Perianesthesia Management for
Arrhythmia Intervention Procedure
Bambang Pujo Semedi
Dept. Anestesiologi dan Terapi Intensif
FK Unair – RSUD Dr Soetomo
Fakta….
•
Aritmia jantung merupakan penyebab morbiditas dan mortalitas
yang bermakna di AS
•
> 40,000 pasien mengalami aritmia yang berakhir dengan kematian
tiap tahun
•
> 800,000 aritmia yang mengharuskan pasien dirawat di RS
•
Terapi aritmia meliputi
•
Terapi medikamentosa
•
Device therapy
•
Prosedur ablasi intervensional (operatif maupun kateterisasi jantung)
•
Terapi aritmia mulai berubah sejak teknologi kateterisasi
semakin canggih dan berkembangnya lab elektrofisiologi
•
Peran anestesi sangat penting untuk mendukung keberhasilan
terapi intervensional.
Pemahaman elektrofisiologi jantung sangat
penting bagi seorang ahli anestesi…
3
Enam tahap konduksi jantung
dan kontraksi…
1. Depolarization of Atrial Muscles – P wave
2. Atrial Systole
3. Depolarization
of Ventricular
Muscles – QRS
wave
4. Ventricular systole
5. Repolarization
of Ventricular
Muscles – T wave
6. Ventricular
Diastole
44 Cardiac Elect rophysiology: Diagnosis and Treatment
75
familiarization with the anatomy of the normal cardiac conduction system, the electrophysiologic basis for common cardiac rhythm dis-orders, and the approaches to their ablative treatment. This chapter discusses these basic principles, together with special anesthetic con-siderations when unique to a particular form of treatment.
BASIC ELECTROPHYSIOLOGIC PRINCIPLES
Anat omy and Physiology of t he Car diac
Pacemaker and Conduct ion Syst ems
Sinus Node
The sinoatrial node (SAN; Figure 4-1) is a spindle-shaped structure composed of highly specialized cells located in the right atrial sulcus terminalis, lateral to the junction of the superior vena cava (SVC) and the right atrium10,11 (see Box 4-1 for a summary of the anatomy of the
cardiac pacemaker and conduction system). Three cell types have been identified in the SAN (nodal, transitional, and atrial muscle cells), but no single cell appears to be solely responsible for initiating the pace-maker impulse. Rather, multiple cells in the SAN discharge synchro-nously through complex interactions.12–14 Rather than a discrete and
isolated structure, studies suggest that the SAN consists of three distinct regions, each responsive to a separate group of neural and circulatory stimuli.15 The interrelationship of these three regions appears to
deter-mine the ultimate rate of output of the SAN. Although the SAN is the
site of primary impulse formation, subsidiary atrial pacemakers located throughout the right and left atria also can initiate cardiac impulses.16–18
In a series of studies both in dogs and humans, it was confirmed that there is an extensive system of atrial pacemakers widely distributed in the right and left atria, as well as in the atrial septum.15,19–21 Because the
atrial pacemaker system occupies a much larger area than the SAN, it can be severed during arrhythmia surgery, resulting in impaired rate responsiveness.10 However, it is extremely difficult to completely abolish
SAN activity through catheter-based ablation techniques.
The arterial supply to the SAN (SAN artery) is provided from either the right coronary artery (RCA; in 60% of the population) or the left circumflex coronary artery (see Figure 4-1). The SAN is richly inner-vated with postganglionic adrenergic and cholinergic nerve terminals. Vagal stimulation, by releasing acetylcholine, slows SA nodal automa-ticity and prolongs intranodal conduction time, whereas adrenergic stimulation increases the discharge rate of the SAN.10
Internodal Conduction
For many years, there has been much controversy concerning the exis-tence of specialized conduction pathways connecting the SAN to the atrioventricular (AV) node. Most electrophysiologists now agree that preferential conduction is unequivocally present, and that spread of activation from the SAN to the AV node follows distinct routes by necessity because of the peculiar geometry of the right atrium.10
The orifices of the superior and inferior cavae, the fossa ovalis, and the ostium of the coronary sinus divide the right atrium into muscle bands, thus limiting the number of routes available for internodal con-duction (see Figure 4-1). These routes, however, do not represent dis-crete bundles of histologically specialized internodal tracts comparable with the ventricular bundle branches.22 It has been suggested that a
parallel arrangement of myocardial cells in bundles, such as the crista terminalis and the limbus of the fossa ovalis, may account for prefer-ential internodal conduction. Although electrical impulses travel more rapidly through these thick atrial muscle bundles, surgical transection will not block internodal conduction because alternate pathways of conduction through atrial muscle are available.23
Atrioventricular Junction and Intraventricular
Conduct ion System
The AV junction (Figure 4-2) corresponds anatomically to a group of discrete specialized cells, morphologically distinct from working myocardium and divided into a transitional cell zone, compact por-tion, and penetrating AV bundle (bundle of His).24 Based on animal
experiments, the transitional zone appears to connect atrial myocar-dium with the compact AV node.25 The compact portion of the AV
node is located superficially, anterior to the ostium of the coronary sinus above the insertion of the septal leaflet of the tricuspid valve. The longitudinal segment of the compact AV node penetrates the central fibrous body and becomes the bundle of His. As the nodal-bundle axis descends into the ventricular musculature, it gradually becomes com-pletely isolated by collagen and is no longer in contact with atrial fibers.
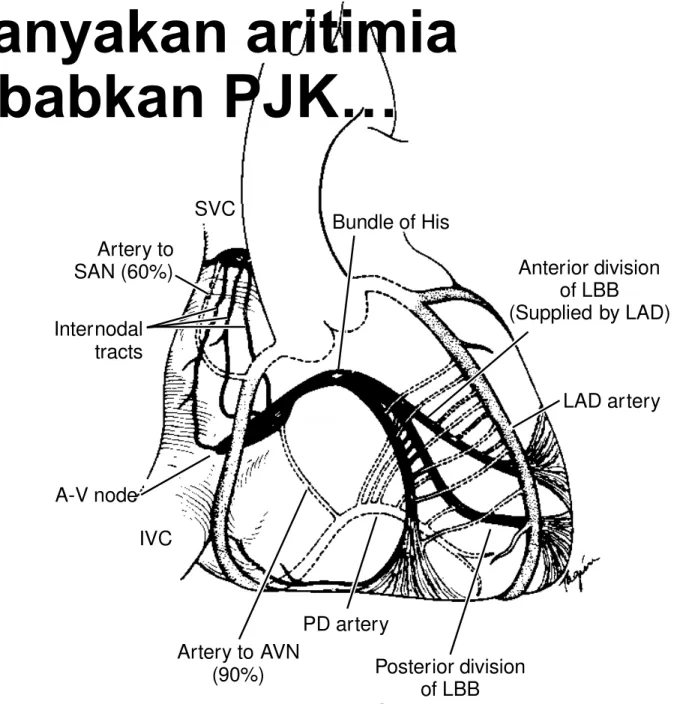
Artery to SAN (60%) SVC S-A node Bundle of His Internodal tracts AV node IVC TV RBB LBB Artery to AVN (90%) PD artery Posterior division of LBB (Supplied by PDA) Anterior division of LBB (Supplied by LAD) LAD artery
Figure 4-1 Drawing of t he anat omy of t he cardiac conduct ion sys-t em including arsys-t erial blood supply. In 60% of pasys-tiensys-ts sys-the sinoasys-trial (S-A) nodal artery is a branch of the right coronary artery, whereas in the remainder it arises from the circumflex artery. The atrioventricular node (AVN) is supplied by a branch from the right coronary artery or pos-terior descending artery. A-V, atrioventricular; IVC, inferior vena cava; LAD, left anterior descending coronary artery; LBB, left bundle branch; PD, posterior descending; PDA, posterior descending artery; RBB, right bundle branch; SAN, sinoatrial node; SVC, superior vena cava; TV, tri-cuspid valve. (From Harthorne JW, Pohost GM: Electrical therapy of car-diac arrhythmias. In Levine HJ [ed]: Clinical Cardiovascular Physiology.
New York: Grune & Stratton, 1976, p 854.)
BOX 4-1. ANATOM Y OF THE CARDIAC PACEM AKER AND CONDUCTION SYSTEM
5
Kebanyakan aritimia
disebabkan PJK…
1. PR interval
berhubungan
atrial
systole
2. Lebar QRS width
menunjukkan
waktu yang diperlukan untuk
mencapai “peak isovolumetric
contraction”
3. Sinkronisasi P
dengan
QRS
menjamin adekwasi waktu
ventricular filling
yang sinkron
dengan pembukan katub AV
6
Kaplan, J.A., Reich, D.L.,& Savino, J.S. 2011. Kaplan’s Cardiac Anesthesia. Missouri : Elsevier Saunders
Irama jantung
mempengaruhi
hemodinamik..
Irama jantung
mempengaruhi
hemodinamik..
•
↓ PR interval
↓ LVEDV
•
↑ QRS width
↓ tekanan yang
dihasilkan
•
Hilangnya regularitas atrial node
↓
LV filling
hampir
30%
(hilangnya atrial kick)
↓ SV
7
Kaplan, J.A., Reich, D.L.,& Savino, J.S. 2011. Kaplan’s Cardiac Anesthesia. Missouri : Elsevier Saunders
Irama Jantung dan DO
2
•
Gelombang U & P patologis
relaksasi LA
•
Asinkroni
gelombang P-QRS (AF) &
↓
PR interval
LV
filling
•
Lebar QRS
SV
8
Mekanisme
Aritmia
Mekanisme Aritmia Jantung
Gaztanaga L, Marchlinski FE, Betensky BP. Mechanism of cardiac arrhythmias Rev Esp Cardiol. 2012;65(2):174–185
Bradiaritmia
•
Disfungsi SA node
•
sinus bradycardia
•
sinus arrest
•
tachy-brady syndrome
(atau disebut juga sebagai sick
sinus syndrome), ketika bradiaritmia muncul bergantian
dengan atrial fibrilasi
•
Kegagalan penyebaran impuls merupakan manifestasi
heart block
pada AV node (AV block)
•
Seringkali disebabkan oleh PJK
•
Terapi : pacemaker
Disfungsi SA node
–
Sick Sinus
Syndrome
•
Disebut juga sindroma bradiaritmia – takiaritmia
•
Sinus bradikardia (biasanya < 40x/menit) diikuti AF
AV Blok derajat 1
AV Blok derajat 2
Tipe 1
AV Blok derajat 2
Tipe 2
AV Blok derajat 3
Pemanjangan PR interval
PR interval tidak konsisten, sesekali terdapat gelombang non konduksi
PR interval konsisten, sesekali terdapat gelombang non konduksi
Disosiasi gelombang P dengan QRS
Takiaritmia -
Automatisasi
•
Meningkatnya automatisasi bisa diakibatkan oleh gangguan
metabolik
•
Terjadi perubahan otot jantung yang semula tidak memilki sifat pacu
jantung menjadi fokus pacu jantung yang abnormal
•
Gangguan metabolik
yang berpotensi menyebabkan
automatisasi
•
Iskemia
•
Hipoksia
•
Hipokalemia
•
Hipomagnesemia
•
Gangguan asam-basa
•
Meningkatnya tonus simpatik
•
Obat-obatan simpatomimetik
Takiaritmia –
Triggered
Arrhythmia
“Triggered activity” adalah
aktivitas ritmis jantung yang
terjadi saat serangkaian osilasi
after-depolarization
mencapai
ambang batas
•
Delayed After Depolarization
(DAD) : fase 4
•
Intoksikasi digitalis, katekolamin,
anti aritmia (golongan IA)
•
Early After Depolarization (EAD)
: fase 2 dan 3
•
Anti aritmia gol. IA dan III
Supraventricular Tachycardia
(SVT)
Atrial Fibrilasi
RA
LV
RV
LA
SA Node
AV Node
N Engl J Med 2012;367:1438-48AF in some instances originates from
automatic foci in
the pulmonary veins
or
vena cava
and
that isolating these sites
may restore sinus rhythm
Haissaguerre M, Jais P, Shah DC, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med 339:659, 1998
Typical
Atrial flutter
Atypical
Atrial flutter
Tujuan terapi pada AF
•
Mengurangi risiko stroke
•
Antikoagulan
•
Kontrol “rate” & “rhytm” untuk mengurangi gejala klinis
•
Farmakoterapi
•
Kardioversi
•
Terapi intervensi
•
Operatif :
Maze I-IV
•
Ablasi
dengan kateter jantung
•
Kombinasi
•
Mengurangi risiko terjadinya “tachyarrhytmia
Pergeseran paradigma….
Ablasi menggunakan kateter jantung
•
Melvin Scheinman (1981)
•
Michelle Haissaguerre (1998)
Invasive heart surgery
minimally invasive surgery
James L. Cox (1997)
Ralph Damiano (2002)
Maze procedure I-IV
Limitasi terapi medikamentosa
•
kurang konsisten dalam
mempertahankan ritme sinus
Cox-Maze Procedure
Prinsip utama :
•
Memutus bagian elektrofisilogik yang
mengakibatkan AF (reentrant circuits)
sinus
rhythm
•
Mempertahankan konduksi SA nodal terhadap AV
nodal
menjaga sinkronisasi AV
•
Mempertahankan fungsi mekanik atrial (“atrial
kick”)
memperbaiki fungsi hemodinamik
Maze I
Maze II
Maze III
Ablasi pada AF..
•
Menantang
•
Tidak semua problem bisa diselesaikan
•
Angka kekambuhan tinggi (AVNRT,AVRT)
•
Diterapi dengan sekurang-kurangnya satu obat untuk
mengendalikan irama sebelumnya
•
”Symptomatic AF” tanpa penyakit jantung struktural
•
Dilatasi LA berat, persisten > 4 tahun – kemungkinan
berhasil rendah
•
RFA digunakan untuk isolasi elektri vena pulmonalis
•
Kontro indikasi : LA thrombus
Cardiac Mapping
•
Pemetaan aktivitas elektrik
jantung untuk mendapatkan
informasi elektroanatomi
jantung
•
Teknik mapping
•
Activation Mapping
•
Pace Mapping
•
Entrainment Mapping
•
Anatomic Localization
•
Electrogram Characteristics
•
Scar Mapping
Merah
scar (konduksi
sangat rendah)
Ungu
konduksi normal
http://what-when-how.com/cardiac-arrhythmias-new-considerations/electromagnetic-mapping-during-complex-rf-ablations-electrophysiology-study-of-the-heart-mapping-procedure-cardiac-arrhythmias-part-4/