Cathy Hamilton BSc(Hons), MSc, RGN, RM, PGDip, PGCert is Senior Lecturer in Midwifery at the University of Hertfordshire and Supervisor of Midwives. Celia Wildeman SCM, DipNS, ADM, PGDC, PGDSPCF, Supervisor of Midwives is Senior Lecturer in the Department of Nursing and Midwifery at the University of Hertfordshire.
Ian Peate and Cathy Hamilton
The unique role and function of the midwife
A midwife is a person who has been regularly admitted to a midwifery training programme, is duly recognized in the country in which it is established, has successfully completed prescribed midwifery training and has acquired the necessary qualifications to be registered and/or has a legal license to practice midwifery.'. The midwife is the senior professional who attends more than 75 per cent of births in the UK; she provides full care to mother and baby from the beginning of pregnancy, during labor and until the baby is 28 days old (Medforth et al. 2006).
The midwife’s role in public health
The midwife is ideally placed to influence and implement public health policy by working with women and their families and to develop a population perspective in midwifery. Midwives make an important contribution to public health by promoting the long-term well-being of women, their children and their families.
Terminology
All chapters in this text relate to midwifery practice and as such are rooted in public health. Public health in midwifery is not new; midwives have always provided public health-focused care.
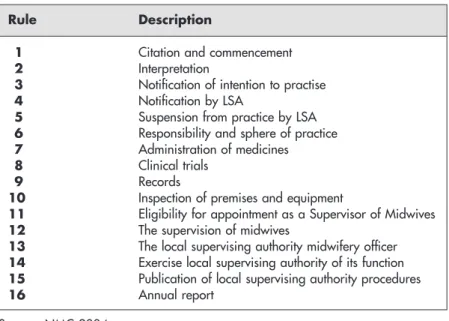
The Nursing and Midwifery Council and Quality Assurance (Education)
Each pre-enrolment midwifery course must demonstrate explicitly and properly that it has incorporated the rules and standards of the NMC, so that those who follow a recognized course are eligible for enrolment. The Nursing and Midwifery Decree 2001 requires the NMC to set rules and standards for obstetrics and Local Supervisory Authorities (LSAs) for the function of statutory supervision of midwives.
Becoming a profi cient midwife
In addition to meeting the NMC age requirement, general entry requirements must also be met. The method of determining these requirements is within the competence of the educational institution; however, the NMC must agree to and allow these requests.
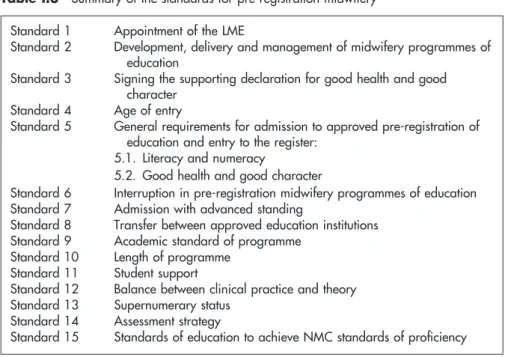
The profi ciencies
These vary from the appointment of the LME to standards of skill (see Table I.3). This text will address the standards of competence for entry to the register for midwives.
Case notes and activities
Effective Communication
Tandy Deane-Gray
Introduction
This can be observed in the first hour after birth and it is this response to adults that makes the baby a social and communicative being as they will take turns showing in their nonverbal responses and vocalisations (Murray and Andrews 2000) provided the adult is sensitive to it. Our early communication skills are captured in patterns, and the foot stomping from a toddler's tantrum may still be visible in the adult.
Some common problems in communication
For example, if you say "You can go home after the pediatrician has released the baby," the client may only hear "You can go home." However, paradoxically it causes anxiety as the client is denied the opportunity to express how they really feel (Stapleton et al. 2002).
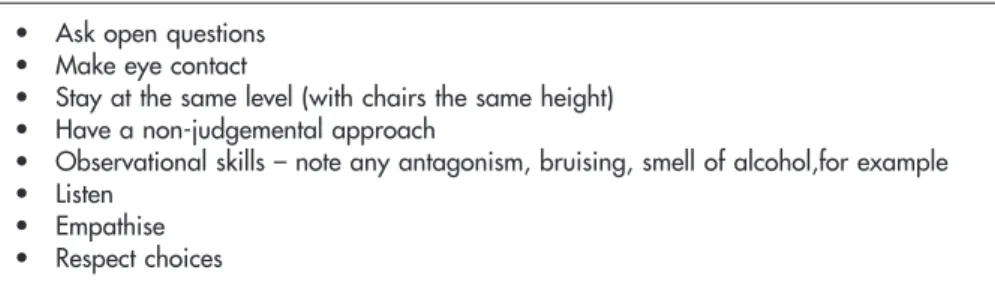
Listening
Remember what is said as if you are to be tested on it. I'm sorry you've been waiting so long, it must be very frustrating for you.
Empathy
One of the difficulties is that it is easy to be sympathetic and the midwife can identify with her own feelings that the client's message evokes. How do you imagine you would feel if you were student A. Student B: Oh, maybe they work hard, it's just that I'm a single parent so I have to find time, while others don't have this responsibility.
Acknowledgement
It seems clear that many of the midwifery issues discussed here would be reduced or avoided if this standard were fully adopted. We achieve this through intimate and sensitive communication between midwives and their clients. 2006) Shadow work in midwifery: an unseen and unrecognized emotional birth.
The Aims of Antenatal Care
Laura Abbott
The midwife’s role as antenatal caregiver
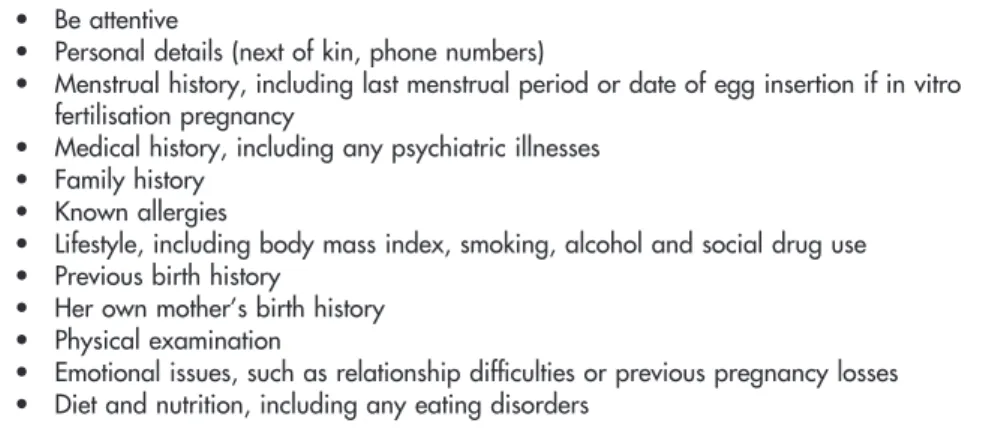
Antenatal assessment and monitoring
The booking visit will provide an overall picture of the woman's physical, psychological and social needs. The woman can refer directly to the obstetrician and does not have to register with her GP.
Emotional well-being
If the woman works, employment issues can be discussed and the woman may want to know her rights in relation to work or self-employment. If this is your first time meeting the woman, she may not want to disclose information right away.
Medical and family history
For example, if she has a history of thrombosis, she may be at risk for blood clotting disorders such as deep vein thrombosis or pulmonary embolism during pregnancy and may need to be offered the services of an obstetrician. If she has a history of severe mental illness, such as psychotic disorders, or a history of postpartum illness, a team approach may be needed to offer her appropriate care during pregnancy and support after the birth of the baby.
Subsequent visits
Record-keeping
These tests are not mandatory. among other things) on the standards of its record keeping. The Confidential Inquiry into Stillbirths and Infant Deaths (DH 1998a), the Confidential Inquiry into Maternal Deaths (DH 1998c), the NMC (2002) and the Health Services Ombudsman (DH 1999) all cite poor record-keeping standards. in the many cases that have been investigated.
Tests offered at subsequent visits
The NMC's 2003 annual report notes that the second highest category for removal from the professional register was failure to keep accurate records and the Health Service Ombudsman (DH 1999) equates poor record keeping with poor standards of care. Chapter 10 further discusses the important issue of effective documentation and Chapter 14 examines confidentiality.).
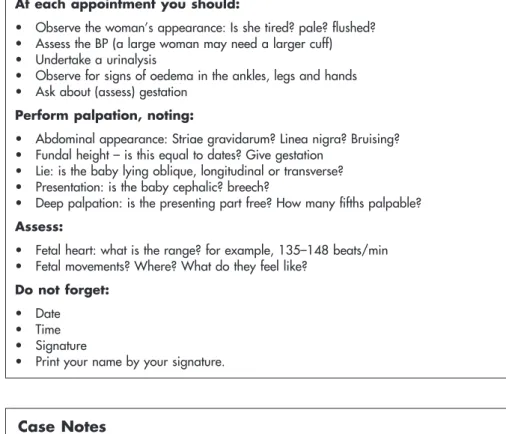
Assessments at each visit
Wickham (2002a) explains that if the number of beats is the same, the baby may be asleep. Auscultation with Pinard gives you several clues about the position of the baby.
Screening
In general, try to hear the FH through the back of the fetus (remember, the baby's lungs are not inflated). Ask about the baby's movements as you palpate, this will help you determine the position.
Conclusion
Respecting the choices women make and valuing the woman as an individual helps to provide personal care. Department of Health (1998b) Information for Health: An Information Strategy for the Modern NHS A National Strategy for Local Implementation.
Programmes of Care During Childbirth
The National Service Framework (NSF; DH 2004) standard for maternity services states that midwives should be the first port of call for women when they learn they are pregnant. It is essential that the midwife is aware of the choices a woman can make and provides her with up-to-date information so that she can make informed decisions in partnership with the midwife.
Place of birth
In terms of medical facilities, if intervention is required, the birth centers are the same as what is expected of a home birth - the woman would be transferred to a hospital, just like if she moved away from home. Reduced incidence of shoulder dystocia (when the baby's shoulder is affected behind the woman's pubic bone).
Independent midwives
I felt that having a relationship of trust with my midwife made a big difference. By the time I was released from my midwife's care, I felt I had put the ghost of my first birth to rest and could move on with family life.
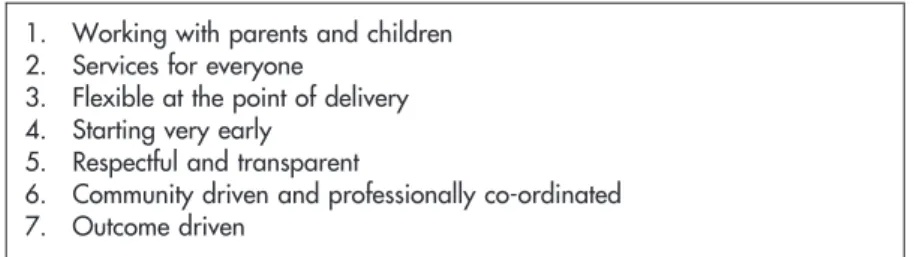
Sure Start programmes of care
I have been asked to attend the above client's home birth and provide all antenatal and postnatal care. See Tables 3.5 and 3.6 for the seven principles of safe start of care and the goals of safe start.
Parenthood education programmes
Active birth courses are chargeable and run by antenatal teachers who have been trained at the Active Birth Centre. Many exercise and yoga classes are aimed at women, involving the couple in childbirth preparation and education.
Birth plans
The latest NMC guideline states that it is the midwife's duty to support and respect the woman's choice. The NMC (2006a; http://www.nmc-uk.org/aFrameDisplay.aspx?DocumentID.=1680) notes that withdrawing a woman's choice of a home birth is similar to the NHS withdrawing hospital services Trust.
When to call the midwife
There are different ways midwives can practice midwifery, from working within a hospital or birth center to working outside the NHS as an independent midwife or caseload for a group of women. An ethnographic study of women's experience of partnership case-midwifery practice: the professional as a friend. 2005) Birth center care: a review of the literature. 2004) Outcomes of freestanding midwifery-led birth centres: a structured review of the evidence.
Interdisciplinary Working: Seamless Working within Maternity Care
Eileen Huish and Lisa Nash
Seamless care
The dietitian, especially for a woman who has diabetes, is overweight or has an eating disorder. The surgical team if you are caring for a woman who needs surgery during pregnancy or postnatally.
The Northwick Park Report
Poor communication and working relationships were found across all staff groups, which exacerbated the high attrition rate. Training and skills for staff caring for women after surgery or who require invasive monitoring.
Collaborative working
Throughout your education and future career, try to identify barriers to collaborative work and try to overcome them. During your training, Interprofessional Education (IPE) will help you prepare for collaborative work and will be discussed in more detail later in this chapter.
Conceptualising teams
Professionalism dictates that the same standard of care should be delivered to a user of the service, regardless of the practitioner's attitude toward that person.
Service user involvement
Functioning teams
During the storm phase, the individuals compete with each other for their position on the team. Any disagreements are resolved within the team and the manager to set tasks for individuals.
Team roles
Consider the consequences if the team never gets beyond the storm phase and refer back to the Northwick Park report. Try to transfer what you have learned about teamwork in the classroom to the practice environment.
Referral and handover
Remember that a paramedic observed the woman in a completely different situation and may have important information that should not be ignored. For example, the counselor may have witnessed aggressive behavior from the woman's partner, leading to suspicion of domestic violence.
Interprofessional education
Discuss your IPL opportunities with your mentor/link tutor at the start of each of your internships. Continue to reflect on your IPE experiences and interprofessional working throughout your career as it should be part of your ongoing professional development.
Intrapartum Care
Annabel Jay and Cathy Hamilton
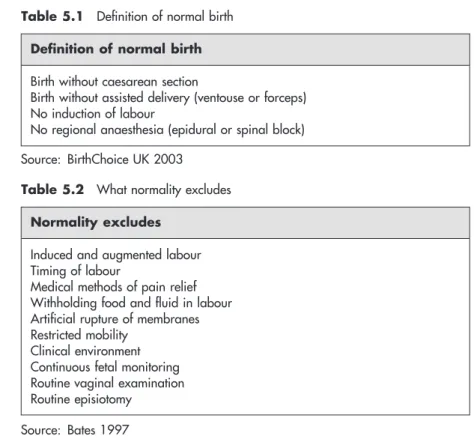
Defi nitions of ‘normal’
However, most people are likely to consider normal birth somewhere between these two extremes (Mead 2004). For statistical purposes, the Government has adopted the definition of normal birth proposed by BirthChoice UK (see Table 5.1).
Stages of labour
Promoting spontaneous labour – avoiding induction of labour
This procedure can be done in an antenatal clinic or at the woman's home and can cause a "show". slightly bloody mucous discharge) and some mild cramping afterwards. Current NICE guidelines recommend that debridement be offered prior to any induction procedure (NICE 2001).
Onset of spontaneous labour
Research shows that a sweep increases the chances of labor starting spontaneously within the next 48 hours and can reduce the need for other methods of induction (NICE 2001). This is only possible if the cervix is already open enough to admit a finger.
Signs that labour has started
Approximately 6-19 percent of women will experience spontaneous rupture of the membranes before labor begins (Tan and Hannah 2002). Spontaneous rupture of the membranes can be recognized by the sudden loss of a significant amount of clear fluid from the vagina.
Midwifery care in early labour
The midwife will need to take a careful history of the woman and usually continued observation of fluid being lost from the vagina will lead to definitive confirmation that spontaneous rupture of the membranes has indeed occurred. The midwife may suggest to the woman that she has a warm bath to help her relax, that she tries to rest as much as possible and that she eats a light meal and drinks plenty of fluids to prepare herself for the start of labour. the active phase of labour.
Initial examination
These recordings should be noted in the woman's records as they will serve as baseline readings as labor progresses. A sample of the woman's urine should be tested at admission and then regularly during labor.
Assessment the progress of labour
The presence of ketones (ketonuria) indicates that the woman has not eaten for some time or suffered from excessive vomiting. An abnormality in any of these readings should be reported to the obstetrician as it may indicate an underlying problem with the general health of the woman or with the progress of her labor.
Observation of the woman’s behaviour
Outward signs
A woman can involuntarily defecate at this time if her rectum is full, as the pressure of the upcoming part tightens the rectum against the sacral bone and expels any contents. Therefore, the spontaneous rupture of the membranes during an uncomplicated birth, which until then had proceeded normally, can mean the end of the first period of labor.
Observation of woman’s psychological state
Abdominal palpation and auscultation
Monitoring of contractions
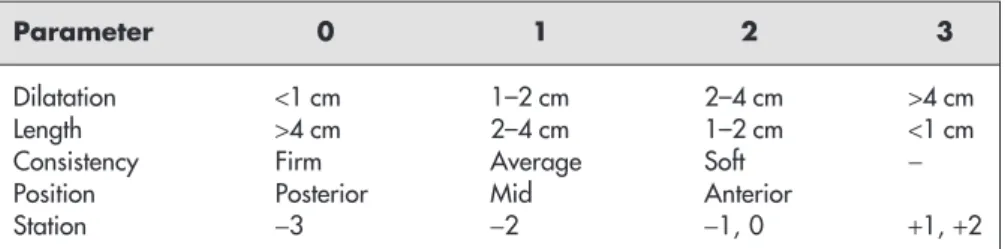
Vaginal examination
Even if the cervix is closed, the midwife can determine the descent of the presenting part (PP) through the pelvis. If the cervix is sufficiently dilated, the midwife can assess the position (bowed or bowed) of the fetal head by feeling the fontanelles.
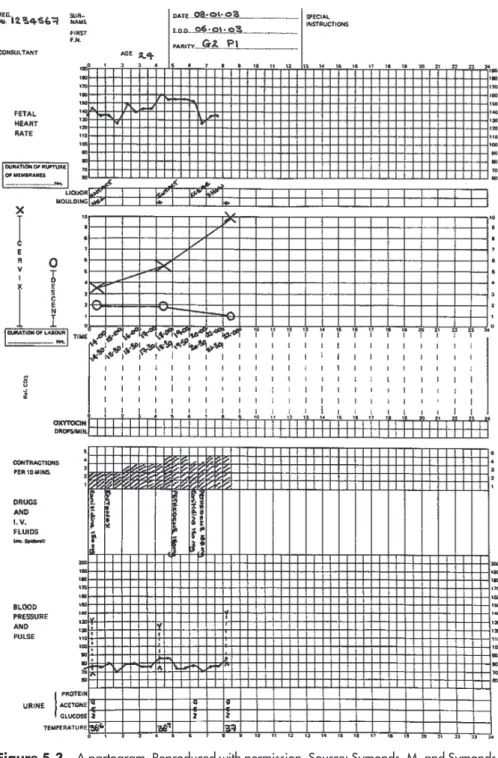
The partogram
The position of the fetus can be determined by palpation of the sutures on the fetal skull. By noting the position and direction of the sutures, the obstetrician can judge whether the fetus turned in a good position for birth.
Medical forms of pain relief
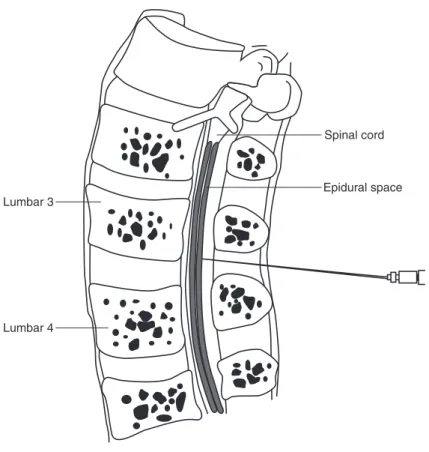
In this way, the maximum effect of the pain reliever will coincide with the peak of the contraction. The local anesthetic is placed in the space with the aim of surrounding the fibers of the spinal nerves to block the pain sensations.
Administration of epidural anaesthesia
Disadvantages of epidural use
As the CSF leaks out, it causes a drop in pressure in the brain that results in a woman experiencing a severe headache, which is worse when she sits down. This causes a loss of sensation and movement in the woman's upper body and will affect the muscles needed for breathing.
Opioid analgesia
Another disadvantage of using pethidine during labor is that it easily crosses the placenta. It has been demonstrated that there are no significant differences in the analgesic and side effects of the two drugs, but that meptazinol induces more vomiting (Sheikh and Tunstall 1986).
Midwifery care in the fi rst and second stages of labour
In the second half of the twentieth century, many maternity units introduced restrictions on eating and drinking during labour. This was once common practice in the UK, but there is currently no evidence to support this.
Midwifery care in the third stage of labour Physiological or expectant management of
Sintometrine (1 ml) is an oxytocic that is often used in the active treatment of the third stage. In this case, the midwife will give the medicine after the baby is born.
Midwifery care after birth
This chapter has focused on the physiological aspects of childbirth with emphasis on the midwife's role in promoting normality. Obstetrics by ear: maternal and caregiver perceptions of the meaning of maternal sounds during the second stage of labor. 2004) Midwives practicing in 11 UK maternity wards.
Effective Emergency Care
Caroline Duncombe, Meryl Dimmock and Sarah Green
These promote multidisciplinary teamwork, which is a requirement of the Clinical Negligence Scheme for Trusts (CNST). These drills should include identification of required equipment and methods to ensure that appropriate emergency help, including cardiac arrest teams, arrives promptly (CEMACH 2004).
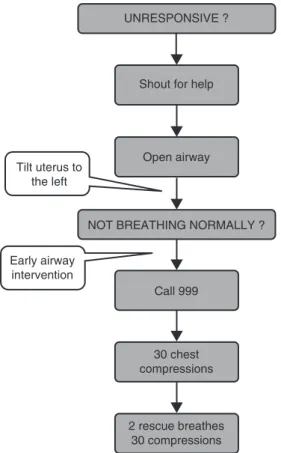
Maternal resuscitation
This happens when a doctor (who can be a midwife or another helper, eg a doctor, healthcare assistant or partner) manually removes the weight of the uterus on the woman's left. Apply pressure to the cricoid cartilage to seal the upper end of the esophagus against the vertebrae and prevent aspiration of acidic stomach contents.
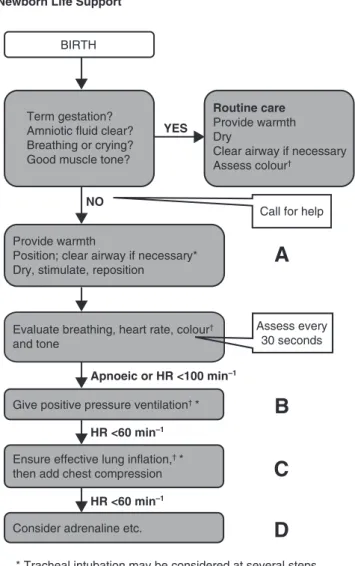
Neonatal resuscitation
The baby should be placed on his back with the head in the neutral position, i.e. a folded towel can be placed under the shoulders to aid in positioning if the baby has a prominent occiput.
Shoulder dystocia
Pressure is exerted by the midwife or an assistant on the mother's abdomen, on the baby's back, in a downward direction towards the side of the mother on which the baby is. The midwife can also reach in with the other hand to apply pressure to the front side of the back shoulder to ensure better rotation.
Vaginal breech delivery
It is commonly thought that the bottom of the baby is smaller than the diameter of the head and can pass through a cervix that is not fully dilated. If necessary to help this process, the baby should be supported by the hips.

Manual removal of the placenta
A gentle cutting motion with the edge of the hand should be used to continue separating the placenta until it is detached. If the placenta cannot be separated easily, heavy bleeding or perforation of the uterus may occur.
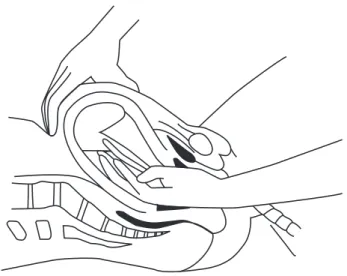
Management of postpartum haemorrhage
A team member takes frequent pulse and blood pressure readings to monitor the woman's condition. This is done by inserting one hand into the vagina, then making a fist against the body of the uterus inside.
Management of an eclamptic seizure
This could be one of the first signs of preeclampsia and occurs in 30 per cent of preeclamptic pregnancies (RCOG 2006). Preeclampsia/eclampsia remains one of the leading causes of maternal death in the UK.
Initial Assessment and Examination of the Newborn Baby
Lyn Dolby
The midwife’s immediate role
Conversely, the condition of the baby may not be good at birth or there may be an obvious physical abnormality. The midwife is responsible for assessing and recording the baby's initial vital signs (see later in this chapter), thus providing a comprehensive record of the baby's condition at birth and during the first hours of life.
The initial assessment and examination at birth
The screening process should be explained to the parents and their consent obtained. The dorsal (top) of the foot should easily line up with the anterior (front) side of the foot.
Completion of the initial examination
The baby should be weighed at the beginning or end of the exam as long as the baby remains warm. Many units do not routinely measure the baby's length due to the logistics of ensuring the accuracy of the measurement.
Effective Postnatal Care
Annabel Jay
Principles of postnatal care
Individualised care
Judy has two teenage daughters from a previous marriage, but Harry is Deepak's first child. Since Judy is a "multip" with good family support, the midwife assumed she wouldn't need much help or advice.
Record keeping and communication
Keeping detailed records in the woman's handwritten notes will facilitate continuity of care between caregivers. The midwife must take the time to listen and allow the woman to talk about the birth as she wishes.
Immediate post-birth care of the woman
Reference must be made in the woman's notes to the time when the urine was passed and the volume passed, if measured. The procedure must be explained to the woman and verbal consent obtained before commencing.