Background
the increase of child mortality in developing country,
the high incidence of serious bacterial infection in
children,
the variety of risk factors of serious infections,
current scoring model has not been tested in limited
Background……
In clinical practice, discriminating children with SBI
from those with other self limiting infections is challenging.
A simple, validated clinical tool to risk stratify and
guide further management of children with suspected SBI would greatly improve their care.
Objective.
to know the validity of of Royal College of Paediatrics
and Child Health Score (SBI score) to predict serious bacterial infection in children with fever and
Validity of SBI score in different cut off point
Validity of SBI score based on age category
Method
.
Diagnostic study was used to find validity of RCPCH
Score and cohort prospective study to find predictor factors of the serious infection.
Gold standard was the latest diagnosis noted on
medical record based on ICD-10.
Sample Population : febrile children 1 months-12
years old who was come to emergency department and policlinic Sanglah Hospital that eligible for inclusion and exclusion criteria.
Convenient sampling
Inclusion criteria :
1. Febrile children less than 7 days,
2. Come first time for that febrile episode and
accompanied by parents,
3. Parents agree to joint in this study.
Exclusion criteria
:
•
Febrile children with emergency condition,
•
Parent didn’t have hand phone or home
Statistical Methods :
Analysis were performed using computer
Sensitivity, specificity, positive predictive value, negative predictive value, positive likelihood rasio, negative
likelihood rasio, post test probability, area under ROC curve were reported
Logistic regression were performed to find predictor factor for SBI
Results
There were 260 subjects. Seven patients of out-patient
department could not be reached so analysis was done on 253 subjects (97.3%).
There were more male than female with the ratio of
1.14:1.
Age group of >36 months dominated the subject
population (51.4%).
Serious bacterial infection was found on 28.9% subject
Variable Status of patients (n, %)
Hospitalized Procalsitonin, n = 24 (n, mean)
SBI
Diagnosis n (%) SBI
Acute Otitis Media Empiema
Pneumonia
Diarrhea by bacterial infection Sepsis
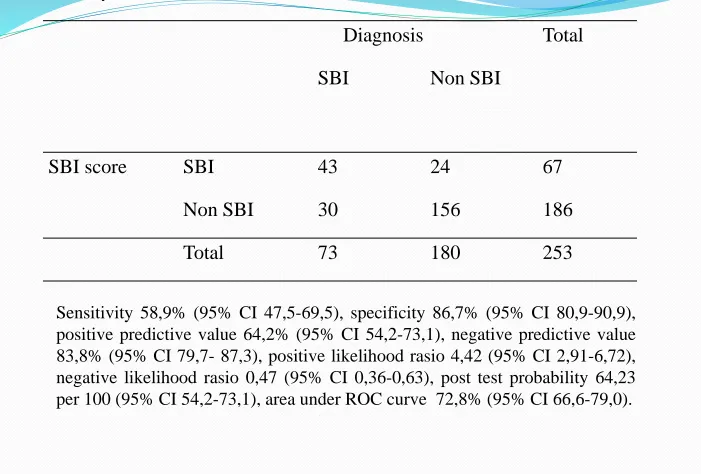
Diagnosis Total SBI Non SBI
SBI score SBI 43 24 67 Non SBI 30 156 186 Total 73 180 253
Sensitivity 58,9% (95% CI 47,5-69,5), specificity 86,7% (95% CI 80,9-90,9), positive predictive value 64,2% (95% CI 54,2-73,1), negative predictive value 83,8% (95% CI 79,7- 87,3), positive likelihood rasio 4,42 (95% CI 2,91-6,72), negative likelihood rasio 0,47 (95% CI 0,36-0,63), post test probability 64,23 per 100 (95% CI 54,2-73,1), area under ROC curve 72,8% (95% CI 66,6-79,0).
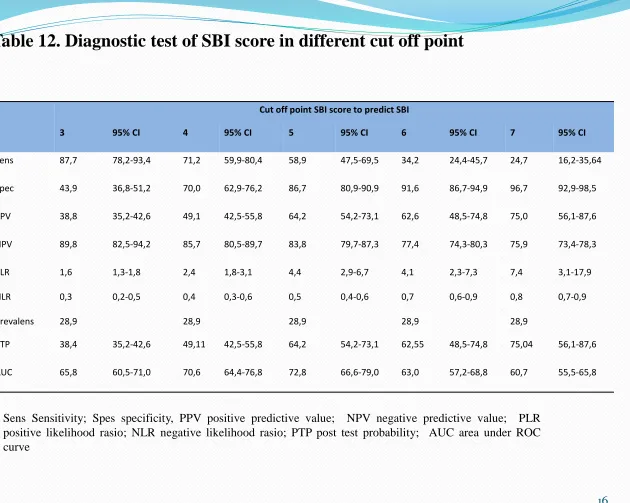
Cut off point SBI score to predict SBI
3 95% CI 4 95% CI 5 95% CI 6 95% CI 7 95% CI
Sens 87,7 78,2-93,4 71,2 59,9-80,4 58,9 47,5-69,5 34,2 24,4-45,7 24,7 16,2-35,64 Spec 43,9 36,8-51,2 70,0 62,9-76,2 86,7 80,9-90,9 91,6 86,7-94,9 96,7 92,9-98,5 PPV 38,8 35,2-42,6 49,1 42,5-55,8 64,2 54,2-73,1 62,6 48,5-74,8 75,0 56,1-87,6 NPV 89,8 82,5-94,2 85,7 80,5-89,7 83,8 79,7-87,3 77,4 74,3-80,3 75,9 73,4-78,3 PLR 1,6 1,3-1,8 2,4 1,8-3,1 4,4 2,9-6,7 4,1 2,3-7,3 7,4 3,1-17,9 NLR 0,3 0,2-0,5 0,4 0,3-0,6 0,5 0,4-0,6 0,7 0,6-0,9 0,8 0,7-0,9 Prevalens 28,9 28,9 28,9 28,9 28,9
PTP 38,4 35,2-42,6 49,11 42,5-55,8 64,2 54,2-73,1 62,55 48,5-74,8 75,04 56,1-87,6 AUC 65,8 60,5-71,0 70,6 64,4-76,8 72,8 66,6-79,0 63,0 57,2-68,8 60,7 55,5-65,8
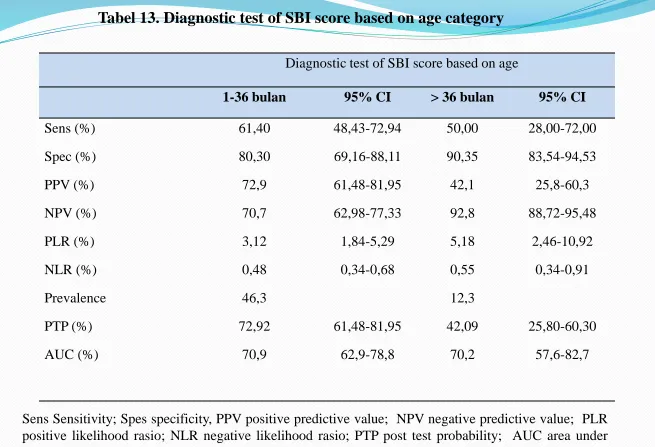
Diagnostic test of SBI score based on age
1-36 bulan 95% CI > 36 bulan 95% CI
Sens (%) 61,40 48,43-72,94 50,00 28,00-72,00
Spec (%) 80,30 69,16-88,11 90,35 83,54-94,53
PPV (%) 72,9 61,48-81,95 42,1 25,8-60,3
NPV (%) 70,7 62,98-77,33 92,8 88,72-95,48
PLR (%) 3,12 1,84-5,29 5,18 2,46-10,92
NLR (%) 0,48 0,34-0,68 0,55 0,34-0,91
Prevalence 46,3 12,3
PTP (%) 72,92 61,48-81,95 42,09 25,80-60,30
AUC (%) 70,9 62,9-78,8 70,2 57,6-82,7
Sens Sensitivity; Spes specificity, PPV positive predictive value; NPV negative predictive value; PLR positive likelihood rasio; NLR negative likelihood rasio; PTP post test probability; AUC area under
No Variable SBI Non SBI p OR 95%CI 3 Duration of fever
(n,median)
73 4,09 180 4,18 0,624**
4 Cough 52 52,0 48 48,0 0,001 6,8 3,7 12,5 5 Rhinorrhea 41 48,8 43 51,2 0,001 4,1 2,3 7,3 6 Breathing difficulty 44 74,6 15 25,4 0,001 16,5 8,2 33,6 7 Diarrhea 10 41,7 14 58,3 0,149 1,9 0,8 4,4 8 Convulsion 2 6,5 29 93,5 0,003* 6,8 1,6 29,4 9 Unconsciousness 6 20,0 24 80,0 0,254 1,1 0,9 1,4 10 Dysuria 0 0 2 100,0 1,000* 1,4 1,3 1,5 11 Development delay 4 50,0 4 50,0 0,233* 2,6 0,6 10,5 12 Risk of infection 32 32,3 67 67,7 0,329 1,3 0,8 2,3 13 State variation
Eye closed 23 46,0 27 54,0 0,003 2,6 1,3 4,9 14 Temperature≥37,5 71 35,7 128 64,3 0,001 14,4 3,4 60,9
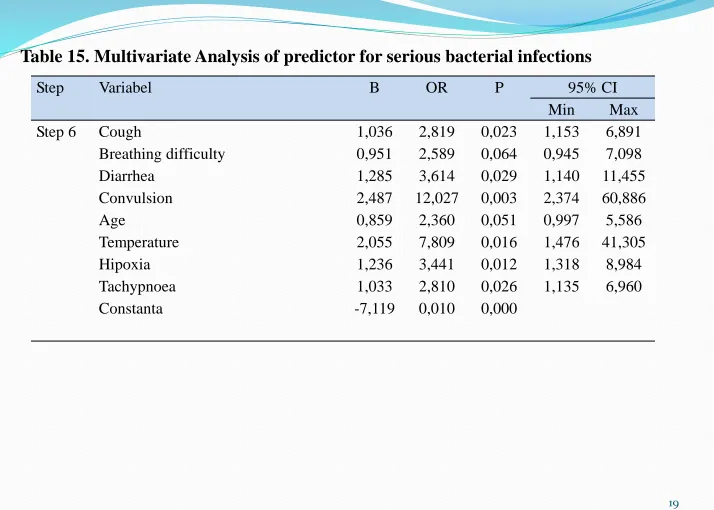
Step Variabel B OR P 95% CI Min Max Step 6 Cough 1,036 2,819 0,023 1,153 6,891
Breathing difficulty 0,951 2,589 0,064 0,945 7,098 Diarrhea 1,285 3,614 0,029 1,140 11,455 Convulsion 2,487 12,027 0,003 2,374 60,886 Age 0,859 2,360 0,051 0,997 5,586 Temperature 2,055 7,809 0,016 1,476 41,305 Hipoxia 1,236 3,441 0,012 1,318 8,984 Tachypnoea 1,033 2,810 0,026 1,135 6,960 Constanta -7,119 0,010 0,000
DISCUSSION
Clinical scoring model to predict SBI in children was less
reported.
Brent et al demonstrates the potential utility of a clinical score in risk stratifying children with suspected SBI Royal
College of Paediatrics and Child Health score (SBI score)
Validation of this score in different setting has not been reported.
•Brent AJ, Lakhanpaul M, Thompson M, Collier J, Ray S, Ninis N, et al. Risk score to stratify children with suspected serious bacterial infection: observational cohort study Arch Dis Child. 2011;96: 361–367.
SCREENING TOOL
Sensitivity
Likelihood ratio
Low sensitivity was not good for screening
Positive LR 4,42 ( 95% CI 2,91- 6,72) : small
change from pre-test probability to post-test
probability.
This study :
• Sensitivity 58,9% and specificity 86,7% • PPV 64,2% and NPV 83,8%
• Positive LR 4,42 and negative LR 0,47
………….VALIDITY of SBI score
Other component : post-test probability.
In this study :
post-test probability 64,23%, we can used this score
Risk factor Analysis for SBI
Clinical symptoms and signs as predictor of SBI has
been reported by many study with different result.
Hsiao et al16 find age and height of fever were not
significant predictor of SBI. White blood cell count and CRP were elevated in infant with SBI.
Risk factor analysis
for SBI …………..
Trautner et al
, child less than 18 years old who come to emergency department with hyperpirexia , risk for SBI : age < 36months, chronic illness, diarrhea, fever more than 48 hours, absolute neutrophil count ≥ x 3 sel/mm3.
Opiyo et al
, systematic review, among sick infants aged 0–59 days, the most valuable in identifying infants at risk of severe illness : history of feeding difficulty, history of convulsions, temperatureaxillary ≥3 . °C or <35.5°C, change in level of activity, fast
breathing/respiratory rate ≥ bpm, severe chest indrawing, grunting, and cyanosis
………….Validity of SBI Score
………….VALIDITAS SKOR IBS
This study :
Risk factor for SBI : cough, breathing difficulty,
diarrhea, convulsion, age 1-36 months, temperature≥
Conclusion
RCPCH Score can used to predict serious bacterial
infection in children aged 1 month- 12 years.
Cough, dyspnea, diarrhea, seizure, age of 1-36 months,
body temperature ≥ 3 . 0 C, hypoxia, and tachypnea