Review Article
iju_2963416..428Transumbilical laparoendoscopic single-site surgery
in urology
John E Humphrey and David Canes
Department of Urology, Tufts University School of Medicine, Lahey Clinic Institute of Urology, Burlington, Massachusetts, USA
Abbreviations & Acronyms CL=conventional
laparoscopy
DVT/PE=deep venous thrombosis/pulmonary embolus
EBL=estimated blood loss E-NOTES=embryonic natural orifice
transumbilical endoscopic surgery
Lap=laparoscopic LESS=laparoendoscopic single-site surgery LOS=length of hospital stay
MAG3=technetium-99m mercaptoacetyltriglycine MOT=mean operative time
OPUS=one port umbilical surgery
SIL=single incision laparoscopy SILS=single port laparoscopy
SPA=single port access SPL=single port laparoscopy
Correspondence:David Canes
M.D., Department of Urology, Tufts University School of Medicine, Lahey Clinic Institute of Urology, 41 Mall Road , Burlington, MA 01805, USA. Email: [email protected]
Received 18 October 2011; accepted 4 January 2012. Online publication 15 February 2012
Abstract: Laparoendoscopic single-site surgery has seen a dramatic rise in the uro-logical community. With the advent of new techniques and instrumentation, laparoen-doscopic single-site surgery has become more accessible for a wide variety of applications. The majority have been carried out through a transumbilical incision in order to effectively hide the scar within the umbilicus. Here, we review the history and clinical applications for transumbilical laparoendoscopic single-site surgery within urology. The current scope is broad , and great strides have been made, but the overall benefit appears to be predominantly cosmetic. Diffusion of laparoendoscopic single-site surgery techniques from tertiary referral centers to the community urologist remains unknown. This review demonstrates the feasibility of transumbilical laparoendoscopic single-site surgery as shown in the urological literature.
Key words: laparoendoscopic single-site surgery, minimally invasive, review, transumbilical.
Introduction
Rise of minimally invasive surgery
Single-port surgery, like many advances in medicine, is the result of constant fine-tuning of prior techniques, and questioning how they can be improved on. The initial impetus driving towards minimally invasive surgery was the morbidity from an open laparotomy incision. The pain, recovery time and inherent wound complications, such as infection and incisional hernias, as well as the cosmetic nature of open surgery drove us to push the field towards laparoscopic surgery, and subsequently its robotic counterpart. The subsequent evolution of technique, ability and technology has led to the development of transumbilical single-port surgery. This is thought to be the next natural step in accomplishing safe, effective proce-dures while limiting the morbidity and cosmetic consequences of large and/or several incisions.
Assumptions that surgical morbidity is simply linearly related to the sum-total of incision length(s), however, have not held under scrutiny in the past. The present review is focused on the urological experience with single-port surgery specifically using a transumbilical approach. The umbilicus provides a location in which the resultant scar can be at least partially hidden from view, enhancing the benefit of improved cosmesis with single-port surgery. The application of transumbilical single-port surgery in urology is ever growing, and herein we describe the worldwide use of this technique to date.
The term now used to describe single-port surgery in the urological literature is LESS. This was developed to incorporate and standardize the various previous terms used to describe one overall concept of minimally invasive operations performed through a single incision using conventional laparoscopic or newer instrumentation such as fixed pre-bent or
deflectable flexible instruments.1 Previous terms included E-NOTES, SILS, OPUS, SPA,
SPL and SIL, among others. The first transumbilical urological LESS procedure described
was by Raman et al. where three nephrectomies were carried out, each using a single
incision with multiple trocars.2 Since that time, the clinical experience has increased
bs_bs_banner
International Journal of Urology (2012)19, 416–428 doi: 10.1111/j.1442-2042.2012.02963.x
dramatically and LESS has cemented itself as an excellent technique for a broad range of urological procedures.
Early history
The first description of a true LESS procedure, evident now only in retrospect, was in the field of gynecology for tubal
ligation in 1972.3A 1-cm infraumbilical incision was made,
through which a laparoscope was inserted to visualize and then cauterize each fallopian tube. The fallopian tubes were exposed using an external tenaculum placed on the uterus from the vagina. The cosmetic benefit of the technique was immediately evident, and eventually led gynecologists to explore similar techniques for larger procedures, including total abdominal hysterectomy and bilateral
salpingo-oophorectomy by 1991.4
General surgeons also began to explore the use of transumbilical LESS surgery for appendectomy and
cholecystectomy.5–7 During this process, a new technique
was developed in 1999 for use in cholecystectomy, by which a single skin incision is made, but two fascial incisions are used to accommodate 5-mm trocars within this common
skin incision.8 This allows more ports for instruments
without compromising the cosmetic benefit.
Initial urological applications
Although LESS procedures were being developed in these other arenas, the evolution from open to laparoscopic and finally robotic surgery was taking place in urology. The benefits realized during this transition included less bleed-ing, fewer complications and shorter hospital stays leading
to faster convalescence.9 It was thus inevitable that
urolo-gists would also begin exploring the single-port system. Although we focus here on transumbilical LESS, in 2007, the first case in urology used a flank incision for placement of an R-port (Advanced Surgical Concepts, Wicklow, Ireland) to complete a nephrectomy on a small,
non-functioning kidney.10 This technique has also been
used for radical nephrectomy with a 7-cm paramedian inci-sion just lateral to the rectus muscle for placement of a GelPort (Applied Medical, Rancho Santa Margarita, CA,
USA).11Another case report described a 4-cm flank
inci-sion with a GelPort to carry out retroperitoneal radical
nephrectomy for renal cell carcinoma in a dialysis patient.12
The pfannenstiel incision has also been explored as a focal point for LESS. In one report, a 7.5-cm pfannenstiel inci-sion was used to carry out both nephrectomy and
neph-roureterectomy, using a GelPort as an access device.13
These approaches proved to be feasible options utilizing non-umbilical incisions. However, the majority of urologi-cal single-site experience, as described here, has been with transumbilical access.
Benefits of LESS
The transition from CL to LESS creates inherent technical challenges. In order for the urological community at large to embrace LESS, clear benefits of LESS over CL must be shown rigorously and scientifically. This has been difficult, as the salient advantage is improved cosmesis, a variable for which there is a paucity of objective measures. An early comparison between LESS and CL among patients under-going nephrectomy showed a subjective cosmetic advan-tage, while also showing comparable outcomes for operative
time, analgesic use, hospital stay and complication rate.14
Similar subjective outcomes have been reproduced with
various procedures,15–18but a recent study by Parket al.used
an objective measure to quantify the cosmetic advantage.19
This group used a body image questionnaire to compare patient satisfaction after kidney surgery. Although the scale was non-validated , it does represent the first objective measure of improved cosmesis with LESS. As rigorous data continues to accumulate, by preliminary observation it seems clear that at least from the surgeon’s perspective, cosmesis is excellent after umbilical LESS surgery. Figure 1 shows the immediate intraoperative cosmetic result of a patient in our own group undergoing a LESS left renal cyst decortication. For this procedure, a 4-cm vertical intraum-bilical incision was made, with the result as shown at 6 weeks postoperatively in Figure 2.
Other theoretical benefits of LESS include decreased postoperative pain and fewer postoperative wound
compli-cations (infection, hernia). Jeong et al. presented data
among patients undergoing adrenalectomy (9 LESS, 17 CL) showing significantly lower postoperative pain in the LESS
cohort.17 However, most comparison series have not had
long enough follow up or were powered with sample sizes necessary to show a meaningful difference in wound complications.
Fig. 1 LESS renal cyst decortication immediate cosmetic
result.
Transumbilical LESS in urology
Technique and instruments
As with any new surgical platform, LESS has been associ-ated with unique ergonomic challenges to overcome and inherent difficulties, which continue to be present. Multiport laparoscopic surgery with strategically placed trocars achieves triangulation for improved tissue retraction and only rare instrument clashing. Triangulation and instrument crowding becomes even more difficult during LESS, whereby bulky instrument handles clash in preciously limited external “real estate”. These difficulties have put the onus not only on the surgeon to creatively overcome these limitations given current instruments, but also on industry to design purpose-built access devices and instrumentation. The technical and equipment challenges with LESS have
previously been described by Sawyer and Ponsky.20They
note the rapid innovation seen with LESS and highlight the obstacles that are inherent to single-port surgery. Two approaches are described: (i) a coaxial approach in which instruments are used in parallel; or (ii) a novel platform. The coaxial approach leads to limited visual perspective, as instruments are in line with the operator’s vision. The tran-sition to novel platforms to overcome this challenge is described below.
Before the current devices were created , surgeons first experimented by using existing laparoscopic instruments through a single skin incision and multiple fascial incisions. This “keyhole” technique (as described above as the first urological transumbilical LESS procedure) was used to complete three nephrectomies (two for chronic infection, one for a 4.5-cm enhancing renal mass) with three adjacent
trocars in an umbilical incision.2Articulating graspers,
stan-dard endoshears and a 45° 5-mm rigid laparoscope or 5-mm deflectable tip laparoscope were used. The authors cited internal and external instrument collision as a constant chal-lenge, as well as a difficult learning curve. Similarly,
adrena-lectomy has been carried out using a 2-cm incision with
adjacent trocars through multiple fascial punctures.21The
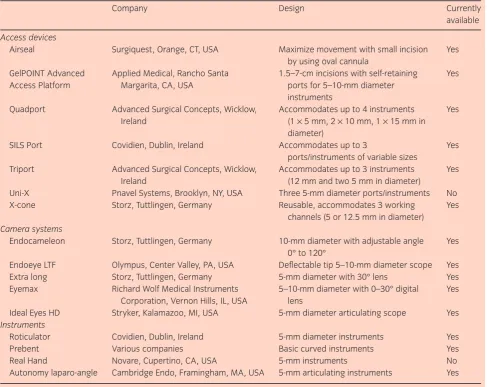
fascial incisions were connected in these cases for specimen extraction. The three challenges noted were limited maneu-verability with tearing of port site fascia, difficult visualiza-tion and potential difficulty with vascular control. In order to meet these challenges, new access platforms were created that depended on only one fascial incision with the potential to accommodate up to three or four instruments at a time (such as with Triport and QuadPort; Advanced Surgical Concepts). The main concept behind new platforms is to provide access for multiple instruments through one incision while limiting device profile. One solution is provided by the GelPOINT Advanced Access Platform (Applied Medical), which allows the surgeon to place multiple trocars through any location in the device. Table 1 shows current access devices and instrumentation for LESS procedures. Figure 3 shows an intraoperative view of the GelPOINT Advanced Access Platform being used for the aforementioned LESS left renal cyst decortication.
One notable addition is that of mini-laparoscopic or needlescopic instruments, which have been and continue to be used as adjuncts during LESS procedures. For certain procedures, in addition to the transumbilical single-port, a small 2- or 3-mm port has been used for a retracting device, requiring no skin suturing and virtually no scar. This adjunct was embraced as a way to bridge the gap between standard laparoscopy and LESS in the consensus statement on LESS
in 2010.22
Applications
As described earlier, nephrectomy was the initial procedure reported for transumbilical LESS in 2007. Since that time in only 4 years, an impressive array of procedures have been successfully completed using a transumbilical LESS approach, spanning almost the full urological surgical arma-mentarium for intra-abdominal procedures. We summarize the literature here, including only those procedures
com-Fig. 2 Cosmetic result 6 weeks after LESS renal cyst
decortication.
Fig. 3 GelPOINT Advanced Access Platform intraoperatively.
JE HUMPHREY AND D CANES
pleted through the umbilicus. We have extracted such data from series in which multiple techniques and access sites were included. As the literature is ever growing, this is not intended to be a comprehensive summary. We hope to give the reader the current scope of the clinical applications utilizing transumbilical LESS. Currently-reported transum-bilical LESS applications by organ systems are detailed below.
Kidney
Raman first described nephrectomy using three trocars
through a single umbilical incision.2 Kidney surgery
com-prises the majority of transumbilical LESS surgery to date. It is therefore instructive to subdivide kidney procedures into the following categories: oncology, reconstructive, donor nephrectomy and other. Oncological procedures with
a LESS approach must be able to be completed without compromising cancer outcomes. This began by demonstra-tion of renal mass cryoablademonstra-tion using a 3.8-mm cryoprobe (Endocare, Irvine, CA, USA) through a Uni-X access
device.23The authors described this method with both
tran-sumbilical and retroperitoneal approaches. The utility of this method was confirmed later in a review of a single-center’s
transumbilical LESS experience.24
Extirpative oncological surgery has also been shown to be
feasible. Aronet al. reported five partial nephrectomies in
200825using the R-Port access device. An extra 2-mm port
was used for a grasper, and one patient needed an additional 5-mm port for liver retraction. The R-Port was again used when carried out on six patients in an overall review of
several LESS procedures by Desai.26 Other devices have
been used for partial nephrectomy including the Uni-X27and
GelPort,28as well as standard trocars through a single
inci-Table 1 Current devices and instrumentation for LESS (alphabetical order)
Company Design Currently
available
Access devices
Airseal Surgiquest, Orange, CT, USA Maximize movement with small incision by using oval cannula
Yes
GelPOINT Advanced Access Platform
Applied Medical, Rancho Santa Margarita, CA, USA
1.5–7-cm incisions with self-retaining ports for 5–10-mm diameter instruments
Yes
Quadport Advanced Surgical Concepts, Wicklow, Ireland
Accommodates up to 4 instruments (1¥5 mm, 2¥10 mm, 1¥15 mm in
diameter)
Yes
SILS Port Covidien, Dublin, Ireland Accommodates up to 3
ports/instruments of variable sizes
Yes
Triport Advanced Surgical Concepts, Wicklow, Ireland
Accommodates up to 3 instruments (12 mm and two 5 mm in diameter)
Yes
Uni-X Pnavel Systems, Brooklyn, NY, USA Three 5-mm diameter ports/instruments No X-cone Storz, Tuttlingen, Germany Reusable, accommodates 3 working
channels (5 or 12.5 mm in diameter)
Yes
Camera systems
Endocameleon Storz, Tuttlingen, Germany 10-mm diameter with adjustable angle 0° to 120°
Yes
Endoeye LTF Olympus, Center Valley, PA, USA Deflectable tip 5–10-mm diameter scope Yes Extra long Storz, Tuttlingen, Germany 5-mm diameter with 30° lens Yes Eyemax Richard Wolf Medical Instruments
Corporation, Vernon Hills, IL, USA
5–10-mm diameter with 0–30° digital lens
Yes
Ideal Eyes HD Stryker, Kalamazoo, MI, USA 5-mm diameter articulating scope Yes
Instruments
Roticulator Covidien, Dublin, Ireland 5-mm diameter instruments Yes Prebent Various companies Basic curved instruments Yes Real Hand Novare, Cupertino, CA, USA 5-mm instruments No Autonomy laparo-angle Cambridge Endo, Framingham, MA, USA 5-mm articulating instruments Yes
Devices are presented in alphabetical order.
Transumbilical LESS in urology
sion29 and homemade access devices.30 Radical
nephrec-tomy has also seen broad use in several series.14,24,26,28–31A
common practice for right-sided nephrectomy has been the addition of a small 2–3-mm port to aid with liver retraction. This gives the surgeon a technical advantage while not sac-rificing the cosmetic benefit of LESS. A more recent series has shown that non-ischemic partial nephrectomy is safe and
feasible with LESS.32Table 2 details LESS kidney surgery
for malignancy.
The full cosmetic benefit of transumbilical LESS can be realized with reconstructive renal procedures. Unlike with many oncological indications, these do not require extension
of the original incision for specimen extraction. Desaiet al.
reported the first pyeloplasty using the R-Port with an addi-tional 2-mm port for a grasper and to aid with intracorporeal
suturing.33 A similar technique was described for simple
nephrectomy in a patient with a poorly functioning left kidney. The same group later published results with single-session bilateral pyeloplasty in two patients, as well as an
ileal ureter and a ureteroneocystostomy with a psoas hitch.34
This shows the evolution of transumbilical LESS techniques to more complex procedures. When compared with conven-tional laparoscopic pyeloplasty, transumbilical LESS pyelo-plasty has been found to have similar immediate outcomes, including length of hospital stay, morphine equivalents, and
minor and major complications.15 Surprisingly, they also
found that median operative times and median estimated blood loss were lower in patients undergoing LESS. This might represent increased attending involvement with LESS inherent at teaching institutions with new techniques.
The transplantation arena has been fertile ground for LESS application and investigation. Transumbilical LESS donor nephrectomy provides the patient cosmetic benefit and potentially faster recovery time with decreased periop-erative pain compared with conventional laparoscopic and open donor nephrectomy. The first experience with LESS donor nephrectomy used the R-Port, as well as a 2-mm port
without an incision to aid in retraction.35A comparison with
conventional laparoscopy has shown that there is an associ-ated quicker convalescence with LESS patients, including days on oral pain medication, days off work and days to
100% recovery.36
Other miscellaneous renal procedures have been com-pleted successfully with transumbilical LESS. These include simple nephrectomy for benign indications and cyst decor-tication. See Table 3 for experience with these procedures, as well as the reconstructive and donor nephrectomy experience.
Adrenal
A rare application of transumbilical LESS has been for adrenalectomy, perhaps because retraction is so crucial to expose the gland. Several series have been published to
date,26,30including the largest that includes a matched case–
control study comparing conventional laparoscopic with
transumbilical LESS adrenalectomy.17 Nine LESS
proce-dures were compared with 17 conventional laparoscopic adrenalectomies matched to age, sex, surgical indications and tumor size. The indications for the LESS procedures
were benign adenoma (n=3), Cushing’s Syndrome (n=1)
and pheochromocytoma (n=5). Tumor size differed
signifi-cantly between groups, with an average size of 2.8 cm (1–5.4 cm) in the LESS cohort compared with 4.3 cm (2.5– 6.0 cm) in the CL group. However, the techniques were similar in terms of conversion rate, operative time, estimated blood loss, complications and hospital stay. The LESS group did have a shorter duration of patient controlled anesthesia
(0.9 days vs1.9 days). Table 4 summarizes the current
lit-erature in regard to transumbilical LESS adrenalectomy.
Ureter
One of the theoretical advantages of the umbilicus as a portal-of-entry is the ability to operate in all quadrants. As the ureter encompasses such a long path, ureteral pathology presents a potential opportunity to capitalize on the versa-tility of umbilical LESS. The variety of ureteral procedures spans oncology, reconstructive and stone diseases. Table 5 describes current literature for LESS ureteral surgeries across this spectrum.
The series of ureterolithotomy described by Leeet al.is the
largest report.42Here, 30 transumbilical LESS
ureterolitho-tomies were carried out successfully with no conversions to conventional laparoscopy. A homemade device was used for access using a 2–3-cm umbilical incision. Patient satisfaction was analyzed and the authors found that 28 out of 30 patients (93.3%) were satisfied with their postoperative outcomes.
Bladder
Current LESS experience with bladder procedures includes those listed in Table 6. Procedures accomplished to date through a LESS approach include radical and partial cystec-tomy, augmentation enterocystoplasty, sacral colpopexy and vesicovaginal fistula repair. Of note, a comparative study
carried out by Whiteet al.looking at sacral colpopexy found
similar efficacy and improved cosmesis for transumbilical
LESS versus laparoscopic and robotic techniques.18There
were no conversions and no immediate complications. The patients showed prolapse reduction at 6 months follow up, and were overall satisfied with the outcomes. The authors state that they are exploring this technique robotically to overcome the learning curve associated with the procedure.
Prostate
With tremendous experience in minimally invasive (laparo-scopic and robotic) prostatectomy, it is not surprising that
JE HUMPHREY AND D CANES
Table 2 Current experience with oncological renal procedures using transumbilical LESS
Author, year
Procedure (n) Access
device
MOT (min) EBL (mL) LOS (days) Complications (n) Conversion
to open/lap
Comments
Goel,
200823
Renal cryoxablation (2) Uni-X 1.5 Flexible,
5 mm, 0°
Flexible grasper, 10 mm flexible ultrasound probe,
None 0 Also performed 4 via
retroperitoneal
Partial nephrectomy (5) R-Port 2.5–4 Rigid, 5 mm,
30°
Straight, plus curved and articulating
3 (3–22) 1 patient with:
pseudoaneurysm,
All right-sided partial nephrectomies
Desai,
200926
Radical nephrectomy (3) nephroureterectomy (2), partial nephrectomy (6)
R-Port Not reported Rigid, 5 mm,
30° or injury, urinary tract infection, urine leak
1 conventional lap
Also performed 33 transvesical procedures through
Kaouk,
200927
Partial nephrectomy (4) Uni-X 1.8 Flexible,
5 mm, 0°
Bent and articulating No 160 420
(50–1200)
3.2 Parenchymal
bleeding ( convert to lap
1 Also performed 1
retroperitoneal and 2 robotic
White,
200924
Cryoablation (8), partial nephrectomy (15), radical nephrectomy (6), nephroureterectomy (7)
Variable, not reported
Not reported Not reported Straight and
articulating
No Varies with
procedure
Varies with procedure
Varies with procedure
Blood transfusion (7), deep vein thrombosis (1),
angio-Describe pure LESS as well as transition to robotic-assisted LESS
Rais-Bahrami,
200929
Radical nephrectomy (2) Staggered
ports in umbilical incision
Not reported Flexible,
5 mm, 0°
-3 (2–4) Delayed hemorrhage
requiring angio-embolization
0 Also performed 4
LESS donor nephrectomies through pfannenstiel incision
Partial nephrectomy (3)
-149.67
Radical nephrectomy (10) Triport 3.95 (3–6) Rigid, 5 mm,
30°
202 (50–900) Not
reported
Intraoperative bleed requiring blood transfusion
0 Suggest present
instruments would aid technique
Raman,
200914
Radical nephrectomy (6) Single
incision with
122 (90–210) 20 (10–600) 2.04
(1.25–3.08)
None 0 Compared to 22
conventional laparoscopic cases, LESS had lower mean
EBL (20vs100)
Stein,
201028
All robotic: pyeloplasty (2), radical nephrectomy (1), partial nephrectomy (1)
GelPort 2.5–5 12 mm
robotic scope, 30° and 0°
Standard robotic instruments
No Varies with
procedure
Varies with procedure
1–2 Blood transfusion (1) 0 Larger incision for
GelPort used for extraction of partial nephrectomy (2), robotic-LESS: partial nephrectomy (11), nephroureterectomy (3), radical nephrectomy (1)
Home-made
No Varies with
procedure
Varies with procedure
Varies with procedure
Bowel injury (2), diaphragm injury (1), transfusion (1) for various urological procedures
0° and rigid, 5 mm, 45°
Straight conventional instruments
No 177.4 148.1 2.57 Urine leak (1) 1 (converted
Table 3 Non-oncological renal transumbilical LESS experience
Author, year Procedure (n) Access
device
Postoperative incision (cm)
Scope Instruments used Additional ports MOT (min) EBL (mL) LOS (days) Complications
(n) ileal ureter (1), uretero-neocystostomy with psoas hitch (1)
R-Port 1.5–3 Not reported Straight and bent Yes (2-mm port) 277
(180–360) 68.75 (50–100)
2 (1–3) None 0 Placed Jackson-Pratt
drains via umbilical incision
Tracy,
200915
Pyeloplasty (14) Single
incision with 3 adjacent trocars
2.5 Rigid, 5 mm, 45° Straight and
articulating
Yes (3-mm and 5-mm port)
202 (178–240)
35 (25–50) 77 (50–149) Hematuria (2),
urine leak (2), acute clot obstruction (1)
0 All outcome measures
were similar to 28 conventional laparoscopic pyeloplasties
Rais-Bahrami,
200929
Pyeloplasty (2) Staggered
ports in umbilical incision
Not reported Flexible, 5 mm,
0°
Straight and flexible
No -203
(199–207)
-100 -2 None 0 Also performed 4 LESS
donor nephrectomies via pfannenstiel incision
Desai,
200926
Pyeloplasty (17) R-Port Not reported Rigid, 5 mm, 30°
or Flexible, 5 mm, 0°
Straight, bent, and articulating
Yes (5-mm port required in 2 cases)
236 (12–360) 79 (10–150) 2 (2–3) None 1
conventional lap
All patients symptom free
White,
200924
Pyeloplasty (8) Variable, not
reported directly
Not reported Not reported Straight and
articulating
No Varies with
procedure
Varies with procedure
Varies with procedure
Hernia (1) None Part of larger series
examining first 100 cases at single center
Stein,
201028
All robotic: pyeloplasty (2)
GelPort 2.5–5 12 mm robotic
scope, 30° and 0°
Standard robotic instruments
No Varies with
procedure
Varies with procedure
1–2 None 0 Robotic-assisted LESS
with GelPort affords greater spacing of ports
R-Port 4–5 Rigid, 5 mm, 30° Straight, plus
curved and articulating selectively
Yes (2-mm port) 198
(180–300)
50 (50–200) 3 None 0 Use of 2 mm port helps
improve triangulation without actual incision
Canes,
201036
Left donor nephrectomy (17)
R-Port 2–2.5 extended
to 4.1 cm (median)
Rigid, 5 mm, 30° Straight, curved,
and articulating
108 (50–200) 3 (1–6) Allograft
thrombosis in 1 patient
1 to conventional laparoscopy
Prolonged warm ischemia time when compared with
5.23 (4–7) Not reported Straight and bent Yes (3- or 5-mm
in 11 cases for retraction)
176.9 (90–240)
158.18 (50–300)
3 (2–5) None 0 Comment that
xiphoid-to-umbilicus
length>16 cm
increases difficulty
R-Port Not reported Rigid, 5 mm, 30°
or Flexible,
104 (50–200) 2.9 (1–6) Corneal abrasion
(1), dyskinesia from antiemetics (1), graft loss due to intravascular clotting (1)
None Median warm ischemia
White,
Not reported Not reported Straight and
articulating
No 218 116 3.4 None 2 to conventional
lap with 3 adjacent trocars
3 None 0 Note that single-use
access devices are expensive and may limit maneuverability
Other renal procedures Rane,
200939
Simple nephrectomy (3)
Triport Not reported Rigid, 5 mm, 30° Straight and
articulating
No 95 (45–150) 66.6
(50–100)
2.33 (2–3) Port-site
bruising, transient postoperative pyrexia
0 Also performed 2 cases
with port in mid-clavicular line
R-Port Not reported Rigid, 5 mm, 30°
or Flexible, 5 mm, 0°
Straight, bent, and articulating
Yes (2-mm port required in 5 cases)
None 0 All simple
nephrectomies morcellated and extracted; cyst with unobstructed drainage -Kidney cyst
excision (1)
-60 -<50
Not reported Not reported Straight and
articulating
No -156 -121 2.3 None 0 Part of larger series
examining first 100 cases at single center -Cyst with 3 adjacent trocars
2.5 Rigid, 5 mm, 45° Straight and
articulating
Yes (3-mm subxyphoid trocar for right nephrectomy)
122 (90–210) 20 (10–600) 2.04 (1.25–3.08) None 0 Compared to 22
conventional laparoscopic cases, LESS had lower mean
EBL (20vs100)
R-Port 2 Flexible, 5 mm,
0°
Straight, flexible, and bent
Yes (2-mm grasper in one case, 3-mm incision for 5 mm grasper in one case)
151 (45–290) 51 (20–100) 2.36 (1–4) Port-site
bruising, transient postoperative pyrexia
0 Compared to
traditional laparoscopy, cosmetic advantage, but no other significant differences
2–3 Flexible, 5 mm,
0° or rigid, 10 mm, 0°
Straight and flexible
No 151 (85–230) 108 (0–500) 3.1 (2–6) Mild fever (1),
mild ileus (2)
0 Demonstrates ability to
use home-made device for access
Rigid, 5–10 mm, 30°; 12 mm
No Varies with
procedure
Varies with procedure
Varies with procedure
Bowel injury (1) during robotic LESS simple nephrectomy
0 Demonstrates
versatility of home-made device for various urological
30° and flexible, 5 mm, 0°
Straight and flexible
Yes (3-mm port for liver retraction in 1 patient)
125 (96–165) 112 (50–250) 3.5 (2–7) Lymphatic
leakage (1)
0 No recurrence of
chyluria with average of 8.3 months follow up
Table 4 Adrenal procedures using transumbilical LESS
Author, year Procedure (n) Access device Postoperative
incision (cm)
Scope Instruments used Additional ports MOT (min) EBL (mL) LOS (days) Complications (n) Conversion
to open/lap
Comments
Jeong, 200917 Adrenalectomy
(9)
Home-made device
2 Flexible, 5 mm,
0°
Straight and articulating
No 169.2 (89–289) 177.8 (50–400) 3.2 (2–4) Serosal tear (1) 0 Matched to
conventional laparoscopy with comparable results
Desai, 200926 Adrenalectomy
(1)
R-Port Not reported Rigid, 5 mm, 30°
or Flexible, 5 mm, 0°
Straight, bent, and articulating
Yes (2-mm port) 150 350 3 Bleeding with
right renal vein injury, subsequent renal vein thrombus (1)
1 to conventional laparoscopy
Only case was converted due to right renal vein injury
Jeon, 201030 Adrenalectomy
(2)
Home-made device
Not reported Rigid, 5–10 mm,
30°; 12 mm robotic scope
Straight, articulating, and flexible
N0 260 125 3 None 0 Demonstrates
versatility of home-made device for various urological procedures
Table 5 Ureteral procedures using transumbilical LESS (excluding nephroureterectomy)
Author, Year Procedure (n) Access device Postoperative
incision (cm)
Scope Instruments used Additional ports MOT (min) EBL (mL) LOS (days) Complications (n) Conversion
to open/lap
Comments
Desai, 200933 Ileal ureter (1),
uretero-neocystostomy with psoas hitch (1)
R-Port 1.5–3 Not reported Straight and bent Yes (2-mm port
for grasper, no true incision)
277 (180–360) 68.75 (50–100) 2 (1–3) None 0 Placed
Jackson-Pratt drains via umbilical incision
Desai, 200926 -Ureteral
reimplant (2)
R-Port Not reported Rigid, 5 mm, 30°
or Flexible, 5 mm, 0°
Straight, bent, and articulating
Yes (2-mm port) -175 (140–210) -175 (100–250) -4 Anastomotic leak
(1)
0 Part of larger
series examining first 100 cases at single center
-Ileal ureter (3) -330 (300–360) -170 (90–250) -2
White, 200924 Ureteral
reimplant (1)
Not reported Not reported Not reported Straight and
articulating
No 180 100 3 None 0 MAG3 normal
Jeon, 201030 -Ureterectomy (1) Home-made
device
Not reported Rigid, 5–10 mm,
30°; 12 mm robotic scope
Straight, articulating, and flexible
No -80 -150 -3 None 0 Ureterectomy
for duplication, ectopic ureter -Ureterolithotomy
(1)
-2 -310 -210 -6
Lee, 201142 Ureterolithotomy
(30)
Home-made device
2–3 Rigid, 10 mm, 0° Straight, flexible,
and articulating Yes
(transcutaneous port for one patient, size not reported)
110.43 61.17 3.40 Fever (2), mild
ileus (1)
1 Useful if
ureteroscopy or shockwave lithotripsy not available
JE
HUMPHREY
AND
D
CANES
424
©
2012
The
Japanese
Urolo
gical
Table 6 Bladder Procedures using transumbilical LESS
Author, year Procedure (n) Access device Postoperative
incision (cm)
Scope Instruments used Additional ports MOT (min) EBL (mL) LOS (days) Complications (n) Conversion
to open/lap
Comments
Noguera, 200943 Augmentation
enterocystoplasty (1)
Quadport 5 Flexible, 5 mm,
0°
Straight and flexible
No 300 <100 6 None 0 Bowel resection
and anastomosis performed extracorporeally
White, 200918 Sacral colpopexy
(10)
Uni-X 1.8 Flexible, 5 mm,
0°
Straight and articulating
No 162 47.5 1.5 Cystocele (1),
stress incontinence (2)
0 Single-port
comparable in series to matched laparoscopic and robotic cases
White, 200924 Radical
cystectomy (3)
Variable, not reported directly
Not reported Not reported Straight and
articulating
No -315 -216 -6.6 None 0 Cystectomy
lymph node
yield=16
Sacral colpopexy (13)
-182 -46.9 -1.6
Kaouk, 201044 Radical
cystectomy (3)
Uni-X 4.5–5 (1.8 cm
before extraction)
Flexible, 5 mm, 0°
Straight and flexible
No 315 (285–360) 217 (200–250) 6 (5–7) None 0 Operative time
decreased from first to third patient
Jeon, 201030 Partial
cystectomy (1)
Home-made device
Variable with procedure
Rigid, 5–10 mm, 30°; 12 mm robotic scope
Straight, articulating, and flexible
No 175 50 4 None 0 Demonstrates
versatility of home-made device for various urological procedures
Abdel-Karim,
201145
Vesicovaginal fistula repair (5)
Triport 2 Flexible, 5 mm,
0°
Bent Yes (in all cases,
5-mm port added for suturing and triangulation)
198 (170–240) 90 (70–120) 2 None 0 Less pain and
shorter hospital stay than same group’s conventional laparoscopic cases
T
ransumbilical
LESS
in
urolo
gy
©
2012
The
Japanese
Urolo
gical
Association
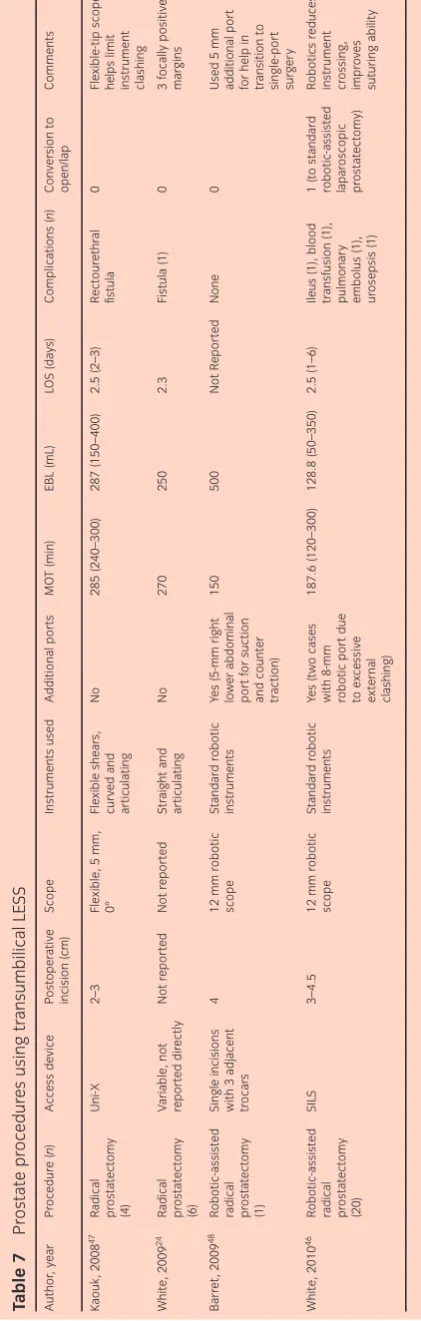
LESS prostatectomy would ultimately be cautiously explored. This has been described both laparoscopically and with robotic LESS. Robotic instruments with articulating tips provide the surgeon with better dexterity when operat-ing through the LESS avenue. The largest series described 20 patients undergoing robotic LESS prostatectomy with reasonable mean operative time (187.6 min), estimated blood loss (128.8 mL) and average length of stay
(2.5 days).46 They concluded that robotic assistance
“reduces or eliminates instrument crossing, has superior ergonomics, and instrument tip articulation significantly facilitates suturing.” Their series is compared with other LESS prostate series in Table 7.
Robotic LESS
Use of robotics for assistance with LESS procedures was intended to bring increased dexterity to offset some of the frustrations with standard laparoscopic LESS surgery. The da Vinci robotic system (Intuitive Surgical, Sunnyvale, CA, USA) has been used successfully through a single
transum-bilical port in a variety of procedures. In 2009, Raneet al.
discussed the use of robotics with LESS and its implications
for future directions.49They described how robotics can aid
LESS with superior visualization of the operative field , enhanced surgical dexterity and excellent ergonomics.
However, the original da Vinci robotic system was not designed specifically for single-site surgery, and therefore has its own limitations. First, the external size and straight shape of the robotic arms lead to external clashing over a single port. Second , the original robotic instrument shafts themselves do not articulate, and therefore intracorporeal clashing can occur as well.
To this end , the newer da Vinci Si surgical system has been modified to be more amenable to single-site surgery. There has been development of VeSPA surgical instruments (Intuitive Surgical) to overcome the aforementioned limita-tions. These instruments are inserted through curved cannu-lae and allow multiple ports through one incision while still allowing intra-abdominal triangulation. The feasibility of this technique was shown in a porcine model in 2010, in which the authors completed various kidney procedures (pyeloplasty, partial nephrectomy, nephrectomy) showing
improved ergonomics and minimal instrument clashing.50
Disadvantages
Transumbilical LESS does have difficulties associated with it that the surgeon must weigh with the cosmetic benefit. As aforementioned , in general utilizing a LESS technique will lead to either no true triangulation or a reliance on curved or bent instruments in order to create triangulation. Thus, there is a learning curve to LESS that might dissuade community
urologists from accepting LESS into their practice. Another Table
7
Radical prostatectomy (4)
Uni-X
Radical prostatectomy (6)
V
Robotic-assisted radical prostatectomy (1)
Single
Robotic-assisted radical prostatectomy (20)
SIL
instrument crossing, impr
o
ves
suturing
ability
JE HUMPHREY AND D CANES
important aspect of incorporating transumbilical LESS is the potential cost of newer instruments and access devices. It might not be worth both the training and cost associated with LESS for the urologist who only has a limited use for LESS. However, there has been no dedicated analysis of cost associated with LESS to this date.
Conclusion
The progression of minimally invasive surgery has led urologists to explore LESS. Born out of a desire for improved cosmesis, and the potential for reduced operative trauma, decreased postoperative pain and complications, transumbilical LESS has successfully been implemented into the urologist’s armamentarium. However, the future role of LESS is still uncertain. Although large specialty centers have described LESS for virtually all urological laparoscopic procedures, it is unclear whether LESS will diffuse beyond select centers. The majority of data available are based on non-randomized series, whereby selection bias might play a significant role. However, a randomized pro-spective trial would be very difficult to complete comparing LESS to conventional laparoscopy. It does seem evident that the cosmetic benefit from LESS is real and reproducible, but any incremental benefit apart from cosmesis seems unlikely to match the leap previously witnessed from open surgery to laparoscopy.
Surgical device companies have responded by developing access devices, scopes and instruments more specifically aimed towards LESS. As technology improves, this will no doubt continue to make the transition to LESS easier for more surgeons. Currently-available LESS training courses should be considered for surgeons interested in LESS techniques to benefit from the collective experience of early adopters.
The urological transumbilical LESS experience is rapidly growing, but many questions remain. Whether the benefits of LESS truly outweigh its technical challenges is currently un-known. We also cannot predict whether LESS in some form will become a permanent fixture in our arsenal, or a historical footnote. For now, LESS surgery remains the subject of intense scrutiny, and is a laudable example of surgical cre-ativity aimed at minimizing surgical trauma for our patients.
Conflict of interest
None declared.
References
1 Box G, Averch T, Cadeddu Jet al. Nomenclature of Natural Orifice Transluminal Endoscopic Surgery (NOTES™) and Laparoendoscopic Single-Site Surgery (LESS) procedures in urology.J. Endourol.2008;22: 2575–81.
2 Raman JD, Bensalah K, Bagrodia A, Stern JM, Cadeddu JA. Laboratory and clinical development of single keyhole umbilical nephrectomy.Urology2007;70: 1039–42. 3 Wheeless CR. Outpatient laparoscope sterilization under
local anesthesia.Obstet. Gynecol.1972;39: 767–70. 4 Pelosi MA, Pelosi MA III. Laparoscopic hysterectomy with
bilateral salpingo-oophorectomy using a single umbilical puncture.N. J. Med.1991;8: 721–6.
5 Pelosi MA, Pelosi MA III. Laparoscopic appendectomy using a single umbilical puncture (minilaparoscopy).J. Reprod. Med.1992;37: 588–94.
6 D’Alessio A, Piro E, Tadini B, Beretta F. One-trocar transumbilical laparoscopic-assisted appendectomy in children: our experience.Eur. J. Pediatr. Surg.2002;12: 24–7.
7 Navarra G, Pozza E, Occhionorelli S, Carcoforo P, Donini I. One-wound laparoscopic cholecystectomy.Br. J. Surg. 1997;84: 695.
8 Piskun G, Rajpal S. Transumbilical laparoscopic
cholecystectomy utilizes no incisions outside the umbilicus. J. Laparoendosc. Adv. Surg. Tech. A1999;9: 361–4. 9 Kercher KW, Heniford BT, Matthews BDet al.
Laparoscopic vs open nephrectomy in 210 consecutive patients.Surg. Endosc.2003;17: 1889–95.
10 Rane A, Kommu S, Eddy B, Bonadio F, Rao P, Rao P. Clinical evaluation of a novel laparoscopic port (R-port) and evolution of the single laparoscopic port procedure (SLiPP).J. Endourol.2007;21(Suppl 1): A22–23. 11 Ponsky LE, Cherullo EE, Sawyer M, Hartke D. Single
access site laparoscopic radical nephrectomy: initial clinical experience.J. Endourol.2008;22: 663–5.
12 Nomura T, Sato F, Takahashi M, Sumino Y, Mimata H. Laparoendoscopic single-site (LESS) retroperitoneal radical nephrectomy in a patient with renal cell carcinoma receiving hemodialysis.Case Report Med2011; doi:10.1155/2011/506032.
13 Ponsky LE, Steinway ML, Lengu IJ, Hartke DM, Vourganti S, Cherullo EE. A pfannenstiel single-site nephrectomy and nephroureterectomy: a practical application of laparoendoscopic single-site surgery.Urology2009;74: 482–5.
14 Raman JD, Bagrodia A, Cadeddu JA. Single-incision, umbilical laparoscopic versus conventional laparoscopic nephrectomy: a comparison of perioperative outcomes and short-term measures of convalescence.Eur. Urol.2009;55: 1198–206.
15 Tracy CR, Raman JD, Bagrodia A, Cadeddu JA.
Perioperative outcomes in patients undergoing conventional laparoscopic versus laparoendoscopic single-site
pyeloplasty.Urology2009;74: 1029–35.
16 Raybourn JH III, Rane A, Sundaram CP. Laparoendoscopic single-site surgery for nephrectomy as a feasible alternative to traditional laparoscopy.Urology2010;75: 100–3. 17 Jeong BC, Park YH, Han DH, Kim HH. Laparoendoscopic
single-site and conventional laparoscopic adrenalectomy.J. Endourol.2009;23: 1957–60.
18 White WM, Goel RK, Swartz MA, Moore C, Rackley RR, Kaouk JH. Single-port laparoscopic abdominal sacral
Transumbilical LESS in urology
colpopexy: initial experience and comparative outcomes. Urology2009;74: 1008–12.
19 Park SK, Olweny EO, Best SL, Tracy CR, Mir SA, Cadeddu JA. Patient-reported body image and cosmesis outcomes following kidney surgery: comparison of laparoendoscopic single-site, laparoscopic, and open surgery.Eur. Urol.2011;60: 1097–104;
doi:10.1016/j.eururo.2011.08.007.
20 Sawyer MD, Ponsky LE. Technical and equipment challenges for laparoendoscopic single-site surgery and natural orifice transluminal endoscopic surgery.BJU Int. 2010;106: 892–6.
21 Castellucci SA, Curcillo PG, Ginsberg PCet al. Single port access adrenalectomy.J. Endourol.2008;22: 1573–6. 22 Gill IS, Advincula AP, Aron Met al. Consensus statement
of the consortium for laparoendoscopic single-site surgery. Surg. Endosc.2010;24: 762–8.
23 Goel RK, Kaouk JH. Single port access renal cryoablation (SPARC): a new approach.Eur. Urol.2008;53: 1204–9. 24 White WM, Haber GP, Goel RK, Crouzet S, Stein RJ,
Kaouk JH. Single-port urological surgery: single-center experience with the first 100 cases.Urology2009;74: 801–4.
25 Aron M, Canes D, Desai MMet al. Transumbilical single-port laparoscopic partial nephrectomy.BJU Int. 2008;103: 516–21.
26 Desai MM, Berger AK, Brandina Ret al. Laparoendoscopic single-site surgery: initial hundred patients.Urology2009;
74: 805–13.
27 Kaouk JH, Goel RK. Single-port laparoscopic and robotic partial nephrectomy.Eur. Urol.2009;55: 1163–70. 28 Stein RJ, White WM, Goel RK, Irwin BH, Haber GP,
Kaouk JH. Robotic laparoendoscopic single-site surgery using GelPort as the access platform.Eur. Urol.2010;57: 132–7.
29 Rais-Bahrami S, Montag S, Atalla MA, Andonian S, Kavoussi LR, Richstone L. Laparoendoscopic single-site surgery of the kidney with no accessory trocars: an initial experience.J. Endourol.2009;23: 1319–24.
30 Jeon HG, Jeong W, Oh CKet al. Initial experience with 50 laparoendoscopic single site surgeries using a homemade, single port device at a single center.J. Endourol.2010;
183: 1866–72.
31 Stolzenburg JU, Kallidonis P, Hellawell Get al. Technique of laparoscopic-endoscopic single-site surgery radical nephrectomy.Eur. Urol.2009;56: 644–50.
32 Bazzi WM, Allaf ME, Berkowitz J, Atalah HN, Parekattil S, Derweesh IH. Multicenter experience with nonischemic multiport laparoscopic and laparoendoscopic single-site partial nephrectomy utilizing bipolar radiofrequency ablation coagulator.Diagn Ther Endosc2011; DOI: 10.1155/2011/636537.
33 Desai MM, Rao PP, Aron Met al. Scarless single port transumbilical nephrectomy and pyeloplasty: first clinical report.BJU Int.2008;101: 83–8.
34 Desai MM, Stein R, Rao Pet al. Embryonic Natural Orifice Transumbilical Endoscopic Surgery (E-NOTES) for
advanced reconstruction: initial experience.Urology2009;
73: 182–7.
35 Gill IS, Canes D, Aron Met al. Single port transumbilical (E-NOTES) donor nephrectomy.J. Urol.2008;180: 637–41.
36 Canes D, Berger A, Aron Met al. Laparo-Endoscopic Single Site (LESS) versus standard laparoscopic left donor nephrectomy: matched-pair comparison.Eur. Urol.2010;
57: 95–101.
37 Ganpule AP, Dhawan DR, Kurien Aet al.
Laparoendoscopic single-site donor nephrectomy: a single-center experience.Urology2009;74: 1238–40. 38 Dubey D, Shrinivas RP, Srikanth G. Transumbilical
laparoendoscopic single-site donor nephrectomy: Without the use of a single port access device.Indian J. Urol.2011;
27: 180–4.
39 Rane A, Ahmed S, Kommu SS, Anderson CJ, Rimington PD. Single-port “scarless” laparoscopic nephrectomies: the United Kingdom experience.BJU Int.2009;104: 230–3. 40 Han WK, Park YH, Jeon HGet al. The feasibility of
laparoendoscopic single-site nephrectomy: initial experience using home-made single-port device.Urology 2010;76: 862–5.
41 Zhang Y, Ye J, Wu Get al. Transumbilical laparoendoscopic single-site renal pedicle lymphatic disconnection for refractory chyluria.J. Endourol.2011;
25: 1337–41.
42 Lee JY, Han JH, Kim TH, Yoo TK, Park SY, Lee SW. Laparoendoscopic single-site ureterolithotomy for upper ureteral stone disease: the first 30 cases in a multicenter study.J. Endourol.2011;25: 1293–8.
43 Noguera RJS, Astigueta JC, Carmona Oet al. Laparoscopic augmentation enterocystoplasty through a single trocar. Urology2009;73: 1371–4.
44 Kaouk JH, Goel RK, White MAet al. Laparoendoscopic Single-site Radical Cystectomy and Pelvic Lymph Node Dissection: Initial Experience and 2-Year Follow-up. Urology2010;76: 857–61.
45 Abdel-Karim AM, Moussa A, Elsalmy S. Laparoendoscopic single-site surgery extravesical repair of vesicovaginal fistula: early experience.Urology2011;78: 567–71. 46 White MA, Haber GP, Autorino Ret al. Robotic
laparoendoscopic single-site radical prostatectomy: technique and early outcomes.Eur. Urol.2010;58: 544–50. 47 Kaouk JH, Goel RK, Haber GP, Crouzet S, Desai MM,
Gill IS. Single-port laparoscopic radical prostatectomy. Urology2008;72: 1190–3.
48 Barret E, Sanchez-Salas R, Kasraeian Aet al. A transition to laparoendoscopic single-site surgery (LESS) radical prostatectomy: human cadaver experimental and initial clinical experience.J. Endourol.2009;23: 135–40. 49 Rane A, Tan GY, Tewari AK. Laparo-endoscopic
single-site surgery in urology: is robotics the missing link? BJU Int.2009;104: 1041–3.
50 Haber GP, White MA, Autorino Ret al. Novel Robotic da Vinci instruments for laparoendoscopic single-site surgery. Urology2010;76: 1279–82.
JE HUMPHREY AND D CANES