STEPHAN ALEXANDER CASTELLANOS: The doctor/patient relationship in end-of-life care: A game-theoretic model. End-of-life care is a sensitive topic because it deals with life and death, as well as the nature of that death. In its most basic form, end-of-life care can be divided into two distinct pathways: aggressive treatment and methods or palliative care and care.
A review of the literature reveals that palliative care can in many cases increase the quality of life. An important part of the decision between aggressive and palliative care is the patient's and physician's feelings about certain aspects of end-of-life care. This article incorporates the literature into a game-theoretic model of the doctor/patient relationship at the end of life.
DUN Cheating-is-unlikely scenario, no respect DUR Cheating-is-unlikely scenario, respect MQOL McGill Quality-of-Life Questionnaire.
INTRODUCTION TO END-OF-LIFE CARE
The issue of prolonged life versus prolonged death will continue to be central to end-of-life care discussions today. David Karnofsky, a pioneering oncologist of the 1960s, was at the forefront of the aggressive treatment movement. Unlike previous meanings of terms such as palliative medical therapy, palliative measures or simply palliation, as well as related ideas such as "supportive care", this new notion of palliative care refers to a set of principles, knowledge base and proven practices, aimed at relieving pain. and end-of-life suffering and accompanying patients through their dying process” [2].
More than $80 billion is spent on end-of-life care in the United States, and nearly 50% of this amount is spent on cancer patients [9]. A 2012 Journal of Oncologic Practice study, "End-of-Life Health Care Costs for Cancer Patients," estimated that the majority of all end-of-life costs for cancer patients stem from life-sustaining measures, with 55% of all costs being costs spent for acute care in the last six months before death [12]. This statistic once again illustrates the persistence of an aggressive attitude ingrained in the oncology community since the 1950s.
Using all this knowledge - from the dichotomy of methods to the high cost of end-of-life care - the thesis will now review the literature that describes the effect that certain factors can have on the implementation of end-of-life care.
VARIABLES TO BE CONSIDERED IN IMPLEMENTATION
This section presents five recent studies on the topic of advanced directives and end-of-life counseling. Of the 46 patients with advanced directives on file, 32 stated that they would not want heroic end-of-life interventions. Once identified, members of the intervention group would be contacted by telephone by a nurse trained in end-of-life counseling.
This study is not alone in finding significant savings associated with advanced directives and end-of-life discussions. Rather, each patient was free to make his or her own decision regarding end-of-life care. One such study found an inverse relationship between a person's expenses at the end of life and his or her quality of life [3].
The main goal of this thesis is to create a game-theoretic model of the doctor/patient relationship at the end of life.
THE GAME THEORETIC MODEL
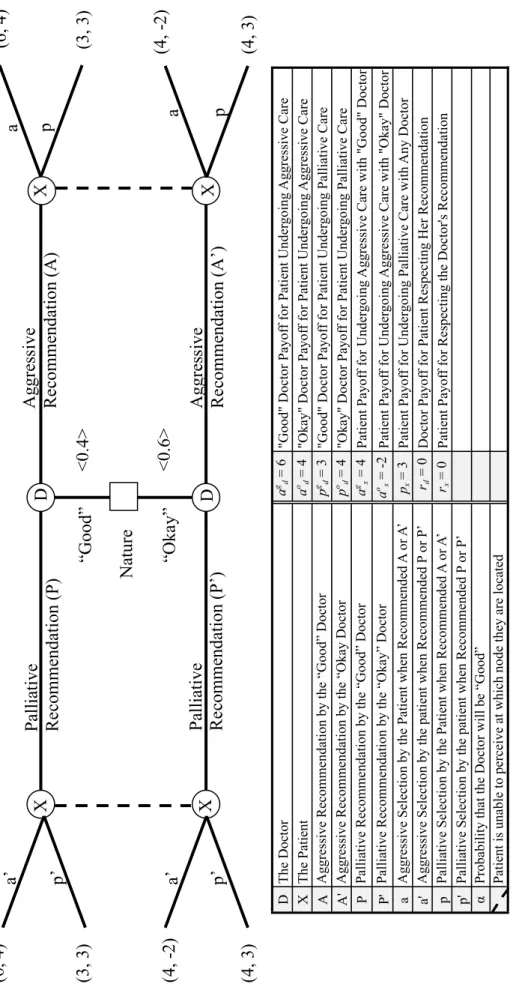
This thesis develops a game-theoretic model of the doctor/patient relationship at the end of the patient's life. In the game, there are two states of the world: one where the Doctor is "good" and one where the Doctor is "okay" - while the terms "good" and "okay" are somewhat arbitrary, they serve to indicate a key difference in the Doctor's ability to correctly to diagnose the patient's condition. Only the doctor knows the state of the world where the game is played.
The doctor then recommends palliative or aggressive treatment to the patient, and the patient can accept or reject the doctor's advice. For the sake of clarity, the doctor has been referred to with a female pronoun, and the patient with a male pronoun. Here, the doctor is "good" if she has had considerable experience with critically ill cancer patients, gives.
The doctor is "okay" if she has had less experience with critically ill cancer patients, resulting in lower recovery-to-discharge rates when AAMM procedures are used. The probability that the doctor will be "good" is denoted by α, and the probability that the doctor will be "okay" is denoted by (1-α). In the second phase, the doctor recommends an aggressive treatment plan or a palliative care plan.
It is important to note that the prime in the doctor's decision notation distinguishes between whether the doctor's type is "good" or "okay", while the prime in the patient's decision notation indicates that the doctor recommended palliative care. Although the payoffs in each scenario are highly qualitative, they are intended to be a fairly accurate depiction of both the doctor's and the patient's relative well-being in the given outcome. It is important to note that these payouts are independent of what the doctor actually recommends, ie.
The QOL component is determined by the patient's treatment choice and the type of physician, and the values were based on the literature. The parameter agx indicates the patient's payoff when undergoing aggressive treatment and the doctor's type is "good", and aox indicates the payoff to the patient with the same choice when the doctor's type is "okay".
THE SCENARIOS
It represents a scenario in which the "good" doctor recommends aggressive care and the "okay" doctor recommends palliative care, and then the patient respects the doctor's opinion in both cases. Under (PP', pp'), "good" and "okay" doctors recommend palliative care, and the patient chooses to undergo that palliative care when it is recommended. Since the Nash equilibrium is (PP', pp'), the patient expects the physician to always recommend palliative care.
So, if the doctor recommends aggressive care, the patient is not sure what to believe. In this scenario, the doctor is able to signal her type - "good" or "good" - to the patient through her choice of recommendation. Under (PP', pp'), both the "good" and "ok" doctors recommend palliative care, and the patient respects that opinion, choosing to undergo palliative care when it is recommended to him.
Equilibrium also indicates that the patient will choose palliative care if aggressive care is recommended. Since the probability that the doctor is "right" is 0.6 in this scenario, the prospect of patient fraud is likely. This conclusion makes sense because since the patient is rational and he knows that the doctor is rational, he knows that the "right" doctor strongly prefers aggressive care.
So, if the doctor recommends palliative care, the patient is not sure what to believe. As in the baseline scenarios, this equilibrium creates a situation where the patient expects the doctor to always recommend palliative care. Among them, both the "good" and "ok" doctors recommend aggressive care, and the patient then respects the doctor's opinion and opts for aggressive care when it is recommended to him.
In the state of the world where the doctor is "good", the patient will choose palliative care after one. Similarly, in the state of the world where the doctor is "okay", the patient will choose palliative treatment following a palliative recommendation, because 5 > -2. In the case of the "good" doctor, the patient prefers palliative treatment to aggressive treatment when the doctor recommends aggressive treatment because 4.5 > 4.
Similarly, in the case of the “good” doctor, the patient prefers palliative care to aggressive care, while the doctor recommends aggressive care, because 4.5 > -2.
IMPLICATIONS AND CONCLUSION
The doctor then recommended palliative or aggressive treatment to the patient, and the patient could accept or reject the doctor's advice. While the patient gained utility from undergoing aggressive care with the "good" physician and also from undergoing palliative care with both parties, the patient always derived disutility—that is, negative utility—from undergoing aggressive care with the "okay" physician. In one, the "good" doctor recommended aggressive treatment and the "okay" doctor recommended palliative care, with the patient following each doctor's recommendation.
There was also a situation where the patient always chose palliative care, and the doctor always recommended it. The next four scenarios introduced the concept of deception, with the doctor now not wanting the patient to know her type. This was because the "okay" doctor now preferred aggressive care even more than the "good" doctor, and the patient was not in favor of that outcome.
Because the patient did not respect the physician's opinion, he instead used his exogenous beliefs to make care decisions. Here, the patient's perception of this likelihood caused him to be willing to take the risk that he might be dealing with an "okay" physician, and to choose aggressive care in each situation. This produced the same result, so that both the patient and the doctor choose palliative care in every situation, but now there were more reasons behind it.
Here, in what was determined to be the logical balance, "good" and "okay" doctors would recommend aggressive care, and the patient would choose aggressive care with that recommendation, even if surprised by a palliative care recommendation. . Unlike the similar outcome of the aggressive "okay" scenario, here the patient is choosing to undergo palliative care as a result of their own preference and not out of fear of being tricked into doing something they don't want to do. It is also worth noting that the patient derives his highest utility in the model from the outcome of the counseling scenario—in the situation where he undergoes palliative care in any state of the world as a result of his unforced choices.
It should be noted that it is not the argument of this paper that everyone should undergo palliative care in every situation - this is a decision that should remain in the hands of the patient after consultation with their doctor. However, this paper has effectively demonstrated—both through its model and a literature review—that effective advance directives and counseling are key to enhancing the patient's quality of life at the end of life.







