1
Cervical Ossification of the Posterior Longitudinal Ligament:
Anterior or Posterior surgery
Akhm ad Im ron* )
Depart m ent of Neurosurgery Facult y of M edicine Padjadjaran Universit y Hasan Sadikin Hospit al Bandung, Indonesia
Object:
Ossificat ion of t he post erior longit udinal ligam ent (OPLL) is a com plex m ult ifact orial disease process com bining bot h m et abolic and biomechanical fact ors, m ost com m only found in m en, t he elderly and Asian pat ient s. There are m any diseases. There are m any diseases associat ed w it h OPLL, such as diffuse idiopat hic skelet al hyperost osis, ankylosing spondylit is, and ot her spondyloart hropat hies. Several fact ors have been report ed t o be associat ed w it h OPLL form at ion and progression, including genet ic, horm onal, environm ent al, and lifest yle fact ors. How ever, t he pat hogenesis of OPLL is still unclear. Plain radiography, CT, and M R im aging are used t o evaluat e OPLL ext ension and t he area of spinal cord com pression. M anagem ent of OPLL cont inues t o be cont roversial. Each surgical t echnique has som e advant ages and disadvant ages, and t he choice of operat ion should be m ade case by case, depending on t he pat ient ’s condit ion, level of pat hology, t ype of OPLL, and t he surgeon’s experience. In t his paper, t he aut hors at t em pt t o review t he incidence, pat hology, pat hogenesis, nat ural hist ory, clinical present at ion, classificat ion, radiological evaluat ion, and m anagem ent of OPLL.
M ethods:
The aut hors perform ed a ret rospect ive review of t heir inst it ut ional experience w it h surgical int ervent ion for cervical OPLL. They also review ed the English-language lit erat ure regarding t he epidemiology, pat hophysiology, nat ural hist ory, and surgical int ervent ion for OPLL.
Results:
Review of t he lit erat ure suggest s an im proved benefit for ant erior decom pression and st abilizat ion or post erior decom pression and st abilizat ion com pared w it h post erior decom pression via lam inect om y or lam inoplast y. Bot h ant erior and post erior approaches are safe and effect ive m eans of decom pression of cervical st enosis in t he set t ing of OPLL.
Conclusions:
2
Introduction
Ossificat ion of t he post erior longit udinal ligam ent is an im portant cause of cervical m yelopat hy that
result s from heterotopic ossificat ion of t he cervical or t horacic PLL. It has been estim ated t hat up t o 25% of patient s presenting wit h cervical m yelopat hy have feat ures of OPLL.1There has been consider- able debat e in recent years regarding t he opt imal surgi- cal approach for addressing t hese compressive lesions. Vent ral approaches consist of variat ions of t he cervical corpect omy, whereas dorsal approaches include a wide range of t echniques including laminoplast y, laminect o- my, and laminect omy wit h inst rument ed fusion. Wit h t he evolut ion of surgical t echnique and a great er underst and- ing of t he biomechanics of cervical deformit y, t he crit eria for select ing one approach over t he ot her has been t he subject of increased st udy.
Of t he many fact ors t o consider when deciding on eit her a dorsal or vent ral approach, t he degree of st eno- sis relat ed t o t he severit y of vent ral compression of t he spinal cord by t he ossified lesion is crit ical t o decision making as pat ient s wit h great er degrees of st enosis have hist orically shown less improvement following eit her dorsal or ventral surgery.4-6 In t his review, we discuss t he epidemiology,
nat ural history, and com mon radiographic findings associated wit h OPLL. The advant ages and disadvantages of current treatm ent options, including ant erior corpect omy, laminectomy, and laminoplast y are reviewed.
Patophysiology
The PLL (post erior longit udinal ligam ent ) ext ends f rom t he occiput t o t he sacrum along t he post erior aspect s of t he vert ebral bodies and t he dorsal aspect s of each int ervert ebral disc. As it becom es hypert rophied and ossifies, it result s in a significant rest rict ion of t he cervical canal diam et er. This com presses t he spinal cord and leads t o ischem ia and myelopat hy. In addit ion t o t his direct com pression, repeat ed im pact s of t he vent ral cord over t he hypert rophied and ossified ligam ent can f urt her lead t o dam age t o t he cord parenchym a.2 The pathogenesis of OPLL remains poorly under- st ood. There is som e evidence t hat ligament cells from pat ient s w it h OPLL have ost eoblast-like charact erist ics.3 Several fact ors have been report ed t o be associat ed w it h OPLL form at ion and progression, including genet ic, horm onal, environm ent al, and lifest yle fact ors. How ever, t he pat hogenesis of OPLL is st ill unclear.
Biomechanical Considerations
3 preexist ing deform it y im proves out - com es associat ed w it h OPLL, t here are ret rospect ive dat a indicat ing t hat pat ient s w ho undergo dorsal procedures w it hout inst rum ent at ion m ay w orsen neurologically as a result of progressive kyphosis.8 Wit h regard t o OPLL, t he presence of a com pressive lesion vent ral t o t he spinal cord increases t he risk of neurological det eriorat ion during any at t em pt at deform it y correct ion, part icularly if a dorsal procedure is planned. For t his reason, decom pression, w it h rat es of clinically significant kyphosis as high as 21%.6,10
If a kyphot ic deform it y is present , a flexion m oment is creat ed w it h t he head pit ched forw ard relat ive t o t he norm al alignm ent of t he cervical spine.2,3 This abnorm al post ure shift s t he norm ally neut ral axial force of t he head vent ral t o t he inst ant aneous axis of rot at ion, t hus creat ing a flexion bending m om ent . This leads t o furt her kyphosis..5 Thus, a vicious cycle of abnorm al forces and progressive deformit y is creat ed.2,3,6 If kyphosis becom es severe, t he spinal cord m ay st ret ch over t he apex of t he deform it y and lead t o furt her neurological decline.5
Pat hology
OPLL is believed t o form t hrough endochondral ossificat ion. M cAfee et al. described t he hist opat hology of OPLL, w hich is com posed largely of lam ellar bone w it h m at ure Haversian canals. Ult rast ruct ural st udy of t he ligam ent um flavum in pat ient s w it h OPLL revealed at rophic elast ic bundles w it h a 2-layer st ruct ure, disappearance of m icrofibrils, irregular alignm ent of collagen fibrils, and m any ext racellular plasm a m em brane-invest ed part icles t hat resem ble m at rix vesicles.
Pat hogenesis
The pat hogenesis of OPLL rem ains poorly under- st ood. There is some evidence t hat ligam ent cells from pat ient s w it h OPLL have ost eoblast-like charact erist ics. Ishida and Kaw ai41 st udied cell lines from nonossified sit es in pat ient s wit h OPLL and found t hat t hey have high alkaline phosphat ase act ivit y, response t o calcit onin, and calcit riol. Parat hyroid horm one and dinoprost one can also st im ulat e an increase in cyclic adenosine m onophos- phat e in t hese cell lines. There are m any proposed genet ic, horm onal, environm ent al, and lifest yle fact ors t hat relat e t o pat hogenesis and progression of OPLL, but m ost of t hese t heories are st ill cont roversial.
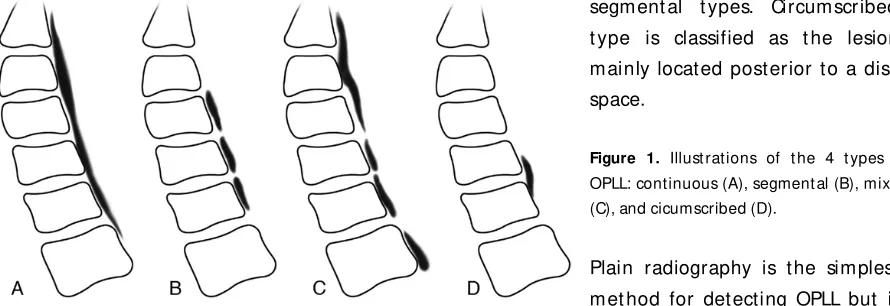
4 bodies. Segm ent al t ype is classified as one or several separat e lesions behind t he vert ebral bodies. M ixed t ype is classified as a com binat ion of cont inuous and segm ent al t ypes. Circum scribed t ype is classified as t he lesion m ainly locat ed post erior t o a disc space.
Clinical Presentation present w it h neurological deficit s such as radiculopat hy, myelopat hy, and in severe cases, bowel and bladder sym pt om s. The onset of sym pt oms is usually gradual, but t here are also some report s of pat ient s w it h t raum a-induced sudden onset myelopat hy.
5
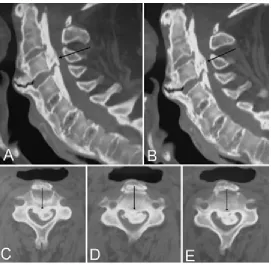
Figure 2. Computed t omography scans show ing OPLL in different locat ions.
On M R im aging, early OPLL appears dorsal t o t he int erspaces and can be seen on axial and sagit t al views. As t he disease progresses, t he dense signal behind t he vert ebral bodies and int erbody spaces becom es hypoint ense on all M R im aging sequences. However, in t he progressed disease, t here are sm aller areas of increased signal. These areas are indicat ive of new bone form at ion w it hin t he ligam ent. In addit ion, OPLL does not enhance w it h Gd. Thus, on enhanced M R im ages, it is possible t o different iat e bet ween a hypert rophied ligam ent and post operat ive scarring. Associat ed changes in t he spinal cord m ay be seen on T2-weight ed im aging in associat ion w it h OPLL. This includes areas of increased T2-signal associat ed w it h cord edem a.
Radiographic Criteria for Approach Selection
The criteria used to select either a dorsal or ventral approach should be based on a number of factors including patient age, comorbidities, severity of symptoms, previous surgery, type of OPLL, extent of OPLL, degree of stenosis, surgeon preference, and assessment of cervical deformity.
Various radiographic schemes have been proposed to help select the best approach for patients with cervical myelopathy. Gwinn et al.14 proposed a simple straight-line method to measure effective spinal canal lordosis in patients with cervical myelopathy. In this scheme, a straight line is drawn from the dorsal-caudal aspect of the C-2 VB to the dorsal-caudal aspect of the C-7 VB (Fig. 1). Effective lordosis is maintained if no ventral bone structure such as VBs, disc-osteophyte complexes, or hypertrophic
6 determining the best surgical approach as ventral surgery may better achieve decompression in these patients. In 2008, Fujiyoshi et al. proposed a new concept for decision making regarding the surgical approach for cervical OPLL. They introduced a new index called the K-line to help determine the effectiveness of a dorsal approach. This line was defined as a line on a lateral radiograph drawn between the midpoints of the spinal canal at C-2 and C-7. According to this line, 2 groups of patients with OPLL were identified. In the K-line (+) group, the OPLL lies ventral to the K-line. In the K-line (-) group, the OPLL passes the line and lies dorsal to the line. In their series, 27 patients with myelopathy as a result of
OPLL underwent either laminoplasty or laminectomy with instrumented fusion. Intraoperative ultrasonography was also used to evaluate the dorsal shift of the spinal cord from t he OPLL. The relationship between the dorsal shift of the spinal cord and the K-line classification was made. Clinical outcomes were assessed using the JOA scores before surgery and at 1 year after surgery.
Fig. 1. In this digital radiograph, the line drawn from the dorsal cau- dal aspect of C-2 to the dorsal caudal aspect of C-7 is used as a ref- erence to measure effective cervical lordosis. In this image, effective spinal canal lordosis is maintained, as no bone from the VBs or disc space is projecting dorsal to the line.
Overall, statistically significant improvement in JOA scores was found in the K-line (+) group. Complications and neurological worsening were not reported. Based on these findings, Fujiyoshi et al. proposed that patients with cervical OPLL that extend dorsal to the K-line have a better chance for neurological improvement with a ven- tral approach, but no patients were studied to support this recommendation. Based on their outcomes and correla- tion with intraoperative ultrasound, it is their assertion that K-line (-) patients have kyphosis that prohibits a dor- sal approach as the spinal cord has less potential to shift following decompression.
M anagement
Nonoperat ive m anagement of OPLL.
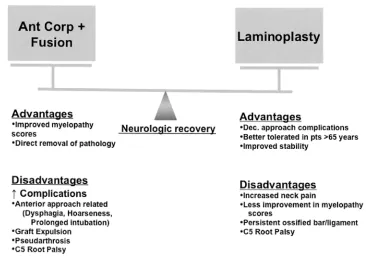
7 or for t hose whose overall m edical healt h precludes t hem f rom surgical t reat m ent. Pharm acological pain m anagement w it h t he guidance of m ult idisciplinary pain specialist s is recom m ended. Nonst eroidal ant iinflam m at ory m edicat ions and st eroid inject ions are t he m ainst ays of nonoperat ive t herapy. Unfort unat ely, despit e t he inflam m at ory nat ure of t he disease, t here have been few pharm acological advances in t he specific ant iinflam m at ory agent s designed for OPLL, as com pared w it h ot her inflam mat ory disease such as rheum at oid art hrit is or ankylosing spondylit is. The m ost com mon locat ion of OPLL is at t he cervical spine. There are several report s of surgical m anagem ent of cervical OPLL w it h opt ions including t he post erior approach (lam inect omy, lam inect omy wit h f usion, lam inoplast y, and open-door and double-door lam inoplast y), t he ant erior approach (ACDF, ant erior cervical corpect omy w it h f usion, open-window corpect omy, oblique corpect omy, skip corpect omy, and ant erior decom pression via a t rans- vert ebral approach), and t he com bined ant erior and post erior approach. The advant ages and disadvant ages of each approach are sum m arized in Figure 3.
Figure 3. Advant ages and disadvant ages of ant erior versus posterior t echniques for decompression in OPLL.10
Surgical M anagement of OPLL
Pat ient s w it h OPLL com m only present w it h sym p-t om s in t heir 40s or 50s. This comm only begins wit h sym pt om s of num bness or axial neck pain. Wit hout surgi-cal decom pression, sym pt om atic OPLL t ends t o progress w it h t im e. In a long-term follow -up st udy, M at sunaga et al. dem onstrat ed t hat 38% of pat ient s present ing wit h baseline m yelopat hy had progressive w orsening of t heir sym pt om s. Ossificat ion of t he PLL has been addit ion-ally found t o progress follow ing decom pression as w ell as during rout ine radiographic follow-up in t he pat ient in w hom decom pression has not been performed. For t hese reasons, especially for younger patient s wit hout es-t ablished deficit s, it is our pract ice t o obt ain strict radio-graphic follow -up. In pat ient s wit h progressive deficit s, including severe weakness or m yelopat hy, surgery is con-sidered. Like ot her authors, w e believe t hat older pat ient s wit h significant com orbid conditions and severe, long-st anding deficit s m ay be poor surgical candidat es.10
8 aft er a successful post erior decompression. Furt hermore, clinical myelopat hy scores have been show n t o improve most significant ly wit h ACC. Several st udies have show n bet t er out com es follow ing ant erior rat her t han post erior decompression for OPLL.7 Fessler et al.8 found t hat pat ient s t reat ed by an ant erior approach had an average improvem ent of 1.24 Nurick grades when compared w it h lam inect omy pat ient s who only improved by 0.07. In addit ion, lam inect omy and fusion or lam inoplast y is not appropriat e in pat ient s w it h poorly preserved cervical lordosis.
Posterior Cervical Approaches
Cervical lam inect omy and decompression can of t en be augm ent ed by lat eral m ass fusion t o correct inst abilit y or t o prevent loss of fut ure sagit t al alignm ent. Lam inoplast y is also offered as an alternat ive t o lat eral m ass fusion. In pat ient s undergoing post erior decompression surgery, t here should be evidence of preoperat ive cervical lordosis of at least 10° and less t han 7 m m of ant erior-post erior OPLL for indirect decompression t o be successful.9 The most significant advantage of a posterior approach is t hat it avoids t he pot ent ial soft-t issue complicat ions of t he ant erior approach. Furt hermore, t here is no risk of graft ext rusion, but t here is a decreased incidence of post operat ive pseudart hrosis. However, post erior decompression should be avoided in pat ient s wit h a kyphot ic alignm ent, spondylolist hesis, suggest ed inst abilit y, or high disc spaces.
Conclusion
OPLL is a com m on cause of myelopat hy in Asian populat ions. W hile t he pat hogenesis of t his disease is st ill unclear, genet ic, horm onal, environm ent al, and life- st yle fact ors are believed t o cause OPLL form at ion and progression. Occurrence of myelopat hy in pat ient s w it h OPLL is relat ed t o bot h st at ic and dynam ic fact ors. Radiological evaluat ion of OPLL includes plain radiography, CT, and M R imaging. Surgical m anagement of OPLL rem ains cont roversial; each approach has it s ow n lim it at ions, advant ages, and disadvant ages. The choice of operat ion should be m ade on a case by case basis, depending on t he pat ient’s condit ion, level of pat hology, and t ype of OPLL, as well as t he experience of t he surgeon.
3. Ishida Y, Kawai S: Ef fect s of bone-seeking horm ones on DNA synt hesis, cyclic AM P level, and alkaline phosphat ase act ivit y in cult ured cells f rom hum an post erior longit udinal ligam ent of t he spine. J Bone M iner Res 8:1291–1300, 1993
9 on it s biology, epidem iology, and nat ural hist ory. Neurosurgery 58:1027–1039, 2006
5. Chen Y, Guo Y, Chen D, Lu X, Wang X, Tian H, et al: Diagnosis and surgery of ossificat ion of post erior longit udinal ligament associat ed w it h dural ossificat ion in t he cervical spine. Eur Spine J 18:1541–1547, 2009
6. Soo M Y, Rajarat nam S: Sym pt om at ic ossificat ion of t he post erior longit udinal ligament of t he cervical spine: pict orial essay. AustralasRadiol 44:14–18, 2000
7. Iwasaki M , Okuda S, M iyauchi A, Sakaura H, M ukai Y, Yonenobu K, et al: Surgical st rat egy for cervical myelopat hy due t o ossificat ion of t he post erior longit udinal ligament : Part 2: Advant ages of ant erior decom pression and f usion over lam inoplast y. Spine 32:654–660, 2007
8. Fessler RG, St eck JC, Giovanini M A: Ant erior cervical corpect omy for cervical spondylot ic myelopat hy. Neurosurgery43:257–267, 1998
9. Yam azaki A, Hom m a T, Uchiyam a S, Kat sum i Y, Okum ura H: M orphologic lim it at ions of post erior decom pression by m idsagit t al split t ing m et hod for myelopat hy caused by ossificat ion of t he post erior longit udinal ligament in t he cervical spine. Spine 24:32–34, 1999 10. Sm it h ZA, Buchanan CC, Raphael PA, Khod LT. Ossificat ion of t he post erior longit udinal