing Increasing Case Backlogs in Indian Judiciary: An Analysis ... 61
14. Diagnosis of Early Myocardial Infarction by Histochemical Staining of Heart on Autopsy ... 65 K Thunderchief, J Magendran
15. A Study on Prevalence of Pulmonary Thrombo Embolism in Bedridden Hospitalized
Deaths- Autopsy based Study ... 71 M Babu, Sushma Muchukota, Bijili Venkatesulu, K Mamatha, B Venkateswarlu
16. Demographic Proile of Unknown Dead Bodies in South Bangalore ... 76 Naveen Kumar T, Jagannatha S R, V T Venkatesha
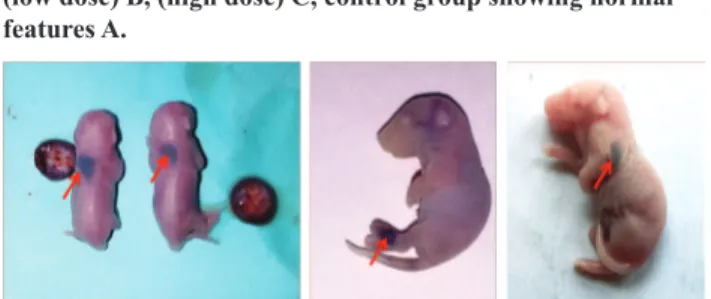
17. Teratological Study of Lamivudine in Swiss Albino Mice ... 80 Nidhi Sunhare, Anand Mishra
18. Accidental Fatality due to Explosion of Air Conditioner: A Rare Case Presentation ... 85 Vivek Kumar Mangare, Lal Chand Verma, Shiv Shankar Jat, R K Punia
19. To Determine the Elemental Distribution Pattren of Gunshot Residue from AK-47 &
Self Loading Rile ... 88 Vidyasagar Mishra, Sanjeev Koni, Pooja Ahuja, M S Dahiya
20. Socio-Demographic Proile of Fatal Cases of Fall from Height - SMS Hospital, Jaipur During the Year 2015-16 ... 93 Prem Chand Meena, Rakesh Kumar Punia
21. Study of Pattern of Cases on Alcoholism Recorded at GMERS Medical College and General Hospital, Vadodara ... 99 Uttam Solanki, Hitesh Rathod, Vijay Shah, Tejas Sailor
22. A Cross Sectional Postmortem Study on Closure of Skull Vault Sutures with Respect to Age from 3Rd to 6Th Decades of Life ... 102 Raj Kumar M G, Kiran J
23. Lanthanides Toxicity and their Involvement in Biological Activities ... 108 Rakesh Kumar Ray, Sushma Upadhyay, Sudhir K. Lamey, Sudhir Yadav
24. An Autopsy Record Study of Rheumatic Heart Disease ... 114
N S Kamakeri, Sunilkumar S Biradar, Smitha M, Mallikarjun K Biradar, Lohit Kumar
25. The Efect of Cold Stress on the Expression of Several Genes Associated with Cold Signal Transduction System Pathway in Cultivars of Canola (Brassica napus) ... 118 Mohsen Safaei, Habibollah Samizadeh Lahiji, Hassan Hassani Kumleh
26. A Study of Organophosphorus Poisoning in Rural Area of Mandya District in Karnataka ... 123 Shreedhara K C, Sidramappa Gouda
27. Toxic and Chemical Substances and Associated Legislations ... 126 Sushma Upadhyay, Rakesh Kumar Ray, Sudhir Yadav
28. A Comprehensive Analytical Study of Railway Fatalities in Twin Cities of Hyderabad
III
29. Variations in the Physico-Chemical Parameters of Thio-Barbiturate Derivatives ... 137
Rakesh Kumar Ray, Sushma Upadhyay, Sudhir Yadav,Sudhir N Limaye
30. Estimation of Age and Sex using Chest Radiograph – An Useful Tool in Identiication ... 141 Tarun Agarwal, B Suresh Kumar Shetty, Archith Boloor,Jagadish Rao PP,
Pavanchand Shetty H , M S Kotian
31. An epidemiological Study of Road Traic Accidents in B G Nagar, Mandya District ... 145 Shreedhara K C, Sidramappa Gouda
32. Evaluating the Efectiveness of Couple Therapy Training to the Consultants of Crisis Intervention Center of Welfare Organization in Improving the Quality of Couples’ Counseling Services (with Emphasis on Reducing the Tendency to Divorce) in Markazi Province ... 149 Kiiumars Farahbakhsh, Ahmad Khaki, Abdollah Moatamedy, Maasumeh Esmaaili, Hossien Salimi Bejestani
33. Correlative Study of Cranial Index with Diameter of Foramen Ovale in Maharashtra Population ... 155 Mohammed Abdul Mateen
34. A Study to Analyze the Impact of Hyoid Laryngeal Matrices on the Opinion of Manner of
Death in Asphyxia Cases ...159 Shreedhara K C, Sidramappa Gouda
35. Association of Barbiturates in Biological Activities as a Toxicological Agent ... 165 Rakesh Kumar Ray, Sushma Upadhyay, Sudhir N Limaye, Sudhir Yadav
36. Stature Estimation from Foot Measurements by Regression Equation in Males of
Bhavnagar - Gujarat ... 171 Tejas C Patel, Hardik Prajapati
37. Medico Legal Aspects in the Cases of Flame Burn Deaths ... 177 Sushma Upadhyay, Sudhir Yadav
38. Retrospective Record Study of Syphilis ... 182 N S Kamakeri, Sunilkumar S Biradar, Smitha M, Mallikarjun K Biradar
39. Does a Higher Educational Level Protect against Anxiety and Stress of Candidate Patients for Protective
Aggressive Procedures? ... 187 Shima Shaermoghadam, Hosien Shahdadi, Mina Taghi Abadi, Mehdi Afshari
40. Investigating the Efect of Using a Workshop based on Emergency Deterioration Index Instrument on the Performance of Nurses ... 193 Vahideh Poyesh, Sara Amanian, Mohammad Jahangiri, Mehran Hesaraki
41. Recognition of the Most Efective Components of Hospital Marketing in Iran ... 198 Mohammad Javad Akbarian Bafghi, Kazem Najai, Maryam Askaryzadeh Mahani,
Niloofar Zafarnia, Aliakbar Alinaghi Langari
43. Nutritional Status Assessment of Elder People based on MNA Tool ... 210 Fahimeh Khoushabi, Mohammad Parsi, Mohammad Reza Shadan, Somayeh Bagheri
44. The Efect of Adlerian Group Counseling on the Level of Assertiveness among Midwifery
Students in Clinical Setting ... 216 Fatemeh Tajabadi, Atefeh Ahmadi, Mansore Forouzi, Zhila Soltan Ahmadi, Younes Jahani,
Kazem Najai, Mohammad Javad Akbarian Bafghi
45. Palatal Rugae Pattern Identiication to Determine Family Lineage in Minangkabau, West Sumatera, Indonesia ... 222 Nila Kasuma, Dewi Elianora, Aida Fitriana, Fildzah Nurul Fajrin, Haria Fitri, Hilaire Tegnan
46. A Study to Explore Bullying and its Impact on the Psychosocial Wellbeing among High School Students of Udupi District, Karnataka ... 226 Reema Rai, Binil V, Savitha
47. Investigation of Anxiety of Patients Undergoing Coronary Angiography in Imam Hossein Hospital of
Mehran in 2016 ... 332 Masoumeh Shohani, Mosayeb Mozafari, Kourosh Sayehmiri, Monavar Hasanvand Amoozadeh
48. Attitude Towards Euthanasia among Students of Arts College – A Comparative Study ... 237 Khan F, Vaswani VR
49. Biological Rhythms, Sleep Quality and Postpartum Depression Disorder ... 242 Sajjad Basharpoor, Javad Drodi, Samaneh Valizade
50. Relationship of Fingerprint with Blood Group among Medical Students in Mangalore ... 248 Khan F, Badiadka KK, Vaswani VR
51. Protective Efect of Baicalin in Rats Exposed to Arsenic-Induced Testicular Toxicity ... 256
Abo Elyazied A Fouad, Amr A Fouad, Walid N Al-Melhim
52. Forensic Clinical Photography: A Game Changer in Medicolegal Investigation and
Forensic Science ... 262 Renjulal Yesodharan, Vishnu Renjith, Ashwini Kumar, Vinod C Nayak
53. Investigating the Efect of Self-Care Group Training on the Level of Resilience of Patients with Type 2
Diabetes ... 267 Shariati Abdolali, Alikhani Fatemeh, Haghighizadeh Mohammad Hosein, Elahi Nasrin
54. Morphology of Lip Print Patterns among Indian and Malaysian Population- A Tool for Racial and
Gender Identiication ... 272 Alister Joseph Thomas, Jagadish Rao Padubidri, Sowmya J Rao, Ravichandra Udupa,
B Suresh Kumar Shetty, Pavanchand Shetty H, Haneil L Dsouza
55. Pattern of Injuries Due to Road Traic Accidents Involving Motorized Two Wheeler Vehicles in Mangalore
Socio-demographic Proile of Pattern of Solvent Abuse
among Street Children in Bengaluru
Murali Mohan MC1,Yadukul s2,Satish KV3
1Assistant Professor, Department of Forensic Medicine & Toxicology, Sri Devaraj Urs Medical College, Kolar, 2Assistant Professor, Department of Forensic Medicine & Toxicology, Chamarajanagar Institute of Medical
Sciences, Chamarajanagar, 3Professor, Department of Forensic Medicine & Toxicology, Bangalore Medical
College & Research Institute, Bengaluru
ABSTRACT
Background: Solvent use among children and adolescents is a major concern across the world. Solvents are easily available, convenient to use, relatively inexpensive, and legal for certain uses; and all these factors promote their use and also abuse at later stages in youngsters.
Objectives:
a) To study the socio-demographic pattern of solvent abuse. b) To describe the patterns and consequences of solvent abuse.
c) To design a better preventive and rehabilitative approach to help these children.
Methodology: The present observational study was conducted in the Department of Forensic Medicine & Toxicology, Bangalore Medical College & Research Institute, Bengaluru during the study period of 2 years from 1st Aug 2010 till 31st Aug 2012. The study was done on the street children, who stay in the areas of Railway Station, Kalasipalya and Shivajinagar of Bangalore City; who were interviewed based on a predesigned proforma relating to solvent abuse and the data were analyzed.Totally 200 street children with history of solvent abuse were enrolled into the study.
Results: In the present study, Solvent abuse was common among male children in the age group of 13-15yrs. Majority of the children were coolie by occupation, started working by the age of 10 years& most of them took shelter on foot path. Tobacco was the most common other substance of abuse followed by Gutka, Alcohol & Ganja.
Conclusion: This study has identiied key issues requiring urgent public health action. The widespread use of solvents is particularly concerning due to easy, cheap availability and unrestricted sales to minors, as well as detrimental health efects of the same should be a major concern for law and policy makers. It is likely that the use of solvents could impact upon the ability of street children to be integrated into society and resume a normal social life.
Keywords: Solvent; Abuse; Streetchildren; Bengaluru
Corresponding author:
Dr. Yadukul s
Assistant Professor, Department of Forensic Medicine & Toxicology, Chamarajanagar Institute of Medical Sciences, Chamarajanagar, (+91 9986510681) Email: [email protected]
INTRODUCTION
Streets throughout the world are home to millions of children who endure hardships and injustices while struggling to survive1. The United Nations Children’s
of the street’,‘children on the street’ and ‘children from street families’2. Children on the street spend
a proportion of their time on the street, working to provide an economic contribution to their family, but often return home at night, maintaining familial ties. Children of the streetboth work and sleep on the streets and have an absence of regular contact with family members. Children from street families live with their families in the street2.
Although street-involved children and youth (SICY) are a world-wide phenomenon, the dynamics that drive children to the streets are quite diverse and vary between high-income and low to middle-income countries3. While youth in developed countries usually
become street-involved due to familial conlict and child abuse4, children in resource-constrained settings
(RCS) succumb to street life due to abject poverty, child abuse, neglect and familial dysfunction, death of one or both parents, warand socio-cultural and religious beliefs5-9. Additionally, the solvent use habits adopted
by SICY in RCS are often divergent from those of their counterparts in high income countries10. Youth in street circumstances in high-income settings engage in using injection drugs and other substances that are not used commonly among children and youth on the streets in RCS10-12.
There are an estimated 100 million street children worldwide of which 30 million are in Asia and 10 million in Africa. India alone has an estimated number of 414,700 street children in its major cities. It is found that about 80,000 street children live in and around Bengaluru. Roughly about 60 new children land up on bus stands and railway stations every day in Bengaluru13.
MetHoDooGY
The present observational study was conducted in the Department of Forensic Medicine & Toxicology, Bangalore Medical College & Research Institute, Bengaluru during the study period of 2 years from 1st Aug 2010 till 31st Aug 2012. The study was done on the street children who stay in the areas of Railway Station, Kalasipalya and Shivajinagar of Bangalore City, who were interviewed based on a predesigned proforma relating to solvent abuse and the data were analyzed. Totally 200 street children with history of solvent abuse were enrolled into the study.
RESULTS & OBSERVATION
In the present study, 93.5% were male and 6.5% were female. Among the diferent age groups (Table 1), it was observed that the highest numbers of children were aged 14 years (31.5%) and the lowest were aged 11 years (1.5%). It was observed that, most of the street children lived (Table 2) in the premises of Gandhinagar (34%); followed by Shivaji nagar(16%), K R Market (14%) & Magadi (6.5%). It is noted that majority of the children were coolie (39%) by occupation (Table 3) followed by begging (28.5%), rag picking (24%), hotel cleaner (6%) and parking toll collector (2.5%). Majority of the street children were from Karnataka (91%), followed by Tamil Nadu (6.5%) and Andhra Pradesh (2.5%). In 64.5% of children, the parents were uneducated (illiterates).
Table 1: Age wise distribution of cases
sl no. Age number of
Table 2: Place of Living/ Native Place
sl no. Place Total number
3 Indian Journal of Forensic Medicine & Toxicology, April-June 2018, Vol. 12, No. 2 followed by shelter home (27%), railway station (14%), market (7%) and home (7%). It was interesting to note that, in 41% of cases, children started to work from an early age of 10years. Tobacco (59.5%) was the most common other substance of abuse (Table 5), followed by Gutka (19%), Alcohol (19%), Ganja (2.5%) and the other major part did not abuse any other substance (32.5%). Inluence of friends (70.5%) was the most common reason for solvent abuse (Table 6) reported by most of the children followed by curiosity (15%), for kick (12%) and for sleeping (2%).
Table 4: Shelter Place
sl no Shelter Place number Percentage
1 Foot Path 90 45%
2 Shelter Home 54 27%
3 Railway Station 28 14%
4 Home 14 7%
5 Market 14 7%
Table 5: Other Substances of Abuse Reported:
sl
Table 6: Reason for Using Solvent:
sl no. Reason For Using
Solvent number Percentage
1. Friends / peer pressure 141 70.5%
2. Curiosity 31 15.5% families. 81.9% of these children were male and earned up to 150 rupees a day. Majority of them took to solvent abuse to feel happy, and felt it as form of relief from various problems. They started with tobacco, solvents and proceeded to use of cannabis and alcohol. Pagore et al14 in a study of 115 children in Delhi found that 68.7%
of the children faced some form of abuse at home and 57.4% took to substance abuse on the streets. Earliest age to begin substance abuse was 5.5 years compared to 11 years as in our study. Poonam et al15 in a study in
Mumbai of 217 children found that 44.23% of them on the streets reported substance abuse. 11.3 years was the mean age to start use of these solvents. Males (63.54%) had higher rate of solvent abuse compared to females, which is similar to our study. According to them 39.34% used cannabis, 37.7% used alcohol and 32.8% took to solvent abuse. 70.5% of the children said they started use of drugs out of inquisitiveness.
Sharma et al16 in a study of 487 children in Delhi showed that 25.7% of them addicted to tobacco. 17% used alcohol, 15.8% used solvents and 26.3% were involved in poly substance abuse. Peer pressure was considered primarily responsible for driving these children to drug abuse. Immaculate Mary et al17
of these children sufer from some form of ill health due to this habit. Similar conditions have been reported in various cities of Nepal, East Timor, Vietnam, Hongkong etc. that 65.9% of these children live on the street with their families and 66.8% have some form of physical abuse19.
These children face a variety of personal problems at their homes and work place. They are exposed to a variety of risk factors normally considered for substance abuse. Peer pressure, work stress, easy availability of drugs, rebelliousness and development of anti social behavior on the streets push these children into solvent and other substance abuse. that the use of solvents could impact upon the ability of street children to be integrated into society and resume a normal social life. Additional efort and collaboration between policy makers, communities and researchers is essential to understand and implement mechanisms to reduce the harms associated with using inhalants, while also preventing and stopping solvent use among this vulnerable population.
Ethical Clearance: Taken from Ethics Committee from Bangalore Medical College and Research Institute, Bengaluru.
Source of Funding: Self Conlict of InteresT: Nil
REFERENCE
1. United Nations Children’s Fund (UNICEF). The State of the World’s Children 2012: Children in an UrbanWorld. NewYork: UNICEF; 2012. 2. World Health Organization (WHO). Working
With Street Children: Module 1. A Proile of Street Children. In: Dependence. Geneva: World Health Organization; 2000.
3. Le Roux J. The worldwide phenomenon of street children: conceptual analysis. Adolescence 1996;
31: 965–71.
6. Ayaya SO, Esamai FO. Health problems of street children in Eldoret, Kenya. East Afr Med J 2001; 78: 624–9.
7. Abdelgalil S, Gurgel RG, Theobald S, Cuevas LE. Household and family characteristics of street children in Aracaju, Brazil. Arch Dis Child 2004; 89: 817–20.
8. Morakinyo J, Odejide AO. A community based study of patterns of psychoactive substance use among street children in a local government area of Nigeria. Drug Alcohol Depend 2003; 71: 109– 16.
9. Njord L, Merrill RM., Njord R., Lindsay R., Pachano JD. Drug use among street children and non-street children in the Philippines. Asia Pac J Public Health 2010; 22: 203–11.
10. De Carvalho FT, Neiva-Silva L, Ramos MC, Evans J, Koller SH., Piccinini CA. et al. Sexual and drug use risk behaviors among children and youth in street circumstances in Porto Alegre, Brazil. AIDS Behav2006; 4: S57–66.
11. Roy E, Boudreau JF, Leclerc P, Boivin JF, Godin G. Trends in injection drug use behaviors over 10 years among street youth. Drug Alcohol Depend 2007; 89: 170–5.7
12. Hadland SE, Marshall BDL, Kerr T, Zhang R., MontanerJS, Wood EA. Comparison of drug use and risk behavior proiles among younger and older street youth. Subst Use Misuse 2011; 46: 1486–94.
13. Benegal V, Kulbhusan, Seshadri S, Karott M. Drug abuse among street children in Bangalore. A project in Collaboration between NIMHANS, Bangalore and the Bangalore Forum for street and working children, Monograph funded by CRY. 1998.
5 Indian Journal of Forensic Medicine & Toxicology, April-June 2018, Vol. 12, No. 2
from Delhi. INDIAN PEDIATRICS 2004 Mar; 41: 221-225.
15. Poonam R.Naik, Seema S. BansodeGokhe, RatnendraR.Shinde, AbhayS.Nirgude. Street children of Mumbai: Demographic proile and substance abuse. Biomedical Research 2011; 22(4): 495-498.
16. Sharma S, Lal R. Volatile Substance Misuse Among Street Children in India: A Preliminary Report. Substance Use & Misuse 2011; 46:46–49. 17. Immaculate Mary. Protecting Children from Substance Abuse: A Critical Need for
Meaningful Achievement of Millennium Development Goals. URL:http://www.ihsnet. org.in/IHSPresentations/ Protecting Children FromSubstanceAbuse08Jan09.pdf.
18. Khan A S, A Situational Analysis of the Street Child phenomenon in Pakistan: A Literature Review. University College London. URL: http://cfsc.trunky.net/download. asp?doc=Publications&id=405.
A Retrospective Analysis of Mandibular
Fractures: An Autopsy Study - 2012-2016
Ajay Kumar T S1, Deepa C2
1Associate Professor, Department of Forensic Medicine and Toxicology, 2Assistant Professor, Department of Dentistry, Sri Devaraj Urs Medical College, Kolar
ABSTRACT
Background and objectives: Mandibular fracture, also known asfracture of the jaw, is one of the most commonly fractured facial bones and the most commonly fractured sites are the body of the mandible. The cause of the injury may be road traic accidents, assault, falls, industrial injuries or sports injuries but the relative number of each varies considerably between countries and areas. This study intends to evaluate the age, gender distribution, the cause and anatomical distribution of mandibular fractures among autopsied cases.
Method: A retrospective study was conducted at Sri Devaraj Urs Medical College, Kolar from 2012 to 2016 and a total of 72 cases were studied.
Results: Out of 72 (100%) cases, the males 54 (75%) outnumbered females with 18 (25%) cases. 45.1% of fractured cases were seen in the age group of 21 – 30 years. Road Traic Accidents 40 (55.6%) was the cause of mandibular fractures in majority of the subjects. The most common site of mandibular fracture was body of mandible with 28 (38.8%) cases.
Conclusion and interpretation: The results could be useful in interpreting the pattern of mandibular fractures among autopsied cases. Since the high frequency of mandibular fractures are due to RTA, the various preventive measures can be employed to minimize the sequelae of mandibular fractures like creating awareness among public about safety measures.
Keywords: Mandibular fractures, Road Traic Accidents, Autopsy, Body of mandible.
INTRODUCTION
Mandibular fracture, also known asfracture of the jaw, is abreakthrough themandibular bone.
It was irst described by Egyptian Papyrus in 1650 BC.1 Given its prominent anatomic location;
the mandible is one of the most commonly fractured facial bones. Before the invention of the automobile, mandibular fractures were most often caused by assault or other blunt trauma like falls, industrial injuries or sports injuries to the jaw. However, Road Traic
Corresponding author:
Dr. Deepa C
Assistant Professor, Sri Devaraj Urs Medical College, Kolar. E-mail: [email protected]
Accidents (RTA) are now responsible for an equal share of the incidence of such injuries.2 In terms of
violence, young males are most at risk with alcohol an aggravating factor. Women and children are much less at risk but can be from domestic violence.3 The relative
number of each varies considerably between countries and areas and they can be usually attributed to cultural, social, environmental and economic factors.4
7 Indian Journal of Forensic Medicine & Toxicology, April-June 2018, Vol. 12, No. 2
The fracture site depends upon the mechanism of injury, magnitude and direction of impact force, prominence of the mandible and anatomy of site.4 The
aim of the present study was to assess age and gender distribution, etiology and anatomic distribution of mandibular fractures among autopsied cases.
MATERIALS AND METhOD
This retrospective study was carried out at Sri Devaraj Urs Medical College, Kolar from 1st January 2012 to 31st December 2016 comprising all cases which were autopsied in the Department of Forensic Medicine.
In this study, the demographic variables such as age and gender, etiology and the site of mandibular fractures were noted. The medico-legal records were also referred for additional information.
The data obtained was recorded in the pre-designed and pre-tested proforma, which comprised relevant data and analyzed.
RESULTS
A total of 72 cases presenting with mandibular fractures of 1423 number of autopsied cases during 2012 to 2016 in the Department of Forensic Medicine were studied.
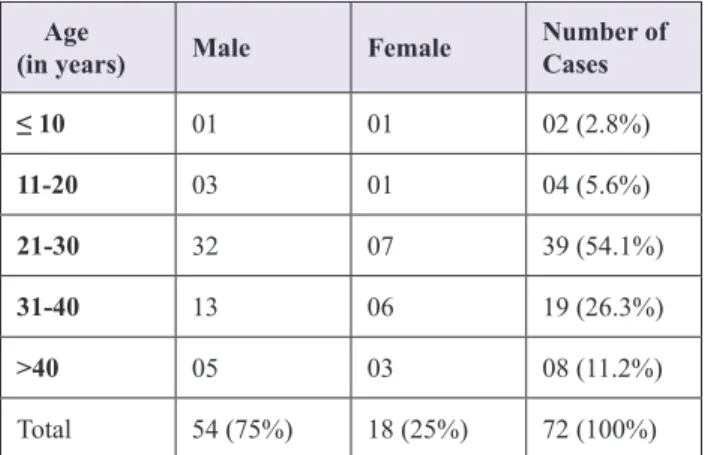
Table 1. Distribution of Mandibular fracture cases according to age and sex
Age
(in years) Male Female
number of Cases
≤ 10 01 01 02 (2.8%)
11-20 03 01 04 (5.6%)
21-30 32 07 39 (54.1%)
31-40 13 06 19 (26.3%)
>40 05 03 08 (11.2%)
Total 54 (75%) 18 (25%) 72 (100%)
Out of 72 (100%) cases, 54 (75%) were males and 18 (25%) were females. The maximum numbers of fractured cases 39 (45.1%) were seen in the age group of 21 – 30 years. More than 2/3rd of the cases were between
21 – 40 years.
Table 2. Distribution of Mandibular fracture cases according to Etiology
Etiology Male Female number of
Cases
RTA 32 08 40 (55.6%)
Fall 18 05 23 (31.9%)
Assault 01 04 05 (6.9%)
Sports 02 00 02 (2.8%)
Other
causes 01 01 02 (2.8%)
Total 54 (75%) 18 (25%) 72 (100%)
Road Traic Accidents 40 (55.6%) was the cause of mandibular fractures in majority of the subjects, followed by Fall with 23 (31.9%) cases.
Table 3. Distribution of Mandibular fracture cases according to Anatomical site
Anatomical Site number of Cases
Para symphysis 12 (16.7%)
symphysis 02 (2.8%)
Body of Mandible 28 (38.8%)
Angle 08 (11.2%)
Ramus 01(1.4%)
Condyle 07 (9.7%)
Coronoid 01(1.4%)
More than one site 13 (18.1%)
Total 72 (100%)
The most common site of mandibular fracture was body of mandible with 28 (38.8%) cases, followed by fracture of mandible with more than one sites with 13 (18.1%) cases. The fracture of ramus and coronoid were the least common sites with 01 (1.4%) cases each.
DISCUSSION
bones of the face. Mandibular fractures occur twice as often as midline fractures. The energy required to fracture it being the order of 44.6 – 74.4 kg/m, which is about the same as the zygoma and about half that for the frontal bone. It is four times as much force is required to fracture maxilla.5
In this study, the males 54 case (75%) outnumbered the females with 18 cases (25%) and the male to female ratio being 3:1. Our results are consistent with the study conducted by Kamlai U et al,6 Ansari et al,7 Kanasakar
et al,4 adi et al, Shapiro et al.8
The male dominance may be due to the paternalistic nature of our society where males keep themselves most of the time outdoors and lead a more active life.
It was also observed that 54.1% of the mandibular fractures occurred in the age group of 21-30 years. More than 2/3rd of the cases were between 21 – 40 years. The
least number of cases were seen in the age group less than 20 years and more than 40 years with 06 cases (8.4%) and 08 cases (11.2%) respectively.
Similar indings were noted in the studies conducted by Abbas et al 9 and Kansakar et al,4 but the study
conducted by Shapiro et al8 reported 34.1 years as mean age. This can be explained by the fact that at young age, people are more mobile, socially active, in business, sports and high speed transportation, inter personal violence, alcohol abuse and so forth.
The lower frequency of mandible fracture is seen at very young age which can be due to high elasticity of bone, poor pneumatization, thick surrounding adipose tissue and internal stabilization by unerupted teeth within maxilla and mandible. In old age, due to lower physical activities mandibular fractures are least common.
Out of 72 cases (100%), RTA (55.6%) is still mainstay as the most common cause of mandibular fracture in our population, which is in accordance with Shah et al,10 Al Ahmed et al,11 Natu SS et al,5 Vyas
A et al12. In this study, the etiology next to RTA was
followed by Fall with 23 (31.9%) cases.
Some of the authors, Jung HW et al,13 Mittal et al14
in their studies opined fall as the commonest cause of mandibular fractures and others Ellis E et al,15 Rashid
A,16 Kirk L,17 Dongas P18 stated intentional injury or
violence as the commonest cause.
The diference in the main cause of injury is largely dependent on the cities where studied were conducted, as well as, the population. High incidence of RTA in our study may be attributed to reckless driving, insuicient helmet and seatbelt usage and the availability of motorcycle for the young generation and consumption of alcohol while driving/riding.
With respect to the anatomical site, the commonest fracture region was the body of mandible with 28 cases (39.8%), followed by more than one sites 13 cases (18.1%), parasymphysis with 12 cases (16.7%). Similar results were reported by Brook IM et al19 and Olson RA
et al 20.
The anatomic distribution and incidence of mandibular fracture are widely variable. The frequently fractured site varied from author to author. Chuong R et al21 opined symphysis as most frequent, Dongas P et al18
and Ogundare BO et al22 opined angle as commonest,
Kansarkar et al,4 Vyas A et al,12 Natu SS5 reported
parasymphysis the commonly fractured site. CONCLUSION
This study helps to interpret the pattern of mandibular fractures among autopsied cases. The mandibular fractures were more common in males (75%) than females (25%), with highest number of cases (45.1%) were seen in the age group of 21 – 30 years. More than 2/3rd of the cases were between 21 – 40
years. RTA was the commonest cause for mandibular fractures with (55.6%) followed by fall (31.9%). The body of the mandible was the commonest fractured site (38.8%), followed by more than one site (18.1%), parasymphysis (16.7%).
Since the high frequency of mandibular fractures are due to RTA, the various preventive measures can be employed to minimize the sequelae of mandibular fractures like creating awareness among public about safety measures.
Conlict of Interest: The authors do not have any conlict of interest in publishing this article.
source of Funding. -Nil
9 Indian Journal of Forensic Medicine & Toxicology, April-June 2018, Vol. 12, No. 2
REFERENCES
1. Lipton JS. Oral Surgery in Ancient Egypt as relected in the Edwin Smith Papyrus. Bulletin of the History of Dentistry 1982; 30: 108.
2. William C Soule. Mandibular Fracture Imaging. Medscape. [Cited on Jul 01, 2015]. Available from: http://www. http://emedicine.medscape. com/article/391549-overview.
3. Mandibular Fractures and Dislocations. Patient. Available from: https://patient.info/in/doctor/ mandibular-fractures-and-dislocations.
4. Kansakar N, Budhathoki B, Prabhu N, Yadav A. Pattern and Etiology of Mandibular Fractures reported at Nepalgunj Medical College: A Prospective Study. Journal of Nepalgunj Medical College 2015; 13 (2): 21-24.
5. Natu SS, Pradhan H, Gupta H, Alam S, Gupta S, Pradhan R et al. An Epidemiological study on pattern and Incidence of Mandibular Fractures: Plastic Surgery International 2012; (2012, Article ID 834364:1-7.
6. Kamali U and Pohchi A. Mandibular fracture at HUSM: A 5-year retrospective study. Arch Orofac Sci. 2009;4:33-5.
7. Ansari SR, Khitab U, Qayyum Z, Khattak A. Retrospective analysis of 268 cases of fractures of mandible. Pak Oral Dent J 2004; 24:135-8. 8. A. J. Shapiro, R. M. Johnson, S. F. Miller, and M.
C. McCarthy, “Facial fractures in a level I trauma centre: the importance of protective devices and alcohol abuse,” Injury, vol. 32, no. 5, pp. 353– 356, 2001.
9. Abbas I, Ali K, Mirza YB. Spectrum of mandibular fractures at tertiary care dental hospital in Lahore. J Ayub Med Coll Abbotabad 2003;15:12-4. 10. A. Shah, A. S. Ali, and S. Abdus, “Pattern and
management of mandibular fractures: a study conducted on 264 patients,” Pakistan Oral & Dental Journal, vol. 27, no. 1, pp. 103–106, 2007.
11. H. E. A. Ahmed, M. A. Jaber, S. H. Abu Fanas, and M. Karas, “The pattern of maxillofacial fractures in Sharjah, United Arab Emirates: a review of 230 cases,” Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontology, vol. 98, no. 2, pp. 166–170, 2004.
12. Vyas A, Mazumdar U, Khan F, Mehra M, Parihar L, Purohit C. A Study of mandibular fractures over a 5 year period of time: A Retrospective Study. Contemporary Clinical Dentistry 2014; 5 (4): 452-455.
13. Jung HW, Lee BS, Kwon YD, Choi BJ, Lee JW, Lee HW et al. Retrospective clinical study of mandible fractures. Journal of Korean Association of Oral Maxillofacial Surgery 2014 Feb; 40 (1): 21-26.
14. Mittal G, Mittal S. Mandibular fractures at veer chandra singh garhwali government medical science and research institute, garhwal region, uttarakhand, India: a retrospective study. Annals of medical and health sciences research. 2013;3(2):161-5.
15. Ellis E, Moos KF and El-Attar A, Ten years of mandibular fractures: an analysis of 2,137 cases, Oral surgery, oral medicine, oral pathology, 59(2), 1985, 120-129. Mandibular Fractures: A review of 1,067 cases, J Oral Maxillofac Surg, 50(6),1992,586-589. 18. Dongas Pand GM Hall, Mandibular fracture
patterns in Tasmania, Australia, Australian Dental Journal, 47(2), 2002, 131-137. cases. J Oral Maxillofac Surg. 1982;40:23–8.
21. Chuong R, Donof RB, Guralnick WC. A
retrospective analysis of 327 mandibular fractures. J Oral Maxillofac Surg. 1983;41:305– 9.
Infection Control in Orthodontics: A Review
Mithun K1, Ashith M V2, harshitha V3, Valerie Anithra Pereira4, Deesha Kumari5
1Assistant Professor, Department of orthodontics, A.J institute of Dental Sciences, Mangalore, 2Reader, Department
of Orthodontics, Manipal College of Dental Sciences Mangalore, 3Reader, Department of Orthodontics, A.J
Institute of Dental Sciences. Mangalore, 4Post graduate Student, Department of Periodontics and Implantology,
Coorg Institute of Dental Sciences, 5Assistant Professor, Department of Public Health Dentistry,
AB Shetty Memorial Institute of Dental Sciences
ABSTRACT
Dental care professionals are at an increased risk of cross infection while treating patients.This occupational potential for disease transmission become evident initially when one realises that most human microbial pathogens have been isolated from oral secretions. Because of repeated exposure to micro-organisms in blood and saliva, incidence of certain infectious diseases has been signiicantly higher among dental professionals than observed for general population.
Keywords: Infection control, Sterilization, Disinfection, Orthodontic oice, Waste management
Corresponding author: Mithun K
Assistant Professor, Department of Orthodontics, A.J institute of Dental Sciences, NH-66, Near Kuntikana Road, Kuntikana Mangalore: 575004.
Mob. +919902355948,
Email: [email protected]
INFECTION CONTROL IN ORThODONTICS
Dental care professionals are at an increased risk of cross infection while treating patients. Incidence of infectious diseases has been signiicantly higher among dental professionals than observed for general population. Orthodontists are exposed to a wide variety of microorganisms in orthodontic oice by contaminated instruments, inhalation of aerosols or via percutaneous injuries with archwires, ligature wires, band material and other sharp cutting instruments.1 A study found
that orthodontists have the second highest incidence of hepatitis B among dental professionals. 2New materials
“as received” from the manufacturers are not free from bacterial contamination before use in patients. Further studies would be required to determine the level of risk that this poses.3
Means of transmission
1. Patient to Dental Team: It can be by three
means
1) Direct contact : With patient’s saliva or blood 2) Droplet infection: They occur as a result of sprays, spatter or aerosols from patients mouth.
3) Indirect contact: involves transfer of microorganisms from the source (e.g., the patient’s mouth) to an item.
2. Dental Team to Patient:If the hands of dental
team member contain lesions or other nonintactskin.If a member of the dental team bleeds on instruments or other items that are then used in the patient’s mouth, cross infection may result.
3. Dental Oice to CommunityMicroorganisms
from the patient contaminate items that are sent out or are transported away from the oice. Dental laboratory technicians have been occupationally infected with hepatitis B virus (HBV). Also, regulated waste that contains infectious agents and is transported from the oice may contaminate waste handlers if it is not done in proper containers.
Goals of infection control4
11 Indian Journal of Forensic Medicine & Toxicology, April-June 2018, Vol. 12, No. 2
1. Decrease the number of pathogenic microbes to the level where normal body resistance mechanisms can prevent infection .
2. Break the cycle of infection from dentist, assistant & patient & eliminate cross infection.
3. Treat all the patient & instrument as though they could transmit an infectious disease
4. Protect patient & personnel from infection & protect all dental personnel from threat of malpractice.
Infection control stratergy
Each clinical practice must have a written infection control policy which must be upgraded with the latest recommendations. Infection control strategy involves various steps
1.Patient screening: A patient with subclinical
infection is a potential source of cross-contamination. Therefore, all the patients must be screened by obtaining the relevant medical and dental history from them and a physician must be consulted if doubt arises
2.Instrument processing:
a. Containment: During and after each procedure, every efort should be made to conine all instruments and devices that have come in contact with the patient to a well-deined and limited area. Rationale: when contaminated instruments are conined to a limited area, microorganisms are not spread unnecessarily. Utility gloves, protective eyewear and clinic garment should be worn
b. holding (presoaking): All contaminated instruments should be stored in a presoak solution immediately after the procedure. Rationale: It is seldom possible to clean the instruments used on each patient immediately after the procedure. The debris on such instruments may dry, making them more diicult to clean. Recommendations:Use presoak solutions which consists of detergents or detergents containing disinfectants like phenolic compounds. Thepre-soaking solution should be discarded at the end of the day.
c. Pre-cleaning/pre-sterilization: All contaminated instruments should be properly cleaned before the process of sterilization. Rationale: Blood, Saliva and material on instruments can insulate microorganisms from sterilizing agents, and interfere with efective
sterilization. Hence cleaning reduces this bio burden to facilitate sterilization.
-Manual cleaning or hand scrubbing: Time
consuming and increases the chances of accidental puncture or cuts through direct handling of sharp and pointed instruments. Complete personal protective equipment should be worn. Instruments should be immersed in a detergent and cleaned under running water using a soft brush with a long handle.
- Ultrasonic cleaning: It is efective, time saving
and much more safe than hand scrubbing. A cleaning solution that is speciically recommended by the manufacturer for use in ultrasonic cleaner should be used.5
Presoaked instruments contained in the basket should be immersed in the cleaning solution of ultrasonic cleaner. The cleaner should be covered and operated for atleast 6-10 mins. After cleaning, instruments should be thoroughly rinsed. 6
d. Corrosion control, drying and lubrication: Before subjecting the instruments for sterilization, the instruments must irst be cleaned thoroughly with no debris and dried to reduce chances of corrosion and a rust inhibitor (dip or spray) should be applied. Lubrication of instruments with movable parts like hinges of orthodontic pliers should be done prior to steam sterilization with a water based lubricant. A sodium nitrite rust inhibitor can also be used. Corrosion resistance is directly proportional to its chromium content and inversely proportional to its carbon content. Disinfectants, or detergents with pH greater than 8.5 can disrupt the chromium oxide layer. Blood saliva and debris if not rinsed and directly autoclaved can cause pitting corrosion. Chrome plated instruments should be processed separately from stainless steel ones, because of electrolytic action which can carry carbon particles from exposed metal of a chrome plated instrument and deposit them on stainless steel. Chrome plated pliers are more resistant to corrosion than stainless steel pliers.
distributed to chairside. Recommendations: Only a wrapping material that is designed as a sterilization wrap for a particular type of sterilizer should be used. Trays and cassettes are very good options for packaging orthodontic instruments and bands, because they retain instruments during pre-soaking, ultrasonic cleaning, sterilization and storage, and inally for use at chairside. They eliminate the potential risks like puncturing or cuts while handling sharp contaminated instruments
Autoclave sterilization must allow steam to penetrate inside it and reach every instrument contained in it and all its surfaces. Requirements of packaging materials: Dry heat sterilization must not insulate items from heat, must not get destroyed by temperature used. Unsaturated chemical vapor sterilization must allow vapour to precipitate on contents and not react with the vapour.
3. Sterilization 1)heat sterilization
a.Dry heat sterilization: This method uses hot air to kill microorganisms and has the advantage of not causing corrosion. It dehydrates the bacterial protein and decreases its resistance to denaturation
At a given temperature, dry heat is less eicient than moist heat, because dry heat is not as eicient a heat conductor as moist heat.
Rapid heat transfer Sterilizer: Also called as forced air convention units. The mechanism of bacterial killing is similar to conventional dry heat unit. They use higher temperature than other dry heat units and there is a controlled internal air low within the chamber. As a result, they have a substantially shorter sterilization intervals.
b.Steam pressure sterilization: Steam sterilization is the oldest and most commonly used of acceptable methods for instrument sterilization in dentistry since many years. Sterilization is accomplished by making use of steam under pressure which causes denaturation and coagulation of microbial proteins.Mechanism: When water heated under pressure, its boiling point is raised together with the temperature of the generated steam.
c. Gas or ethylene oxide sterilization
Ethylene oxide: The use of ETO is recognized by
the American Dental association (ADA) and Centers for Disease control and prevention (CDC) as an acceptable method of sterilization for the following items that can be damaged by heat and/ or moisture, and those that can be cleaned and dried thoroughly.
MECHANISM: A gas with very high penetrating ability. It acts by alkylating the amino, carboxyl, sulphhydril groups in protein molecules thus reacts with RNA and DNA. trays: ethylene oxide sterilization or disinfection by NaOCl or iodophor. Alginates are relatively less stable, hence ADA recommends disinfection of alginates by immersion in diluted sodium hypochlorite or iodophors with minimal disinfection time. After disinfection the impressions should be rinsed to remove residual disinfectant.
b. Disinfection of removable appliances: Immerse completely into a disinfectant for the time recommended for tuberculocidal disinfection. ADA reccomends immersion in iodophors or sodium hypochlorite for 10 mins. Disinfection of baseplates of removable orthodontic appliances by using 0.12% chlorhexidine spray once or twice a week reduced the contamination by Mutans Streptococci on the acrylic surface.7
c. . Disinfection of wax bites: ADA recommends
disinfection of wax bites by a spray-wipe-spray techniqueShould remain wet after the second spray for atleast 10 mins. Rinsed again to remove residual disinfectant.
d. Stone cast disinfection:ADA recommends disinfection of wax bites by a spray-wipe-spray technique should remain wet after the second spray for atleast 10 mins.
13 Indian Journal of Forensic Medicine & Toxicology, April-June 2018, Vol. 12, No. 2
f. Orthodontic bands: Thread the bands to be sterilized on the auxiliary wire, and suspend the wire across the rack to dry heat or autoclave sterilization
g. Orthodontic wires: TMA wires treated with ethylene oxide, autoclaving. NiTi wires treated with
ethylene oxide. Stainless steel wires treated with autoclave, dry heat and ethylene oxide. 9
h. Orthodontic marking pencils:Conventional
orthodontic pencils can not be autoclaved. Gas sterilization can be done. 10
i. Elastomeric Chains and Ligatures: Chemicals are not suitable for disinfection of elastomeric ligatures and E-chains because they alter the physical properties of the elastics. For E-chains it is best to cut-of some more above that is required and discard the rest.
Sterilization monitoring: The goal of sterilization is to eliminate all forms of microorganisms on the items being processed. Reports describing spore testing of sterilizers used in dental oice have indicated sterilization failure frequencies from 15.1% – 51%. ADA recommend weekly spore testing of dental oice sterilizer. Types of monitoring
a. Biological monitoring: Biological indicators
contain highly resistant bacterial spores that are more diicult to kill than any other microbes. Types of biological indicators :
-Bacillus stearothermophilus - steam or chemical vapor sterilization
-Bacillus subtilis - dry heat or ethylene oxide gas sterilization.
b. Chemical monitoring
It involves use of color-changing chemical indicators on the outside and inside of packs, bags, cassettes or trays.
-Rapid-change indicators: Tapes, labels and
bag markings are referred to as external chemical indicators. Change in color after brief exposure to high temperature, which indicates that the items have been processed through a sterilizer.
-Slow-change or integrated indicator: Indicators designed to use inside of packs, bags or trays, called internal indicators are more accurate than external
indicators. Atleast one item per load should contain an internal indicator.
c. Physical Monitoring: Physical monitoring of the
sterilization process involves observing the gauges and displays on the sterilizer and recording the sterilizing temperature, pressure and exposure time. Thus, physical monitoring may not detect problems resulting from overloading, improper packaging material or use of closed containers.
handling processed instruments
a. Drying and Cooling : Packs, pouches or
cassettes processed through steam sterilizer may be wet and must be allowed to dry before handling
b. Storage : Handling of sterile packages should be kept to a minimum.The oldest sterile should be used irst as long as the packaging material is intact. This is referred to as the “irst in-irst out” system of stock rotation.11
c. Distribution : Instruments from sterile packs
or pouches can be placed on sterile, disposable trays. Sterilized instrument cassettes are distributed to and opened at chairside
3. Personal protective and barrier technique: a. Gloves: The operator should thoroughly rinse penetration of con taminated luids which collect on the outer mask layer.
c. Eyewear: Eyewear should be disinfected between
patients by spray wipe spray method.
d. Pre procedure antiseptic mouthwash: during
invasive procedure as mini implant placement. A long lasting antimicrobial rinse such as 0.12% clorhexidine gluconate can suppresses oral microorganisms for upto 5hrs.
4. Dental oice design
should incorporate a smooth eicient operational low. Instrument recirculation center (IRC) should not be attached to treatment and nontreatment areas or placed in a walkway
b. Cabinetry :The number of drawers and their contents should be minimized to simplify cleanup procedures. Treatment room cabinetry should be positioned on both sides of the patient’s chair. This will allow both the doctor and assistant access to essential side support areas and provide lexibility to both right and left-handed clinicians working in the same space.
c. Laminates and wall and loor coverings :It
should be easy to clean and disinfect all the surfaces. Avoid wood surfaces textured wall coverings and decoration. Laminates in long run hold their clean appearance.
d. Ventilation :Work areas must have positive
ventilation to control noxious vapours form various chemicals used in laboratory and sterilization areas.
5. Water system: The dental unit water supply
systems (DUWS) are contaminated with micro organisms in the form of a bioilm.new heat sterilizable independent water delivery system (AquaSept) has been introduced in the market which eliminates the possibility of DUWS contamination. Heat sterilization of all system components between patients prevents bioilm build-up and kills passively retracted pathogens. The CDC recommends Independent water reservoir, Line ilters, Handpiece for 20- 30 sec, Antiretraction valve, Periodic chemical treatment.
5. Waste management
Management of Regulated Medical Waste in Dental HealthCare Facilities is done by use of color-coded or labeled container that prevents leakage (e.g., biohazard bag) to contain nonsharpregulated medical waste. Handling, segration, mutilation, disinfection, storage, transportation and inal disposal are vital steps for safe and scientiic management of biomedical waste management in any establishment. The commonly used items in an orthodontic oice and their disposal protocol are shown in (Table 1)
Table 1: Orthodontic waste disposal protocol
Impression material(Discarded/Used) Immerse 1% Sodium hypochlorite solution bucket for 24 hours and then Dispose in Black container
Dental Casts (Discarded/Used) Immerse 1% Sodium hypochlorite solution bucket for 24 hours and then Dispose in Black container
Removable Appliances with wire component
(Used/Broken not to be worn by patient anymore Sharps Container containing 1% Sodium hypochlorite Wires, steel ligatures, orthodontic miniimplants,
Needles after being burnt, Sharps Container containing 1% Sodium hypochlorite
Wax bite registrations Red container
Debonded brackets, buttons and other attachments Red container E-chain, elastic ligatures, elastics Red container
Mouthmask, Gloves Red container
Headcap, Shoe covers Black container
Infected cotton Yellow container
Syringe (after breaking at Hub in Needle destroyer) Red container
CONCLUSION
Infection control is half the treatment of any practice. It should be remembered that, we are health care professionals who are supposed to treat and not infect. We are dealing with very fragile and viable tissues
15 Indian Journal of Forensic Medicine & Toxicology, April-June 2018, Vol. 12, No. 2
Conlict of Interest: Nil Source of Funding: Self
Ethical Clearance: Ethical clearance not required as it is review article
REFERENCES
1. Bagramian RA, McNamara JA Jr. A prospective survey of percutaneous injuries in orthodontists. Am J OrthodDentofacOrthop 1998;114:654-8 2. Starnbach, H. and Biddle, P.: A pragmatic
approach to asepsis in the orthodontic oice, Angle Orthod.1980.50:63-66.
3. Christopher S. Barker Microbial contamination of “as received”and “clinic exposed” orthodontic materials.Am J OrthodDentofacialOrthop 2013;143:317-23.
4. Council on Dental Therapeutics and Council on Prosthetic Services and Dental Laboratory Relations. Guidelines for infection control in the dental oice and the commercial dental laboratory. J Am Dent Assoc 1985;110:969-72.
5. Spolyar JL, Johnson CG, Head R, Porath L. Ultrasonic cold disinfection. J ClinOrthod 1986;20:852-3.
6. Spolyar JL, Johnson CG, Head R, Porath L. Ultrasonic cold disinfection.JClinOrthod 1986;20: 852-3.
7. Evaluation of home disinfection protocols for acrylic baseplates of removable orthodontic appliancesAm J OrthodDentofacialOrthop 2011;140:51-7
8. Efect of routine steam autoclaving on orthodontic pliers European Journal of Orthodontics (1993) 15 (4): 281-290.
9. Staggers JA, Margeson D. The efects of sterilization on the tensile strength of orthodontic wires. Angle Orthod. 1993 Summer;63(2):141-4. 10. Ascencio F, Langkamp HH, Agarwal S, Petrone
JA, Piesco NP. Orthodontic marking pencils: a potential source of cross-contamination. J ClinOrthod. 1998 May;32(5):307-10
A Study on Demographical and Clinical Proile
and the Outcome of Snake Bite Victims in a
Rural Tertiary Care hospital
Shreedhara K C1, sidramappa Gouda2
1Assistant Professor, Department of Forensic Medicine, AdichunchangiriInstituete of Medical Sciences ,
B G Nagar, Mandya, 2Assistant Professor, Department of Forensic Medicine,
Navodaya Medical College, Raichur
ABSTRACT
Background: Snake bite is an important occupational and rural hazard because India has always been a land of Exotic snakes.Snake bite is a major public health problem throughout the world, more so in tropical and subtropical countries. In a predominantly agricultural country like India with its rich lora-fauna, the encounter between man and snake is frequent occurrence. With rapid urbanization and deforestation, the incidence of snake bite is high and forms a signiicant group of hospital admissions. Objective : To know demographical and clinical proile of snake bite patients presenting to a Rural tertiary care centre in mandya. Materials and method: A cross sectional study was conducted in Adichunchanagiri Institute of Medical Sciences from March 2015 to March 2016. All the cases with presented with history of snake bite and or clinical features and admitted to hospital were included in the study. A total of 46 Cases of Snake bite were admitted during the study period. Results: In this study majority of victims were in the age group of 25-50 years. The male to female ratio was almost more than 2:1. The mean age of the patient was 36.58 years. 60.85% cases of cases presented to emergency room with pain and tenderness in the bite site alone and rest of the cases with other signs of local envenomation. Conclusion: Awareness should be created among the population regarding the implications of snake bite on the loss of life. Basic First aid, use of boots and importance of the early hospitalization for the early recovery has to be advised and educate to the population at risk.
Keywords: Snake bite, Venom, Rural, Occupation,
INTRODUCTION
Snakebite is a common medical emergency and an occupational hazard in most parts of India.
Early in 2009, snake-bite was inally included in the WHO’s list of neglected tropical diseases conirming the experience in many parts of this region that snake- bite is a common occupational hazard of farmers, plantation workers and others, resulting in tens of thousands of deaths each year and many cases of chronic physical handicap.1
Corresponding author :
Dr. sidramappa Gouda
Assistant Professor, Department of Forensic Medicine & Toxicology, Navodaya Medical College, Raichur Mob. 7899606175, E-mail: [email protected]
Various studies have shown that nearly 15,000 to 25,000 people die annually in India due to snake envenomation, whereas the world mortality is estimated to be 30,000 to 40,000 per annum. 2. In India death due
to snake bite accounts to total of 2.8 to 5.3%,which is much higher when compare to USA(20 death per year) and Europe(1 death in 3-5year). 2
The factors like favorable climate, rural predominance of the population and farming practiced in India are the major contributing factor for the snake bite. Hence India is also know as land of Exotic Snakebites
17 Indian Journal of Forensic Medicine & Toxicology, April-June 2018, Vol. 12, No. 2
Many species are mainly nocturnal (night hunters) e.g. kraits, but other species are mainly diurnal (day- time hunters). People must be specially vigilant about snake-bites after rains, during looding, at harvest time and at night and to be taken necessary precaution.
Snake-bite is an environmental, occupational and climatic hazard in rural area and attention to the following recommendations for community education might reduce the risk of bites. Snakes have adapted to a wide range of habitats and prey.
Most often snake bites are reported due to human interaction with the habitat of the snakes.
In India there are about 216 species of snakes of which about 52 are venomous and of these only 5 varieties of snakes are commonly encountered as the cause of snakebite poisoning2. They are,
1. Russell’s viper - Doboiaruselli 2. Cobras - (Common cobra )- NajaNaja 3. Krait – BungarusCaeruleus
4. Saw scaled viper - EchisCurinatus and Pit viper. 3
Hence This Study Is Undertaken To Asses The Demographical And Clinical Proile And The Outcome Of Snake Bites In The Rural Area Of Mandya District, Karnataka.
OBJECTIVE
To know demographical and clinical proile of snake bite patients presenting to a rural tertiary care centre in Mandya district Karnataka.
MATERIALS AND METhOD
A cross sectional study was conducted in Adichunchanagiri Institute of Medical Sciences from March 2015 to March 2016. All the cases with presented with history of snake bite and or clinical features and admitted to hospital were included in the study. A total of 46 Cases of Snake bite were admitted during the study period .The admitted patients were admitted in the emergency ward and history of the snake bite , time site, identiication marks of snake ,any signiicant features of snake , clinical features and symptoms were evaluated on admission. Immediately after the admission and irst aid of the cases the patients’ blood was sent for routine
examination and complete blood picture.The number of the doses of Anti Snake venom used was also noted.
RESULTS
A total number of 46 patients were admitted in the Adichunchanagiri Institute of Medical Sciences during the study period. In this study majority of victims were in the age group of 25-50 years. The male to female ratio was almost more than 2:1. The mean age of the patient was 36.58 years.
Table 1 : Socio Demographical Proile of the
cases
AGe FREQUENCY PERCENTAGE
<20 4 8.6
20-29 12 26.08
30-39 14 30.43
40-49 9 19.56
50-59 5 10.86
60-69 2 4.34
seX FREQUENCY PERCENTAGE
MALE 27 58.69
FEMALE 19 41.31
OCCUPATION FREQUENCY PERCENTAGE
Farmer 26 56.5
Labour 12 26
Housewife 6 13
Others 2 4.5
EDUCATION
STATUS FREQUENCY PERCENTAGE
Illiterate /till 4th 32 69.5
5-10 th 8 17.39
More than 10 th 6 13.11
Table 2: Time and Site of Snake Bites Site of bite Head and neck
Upper limbs
Out of 46 snake bites victims 60.8% type of snake were not identiied. Hematotoxic viper bites were next most common snake bites. About 70% victims were of hematotoxic snake bite victims among the unidentiied cases. Rest consisted both neuro and hematotoxic snake bites.
Out of 46 cases 76.1% of bites were mostly on the lower limbs involving ankle and foot including webspaces . Signiicantly the bites were more frequent around dusk and early night .Once the dim light sets in movement of mankind also reduces and the snakes and other creatures move out of their habitat in search of prey. So this is the time when patients account for maximum no. of snake bites.
Table 3: Clinical Proile of Snake Bite
Frequency Percentage
Haematotoxic Manifestation NilBleeding from site 3016 65.234.8
Neuroparalytic Manifestation NilPtosis incision in 10.8% of snake bite victims.
60.85% cases of cases presented to emergency room with pain and tenderness in the bite site alone and rest of the cases with other signs of local envenomation. Bleeding from the site of bite was most common hematotoxic manifestation seen in our study and was
mostly seen in the viper snake bites.Ptosis& respiratory paralysis was seen in as the neurotoxic Manifestation and was mostly seen in krait and cobra bites.