The Prognostic Value of Nailfold Capillary
Changes for the Development of Connective
Tissue Disease in Children and Adolescents with
Primary Raynaud Phenomenon: A Follow-up
Study of 250 Patients
Slavica Pavlov-Dolijanovic´, M.D., M.Sc.,* Nemanja Damjanov, M.D., Ph.D.,* Predrag Ostojic´,
M.D., M.Sc.,* Gordana Susˇic´, M.D., M.Sc.,* Roksanda Stojanovic´, M.D., Ph.D.,* Dragica
Gacic´, M.D.,* and Aleksandra Grdinic´, M.D., M.Sc.
*Institute of Rheumatology-Belgrade, KBC ‘‘Dragisˇa Misˇovic´-Dedinje’’, Belgrade, Serbia and Montenegro
Abstract:
To assess the prognostic value of capillaroscopy findings for the development of connective tissue disease in children and adolescents with Raynaud phenomenon, we followed up a group of 250 (mean age 15 years) for 1 to 6 years after the first capillaroscopy was performed. Every 6 months they were screened for signs and symptoms of connective tissue disease. Analysis was performed on capillary changes registered 6 months before the development of connective tissue disease. Capillary changes were classified into three types: normal, nonspecific, and sclerodermatous. At the end of the follow-up period, 191 (76%) subjects had primary Raynaud phenomenon, 27 (10.8%) were diagnosed as having undifferentiated con-nective tissue disease, and 32 (12.8%) fulfilled the criteria for a diagnosis of a specific connective tissue disease. Systemic lupus erythematosus was found in nine (3.6%) patients, rheumatoid arthritis in 10 (4%) patients (six of them with juvenile onset rheumatoid arthritis), and scleroderma spectrum disorders in 13 (5.2%). The mean time for the evolution of Raynaud phe-nomenon into undifferentiated connective tissue disease or a form of the disease was 2 years. Most of the subjects with primary Raynaud phenom-enon (173/191, 91%), undifferentiated connective tissue disease (22/27, 81%), juvenile onset rheumatoid arthritis/rheumatoid arthritis (7/10, 70%), and systemic lupus erythematosus (6/9, 67%) had normal capillary findings. Nonspecific capillary changes occurred in 3 of 10 (30%) patients with rheu-matoid arthritis, 2 of 9 (22%) with systemic lupus erythematosus, 4 of 27 (15%) with undifferentiated connective tissue disease, and 18 of 191 (9%) with primary Raynaud phenomenon. Of all the subjects, only 10 (4%) showed sclerodermatous disease type capillary changes 6 months before theAddress Correspondence to Slavica Pavlov-Dolijanovic´, M.D., M.Sc., Institute of Rheumatology-Belgrade, Institute of Rheuma-tology-Belgrade, Resavska 69, 11 000 Belgrade, Serbia and Montenegro, or e-mail: [email protected] or [email protected]
expression of a particular disease: eight (62%) of these developed sclero-derma spectrum disorders, one expressed systemic lupus erythematosus, and one had undifferentiated connective tissue disease. We concluded that there were no specific capillary changes predictive for future development of systemic lupus erythematosus, juvenile onset rheumatoid arthritis/rheuma-toid arthritis, and undifferentiated connective tissue disease in children and adolescents with Raynaud phenomenon. Most of our study subjects with Raynaud phenomenon who developed these diseases had normal capillary findings or nonspecific changes. Children and adolescents who developed scleroderma spectrum disorders showed a sclerodermatous type of capillary changes 6 months before the expression of the disease, indicating that this type of capillary changes in children and adolescents with Raynaud phe-nomenon highly correlated with further development of scleroderma spec-trum disorders.
Raynaud phenomenon (RP) in adults, as well as in children, is a vasospastic disorder characterized by the episodic color changes of blanching, cyanosis, and hyperemia of the digits in response to cold (1). In adults RP can occur in response to emotional stress. However, no evidence of relationship between the occurrence of RP and emotional stress was found in children (2). It can be classified as a primary phenomenon of unknown cause, or secondary to a number of different diseases, such as connective tissue diseases (CTD) (3). Most of the follow-up studies of children with RP noted the development of associated CTD in 25% to 30% of those affected (4,5), but some investigators reported up to 52% transition to CTD and 15% transition to probable CTD (6). The mean time between the onset of RP and development of CTD in children was 2 to 6 years (4–6).
Early detection of CTD in subjects with RP is important, and sometimes crucial for better treatment results, and a better prognosis. Therefore, it is important to assess the prognostic significance of various diagnostic methods for early detection of CTD in subjects with RP. One of these methods is nailfold capillaroscopy. This simple, noninvasive, easy-to-perform method is very important as a screening tool for detecting the subjects with RP who are at high risk for the development of CTD as adults (7). However, long-term protocol studies deal-ing with nailfold capillaroscopy changes in large homogeneous groups of children and adolescents with long-standing primary and secondary RP have not been conducted.
Significant changes in capillary morphology are pre-sent in 80% of adult patients with scleroderma and related disorders (7,8). These are called scleroderma (SD) type capillary changes and include mainly a decrease in capillary density and widened, giant loops, often sur-rounded by avascular areas. The extent of microangi-opathy detected by nailfold capillaroscopy has been shown to correlate with disease severity and prognosis
(7,9). Furthermore, the presence of SD type capillary changes in adult patients with RP is thought to be indicative of the future development of CTD, even in the absence of other disease symptoms (10,11). Comparable quantitative capillaroscopic data for healthy children, as well as for pediatric rheumatology patients are limited (12–15). Nevertheless, nailfold capillaroscopy findings have been proposed as a potential marker for more persistent disease in children with juvenile dermatomy-ositis (12) or systemic sclerosis (16). Correlation between the degree of vaculopathy and the clinical course has also been documented (12,13,16).
The aim of this study was to assess the prognostic value of capillaroscopic findings for the development of CTD in children and adolescents with RP, to detect the spectrum of CTD associated with RP, and to evaluate differences in duration of RP before the development of a specific CTD in the same patient population.
PATIENTS AND METHODS
Patients
Two hundred fifty children and adolescents with RP (205 girls and 45 boys) aged 10 to 20 years (mean age 15 years) were prospectively followed up in a study approved by the Research Ethic Committee of the Institute of Rheumatology, Belgrade. The median duration of RP was 2 years, ranging from 1 month to 11 years.
Methods
Children and adolescents with RP were followed up for 1 to 6 years after the first capillaroscopy was done. Capillaroscopy and a clinical search for criteria of CTD were repeated every 6 months.
et al (17), which is similar to the technique described by Maricq (18). Briefly, an OPTON microscope with 16·
and 100·magnifications was used. Cold light was
pro-vided by a Schott Mainz KL 150 fiber optic light source (50/60Hz, 2000W, lampe 15V/150W, Germany). Each subject was seated indoors for a minimum of 15 to 20 minutes before the examination, at a room tempera-ture of 20 to 22C. The nailfolds of eight fingers (the
second, third, fourth, and fifth on both hands) were examined in each patient, after a drop of immersion oil was placed on the nailfold bed to improve resolution. Fingers affected by recent local trauma were not ana-lyzed. Capillary changes found 6 months before the cri-teria for a diagnosis of CTD were fulfilled were used for analysis. These were classified into three types (7,8): normal (typical hair pin structure), nonspecific capillary changes (meandering and crossed capillaries, focal dis-tribution of capillary hemorrhages, capillary thinning, and capillary spasm), and the sclerodermatous type mentioned above.
Clinical search comprised history taking, physical examination, laboratory testing [including serologic tests for antinuclear antibodies (ANA), rheumatoid factor, and antiphospholipid (APL) antibodies], and particular analyses (including radiographies and ultrasound). Ser-ology and specific analyses were ordered according to clinical impression. None of the patients used beta-blockers.
Statistical Analysis
Chi-squared test with Yate’s correction for continuity was used.Pvalues were calculated by two-sided Fisher’s exact test.
RESULTS
Among 250 subjects included in the study, there were 110 (44%) children between 10 and 16 years of age, and 140 (56%) adolescents aged 17 to 20 years. Characteristics of the study population are shown in Table 1. Eighty-two
percent of the subjects were female children, the fema-le:male ratio was 5:1.
Follow-up Data
At the end of the follow-up period, 191 (76%) patients with RP had no signs and symptoms of CTD, and they were considered to have primary RP. Fifty-nine patients (23.6%) developed CTD, and were considered to have secondary RP (Table 2).
Distribution of the Types of Capillary Changes
Two hundred eleven children and adolescents with RP (84.4%) were classified as having normal type, 29 (11.6%) patients were classified as having nonspecific capillary changes, and 10 (4%) patients had the SD type (Table 2). The frequency of normal capillary findings in the subjects with primary RP was significantly higher than that in the patients with secondary RP (p < 0.01). On the other hand, the SD type was noted only among the patients who had secondary RP. Nonspecific capil-lary changes had a similar distribution in both primary and secondary RP subgroups.
Distribution of Subjects Who Developed CTD
After 2 years of follow-up, 27 of 250 (10.8%) subjects had some signs and symptoms of CTD, but did not fulfill the criteria for CTD, and they were considered to have undifferentiated CTD (Table 3). Thirty-two (12.8%) of
TABLE 1.Characteristics of the Study Population
No. of subjects
TABLE 2.Distribution of the Types of Capillary Changes in Children and Adolescents with Primary and Secondary Raynaud Phenomenon (RP)
Diagnosis
Type of capillary changes (patient numbers)
Total Normal Nonspecific SD type
Primary RP 173 18 0 191
Secondary RP 38 11 10 59
Total 211 29 10 250
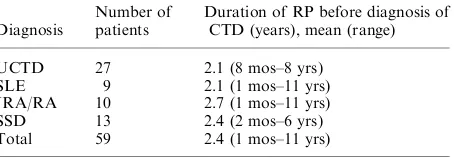
TABLE 3.Distribution of Patients who Developed Connective Tissue Diseases (CTD) during the 1- to 6-year Follow-up Period, and Duration of RP before Diagnosis of CTD
Diagnosis
Number of patients
Duration of RP before diagnosis of CTD (years), mean (range)
UCTD 27 2.1 (8 mos–8 yrs)
SLE 9 2.1 (1 mos–11 yrs)
JRA/RA 10 2.7 (1 mos–11 yrs)
SSD 13 2.4 (2 mos–6 yrs)
the 250 subjects fulfilled the criteria for the diagnosis of a particular CTD. The mean time between the beginning of RP until diagnosis of a particular CTD was 2.4 years. Among 32 patients with criteria sufficient for diagnosis of a particular CTD, nine (3.6%) patients had systemic lupus erythematosus (SLE), 10 (4%) patients had rheu-matoid arthritis (RA) [six of these were with juvenile onset RA (JRA)], and 13 (5.2%) subjects had sclero-derma spectrum disorders (five with sclero-dermatomyositis/ polymyositis, five with systemic sclerosis, and three with sclerodermatomyositis). The average duration of RP until diagnosis of CTD in patients who fulfilled the cri-teria for JRA/RA was not significantly longer than in those with other CTD (p¼0.8).
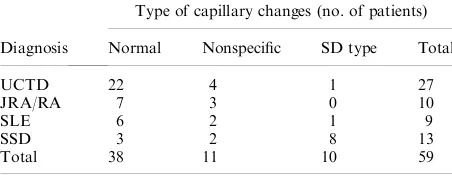
The distribution of different types of capillary changes in patients who developed CTD is shown in Table 4. Normal capillary findings were not significantly differ-ently distributed among the patients with undifferenti-ated connective tissue disease (UCTD), JRA/RA, and SLE. The frequency of normal capillary findings in the patients with UCTD was significantly higher than in those in the scleroderma spectrum disorders (SSD) sub-group (p¼0.0013). Nonspecific capillary changes were
distributed equally in the different subgroups of RP. SD-type capillary changes were present in 8 of 13 (61.5%) patients with SSD, in 1 of 9 (11.1%) patients with SLE, and 1 of 27 (3.7%) patients with UCTD. No JRA/RA patient showed any significant abnormality of capillary morphology. Sclerodermatous type capillary changes were significantly more frequent among the patients with SSD than among those with SLE and UCTD (p < 0.01).
Antiphospholipid antibodies were found in five chil-dren who had digital pits. Two of them were APL anti-body-positive, while others were negative.
DISCUSSION
The results of our study are comparable with those of other authors, indicating that RP in children and ado-lescents, as well as in adults principally affects females,
and in most cases, is not associated with the future development of CTD (5). In our study, for both primary and secondary RP, 82% of patients were female children. Approximately 76% of children and adolescents did not have any recognized underlying CTD (primary RP) and 24% of children and adolescents developed CTD (sec-ondary RP). The proportion of sec(sec-ondary RP in our study population was lower than that in other studies. Bethhencourt et al (19) found secondary RP in 10 of 32 (31.2%) children, Nigrovic et al found it in 19 of 52 (36.5%), and Duffy et al reported it in 14 of 27 (52%) children. One reason for these differences was probably the fact that we investigated children and adolescents together (up to 20 years of age), whereas the other authors included subjects only up to 18 years of age.
Our study confirms that, in most patients, RP is not associated with the future development of CTD, but in one of four children or adolescents it could be the first symptom of CTD, such as UCTD, SSD, JRA/RA, and SLE.
We found that the average RP duration before the development of CTD in children and adolescents was 2 years. The mean duration of RP till development of JRA/RA showed tendency to be longer than that for other CTD (p¼0.88). We were not able to see any
sig-nificant difference in RP duration before development of any CTD.
In our study, the greatest number of children and adolescents during the follow-up period developed UCTD (approximately 11%) or scleroderma spectrum disease (2% of patients had systemic sclerosis, 2% of patients had dermatomyositis/polymyositis, and 1.2% had sclerodermatomyositis), and a lesser number of patients developed JRA/RA (4%) or SLE (3.6%). Sim-ilar to our results, Nigrovic et al noted mixed CTD in 1.9% patients, scleroderma in 1.9% patients, and myo-sitis in 1.9% patients. These authors found arthritis in a large number of patients (28.8%). Rheumatoid arthritis is usually not reported as CTD underlying RP, i.e., sec-ondary RP. The data indicate that RP is not rare in adult patients with RA (20,21). Saraux et al (21) registered RP in 17.2% (54/332) RA adult patients. This group had a slightly higher prevalence of vasculitis than RA patients without RP. Among adults with RP, Grassi et al (22) found that 5% (38/781) of patients had RA. Cassidy reported 7% of RP adult patients had RA (23). However, JRA is thought to represent only 1% (23) or less than 1% (24) of the causes of RP. In our study, 6 of 250 (2.5%) children with RP developed JRA during 1 to 6 years of follow-up. Two of them were ANA positive (systemic onset JRA), and others were ANA negative (oligo- and polyarticular JRA). The later group is still being followed up as JRA could shift to other CTD (25,26).
TABLE 4.Distribution of Different Types of Capillary Changes in Patients with UCTD and a Articular CTD
Diagnosis
Type of capillary changes (no. of patients)
Normal Nonspecific SD type Total
UCTD 22 4 1 27
JRA/RA 7 3 0 10
SLE 6 2 1 9
SSD 3 2 8 13
An association of APL antibodies and RP is reported in adults (27) and children (5). The potential pathogenic mechanism for APL antibodies in RP is binding and activating endothelium (28). Endothelial damage and/or thrombosis in the digits might result. We investigated for APL antibodies in five children who had digital pits. The test was positive in two of them. All five patients finally developed SLE. In the study by Nigrovic et al (5), of children with secondary RP who were found to be APL antibody-positive (7/23; 30%), the majority (6/7) had SLE. They also reported a high prevalence of APL antibodies in children with primary RP (18/50; 36%).
In our study, subjects with primary RP and most of children and adolescents with RP who developed SLE, JRA/RA, and UCTD had normal capillary finding or nonspecific capillary changes. Only one subject who developed SLE (1/10, i.e., 11%) and one subject who developed UCTD (1/27, i.e., 3.7%) during the follow-up period had SD type capillary changes 6 months before the full expression of the disease. On the other hand, 8 of 13 (61%) children and adolescents who developed SSD (systemic sclerosis, dermatomyositis and sclerodermatomyositis) exhibited SD type capillary changes 6 months before the full expression of the disease.
In our 250 children and adolescents, we found that SD-type capillary changes significantly correlated with the future development of scleroderma spectrum dis-orders. This finding was similar to that reported by Duffy et al. Also, Dolezalova et al found a strong correlation between lower capillary density, enlarged dilated capillary loops, abnormal capillaries, avascular areas, and nailfold vascular disarrangement (SD-type changes), and CTD (juvenile dermatomyositis, systemic sclerosis, and Mixed CTD) in children. Spencer-Green et al found SD-type capillary changes in 11 of 19 (58%) children with dermatomyositis. In contrast, children and adolescents with primary RP and most of the subjects who developed SLE, JRA/RA, and UCTD had normal capillary findings or nonspecific capillary changes. We did not find any specific capillary changes predictive for future development of SLE, JRA/RA, and UCTD in children and adolescents with RP. These findings were similar to those of other studies in chil-dren, as well as in adults (16,29,30). Scleroderma type capillary changes in children and adolescents with RP strongly suggest the development of scleroderma spec-trum disorders in the near future. This finding gives us a chance to define, among a large number of children and adolescents with RP, a small subgroup with a high risk of development of SSD. Early detection of patients with SSD allows for an early start of proper treatment, and probably for a better prognosis.
ACKNOWLEDGMENTS
We thank Dr Zorica Sˇporcˇic´ for helpful comments on the manuscript.
REFERENCES
1. Bolster MB, Maricq HR, Leff RL. Office evaluation and treatment of Raynaud phenomenon. Cleve Clin J Med 1995;62:51–61.
2. Gareth TJ, Ariane LH, Sarah EW et al. Occurrence of Raynaud phenomenon in children ages 12–15 years. Prevalence and association with other common symptoms. Arthritis Rheum 2003;48:3518–3521.
3. Jayanetti S, Smith CP, Moore T, et al. Thermography and nailfold capillaroscopy as noninvasive measures of circu-lation in children with Raynaud phenomenon. J Rheuma-tol 1998; 25:997–999.
4. Gonzalez Pascual E, Esquinas Rychen G, et al. Raynaud phenomenon in childhood: review and progress control in eight cases. An Esp Pediatr 1998;48:603–607.
5. Nigrovic PA, Fuhlbrigge RC, Sundel RP. Raynaud phenomenon in children: a retrospective review of 123 patients. Pediatrics 2003;111:715–721.
6. Duffy CM, Laxer RM, Lee P, et al. Raynaud syndrome in childhood. J Pediatr 1989;114:73–78.
7. Maricq HR, Spencer-Green G, LeRoy EC. Skin capillary abnormalities as indicators of organ involvement in scleroderma (systemic sclerosis), Raynaud syndrome and dermatomyositis. Am J Med 1976;61:862–870.
8. Maricq HR, LeRoy EC, D Angelo WA, et al. Diagnostic potential of in vivo capillary microscopy in scleroderma and related disorders. Arthritis Rheum 1980;23:183–189. 9. Houtman PM, Kallenberg CGM, Wouda AA et al.
Decreased nailfold capillary density in Raynaud phenom-enon: a reflection of immunologically mediated local and systemic vascular disease. Ann Rheum Dis 1985;44:603– 609.
10. Maricq HR, Weiberger AB, LeRoy EC. Early detection of scleroderma spectrum disorders by in vivo capillary microscopy: a prospective study of patients with Raynaud phenomenon. J Rheumatol 1982;9:289–291.
11. Harper FE, Maricq HR, Turner RE, et al. A prospect-ive study of Raynaud phenomenon and early connectprospect-ive tissue disease. A five year report. Am J Med 1982;72:883– 888.
12. Spencer-Green G, Crowe WE, Levinson JE. Nailfold capillary abnormalities and clinical outcome in childhood dermatomyositis. Arthritis Rheum 1982;25:954–958. 13. Nussbaum AL, Silver RM, Maricq HR. Serial changes in
nailfold capillary morphology in childhood dermatomyo-sitis. Arthritis Rheum 1983;26:1169–1172.
14. Terreri MTRA, Andrade LEC, Pucinelli ML, et al. Nail fold capillaroscopy: normal findings in children and adolescents. Semin Arthritis Rheum 1999;29:36–42. 15. Herrick AL, Moore T, Hollis S et al. The influence of
age on nailfold capillary dimensions in childhood. J Rheu-matol 2000;27:797–800.
17. Damjanov N, Pavlov S, Radosavljevic V, et al. Prognostic significance of capillaroscopic findings in subjects with Raynaud phenomenon. Acta Rheumatol Belgradensia 1998;28:12–17.
18. Maricq HR. Widefield capillary microscopy: technique and rating scale for abnormalities seen in scleroderma and related disorders. Arthritis Rheum 1981;24:1159–1164. 19. Bethhencourt J, Bustabad S, Alvarez A, et al.
Immunolo-gical features and nail-fold capillary patterns in 32 cases of Raynaud phenomenon in childhood. Ann Rheum Dis 2003;62:ABO 472.
20. Greager MA, Dzau VJ. Vascular diseases of the extremities – Raynaud phenomenon. In: Fauci AS, Braunwald E, Isselbacher KJ, et al. eds. Harrisons principles of internal medicine, 14th edn. New York: McGraw-Hill, 1998:1401– 1402.
21. Saraux A, Allain J, Guedes C, et al. Raynaud phenomenon in rheumatoid arthritis. Br J Rheumatol 1996;35:752–754. 22. Grassi W, De Angelis R, Lapadula G, et al. Clinical diag-nosis found in patients with Raynaud phenomenon: a multicentre study. Rheumatol Int 1998;18:17–20. 23. Cassidy JT. The systemic sclerodermas and related
disor-ders. In: Cassidy JT, Petty RE eds. Textbook of pediatric rheumatology, 4th edn. New York: Churchill Livingstone 2001:505–533.
24. Hossny E, Hady HA, Mabrouk R. Anti-centromere antibodies as a marker of Raynaud phenomenon in
pediatric rheumatologic diseases. Pediatr Allergy Immunol 2000;11:250–255.
25. Takei S, Maeno N, Shigemori M, et al. Two cases with SLE and MCTD developed after a long period of chronic arthritis that was initially diagnosed as JRA. Ryumachi 1997;37:702–708.
26. Vuilleumier C, Sauvain MJ, Aebi C, et al. Systemic lupus erythematosus initially presenting as idiopathic juvenile arthritis with positive antinuclear antibodies. Acta Paediatr 2003;92:512–513.
27. Vayssairat M, Abuaf N, Baudot N, et al. Abnormal IgG cardiolipin antibody titers in patients with Raynaud phenomenon and/or related disorders: prevalence and clinical significance. J Am Acad Dermatol 1998; 38:555–558.
28. Meroni PL, Raschi E, Testoni C, et al. Endothelial activation by APL: a potential pathogenic mechanism for the clinical manifestations of the syndrome. J Autoimmun 2000;15:237–240.
29. Lefford F, Edwards JCW. Nailfold capillary microscopy in connective tissue: a quantitative morphological analysis. Ann Rheum Dis 1986;45:741–749.