It contained air pumped down from the surface after the development of efficient air pumps around 1800 AD. Paul Bert, a French scientist, was the first to explain that the disease was caused by the formation of nitrogen bubbles in the body and proposed the idea of a slow rise to the surface.

PHYSICS
PRESSURE
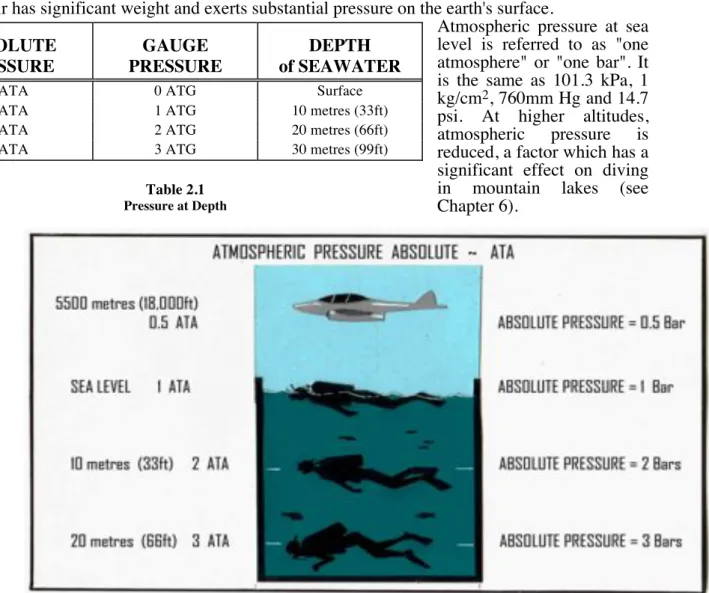
The total pressure exerted on a diver at depth will be the pressure due to the atmosphere acting on the surface of the water (atmospheric pressure) plus the pressure due to the depth of the water itself (hydrostatic pressure). The partial pressure contributed by each gas is proportional to its percentage of the mixture.
GAS LAWS
Each gas contributes the same proportion to the total pressure of the mixture, as does its share of the composition of the mixture. This means that if the pressure of gas exposed to a liquid increases, then more gas will dissolve in the liquid.
GASES OF IMPORTANCE TO DIVERS
It is called an "inert gas" because it does not participate in human biochemical processes. It is sometimes used with very low O2 percentages, at great depths, by skilled professional divers.
BUOYANCY
The ancient Greek, Archimedes (apparently while lying in his bath), discovered that when an object is immersed in a liquid, it appears to be lighter, and that the apparent loss of weight (or buoyancy) equals the weight of water displaced. by the object. That is to say – the buoyant effect will be equivalent to the weight of liquid with equal volume to the submerged object.
PHYSICAL EFFECTS OF THE ENVIRONMENT
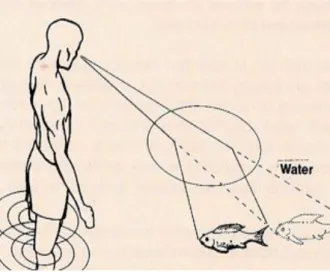
Even a sinking object will still appear lighter than it would out of liquid. The clear focus of the eye depends greatly on the refraction of light rays that pass between the air in front of the eye and the cornea (the clear surface at the front of the eye).
PHYSIOLOGY*
METABOLISM
RESPIRATION
The lungs occupy a football-sized cavity on each side of the chest. Only about 10% of the air in the chest is exchanged with each breath during quiet breathing.
CARDIOVASCULAR SYSTEM
The heart is a large muscular pump (about the size of a man's fist) located in the center of the chest. The left side of the heart receives this oxygen-rich arterial blood from the lungs and pumps it throughout the body.
COMPRESSED-AIR DIVING
Blood flow from the heart is pulsatile and blood pressure varies depending on the phase of heart contraction. Excessively high blood pressure (hypertension) can eventually cause damage to blood vessels and put too much strain on the heart.
BREATH-HOLD DIVING
This is probably because the partial pressure of O2 in the lungs increases as they are compressed. There is a corresponding increase in the partial pressure of O2 in the blood, which will reduce the hypoxic stimulus for breathing.
DIVING EQUIPMENT
FREE DIVING EQUIPMENT
In a significant proportion of diving accidents, the diver fails to release the weight belt at the time of the emergency. It should be attached to the diver in a place where it cannot become snagged (for example, the inside of the calf or arm) and is easily accessible.
COMPRESSED GAS DIVING EQUIPMENT
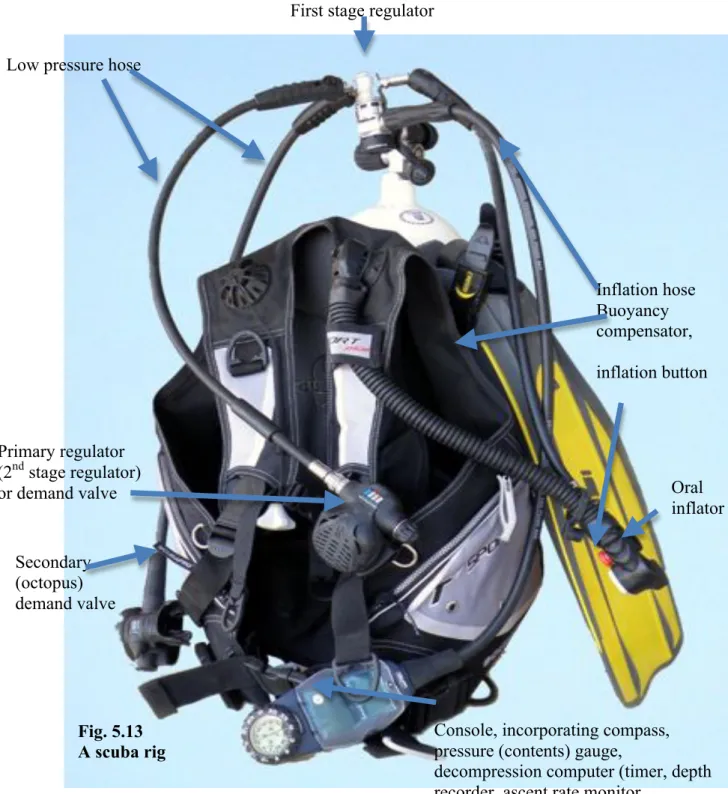
SCUBA
When inhaling, a diaphragm moves to open a valve in the demand regulator, and air flows from the air hose to the diver, below ambient pressure. The gas outlet from the cylinder to the regulator is controlled by a high-pressure valve or tap.
HOOKAH and SSBA
STANDARD DRESS or HARD HAT
It uses a smaller, lightweight fiberglass or aluminum helmet or mask along with a dry or heated wetsuit, allowing the diver to swim and move more freely. The diver usually breathes gas mixtures, which include helium, to prevent the development of nitrogen narcosis.
REBREATHING APPARATUS
ANCILLARY DIVING EQUIPMENT
Ideally, there should be a separate emergency supply of inflation gas - this can either be a CO2 cartridge or a small compressed air cylinder. However, with most of these devices it is difficult in an emergency to drop an empty scuba tank on the surface without losing the B.C.

BUOYANCY OVERVIEW
Unfortunately, in the event of an underwater emergency, it is much slower as the air supply also decreases due to the effect of Boyles' law. The safety of the buddy system in diving depends on the two divers communicating with each other continuously.
STAND-BY DIVER
DIVING
ENVIRONMENTS
WATER MOVEMENTS
The best technique is to swim against the current during the first half of the dive and use it to float back to the boat during the second half. Another rope (a floating or Jesus line) should drift with the current from the back of the boat, for a distance of 50 meters or more.
ENTRAPMENT
The return to the cave entrance is marked by a line delivered from a reel by the dive leader, who enters first. The vertical passage to the surface is marked by a heavier bulkhead line, making it less likely for the diver ascending hastily to become entangled.
ENVIRONMENTAL VARIANTS
The critical difference, however, is that the diver in the lake returns to a lower surface pressure. In the mountain lake, because the surface pressure is only half that of sea level (0.5 ATA), the diver only needs to dive to 5 meters (1 ATA) and return to the surface to encounter the same 2:1.
STRESS DISORDERS, PANIC & FATIGUE
INTRODUCTION
PERSONALITY FACTORS
Although the failure rate for military and commercial diving courses is high, the failure rate for many recreational diving courses is close to zero. The standards set by some diving organizations are of concern as they may be too influenced by commercial considerations.
STRESS RESPONSES
There was a tidal current coming through which slowed their progress to the planned end of the dive - the safe exit point. For the assisting diver, it is usually prudent to ensure their safety and the integrity of their equipment as a priority.
THE FEMALE DIVER
Statistically, there is some reason to believe that diving-related incidents are more frequent around the time of menstruation. There is no correlation between the development of DCS and the consumption of oral contraceptives per se.
PREGNANCY
The circulation of the fetus contains a channel (the ductus arteriosus) that allows blood to bypass the lungs. Due to the unique circulation of the fetus, even a few bubbles in the fetal circulation can have disastrous consequences.
BAROTRAUMA
ANATOMY OF THE EAR
The mastoid sinuses (air pockets in the mastoid bone) also exit the middle ear. The middle ear communicates with the outer and inner ear by transmitting sound from the outer ear to the inner ear.
THE MECHANISM OF HEARING
The tympanic membrane (or tympanic membrane) is connected by the three small ear bones or ossicles - malleus, incus and stapes - to the oval window across the middle ear space. The outer (air) and middle ear (ossicles) thus conduct sound waves to the inner ear.
EXTERNAL EAR BAROTRAUMA
These vibrations are transmitted and amplified by the bony chain system of handles, to the oval window. Damage to the outer ear and middle ear disrupts the conduction of sound waves to the inner ear and therefore causes conductive deafness.
MIDDLE EAR BAROTRAUMA OF DESCENT
Fluid can also be felt trickling down the throat after it has run down the Eustachian tube from the middle ear space. Crackling sounds (especially during chewing, swallowing or jaw movements) may also be heard, caused by air bubbles in the blood/body fluid mixtures in the middle ear.
PREVENTION OF BAROTRAUMA
This usually causes the Eustachian tubes to open momentarily, allowing air to enter or leave the middle ear. By that stage, the middle ear mucosa is already swollen and obstructing the Eustachian tube, making equalization more difficult.
MIDDLE EAR BAROTRAUMA OF ASCENT
If the use of these hoods is necessary, it is better to have holes above the ear that will allow air and water movement and pressure. Special earplugs and masks used to prevent ear barotrauma probably work only to delay the damage and thus cause fewer symptoms—not to prevent the damage.
INNER EAR BAROTRAUMA
Straining, sneezing, blowing the nose, sexual activity, loud noise and clearing of the middle ear should be avoided to prevent pressure waves in the inner ear. In the absence of a round window fistula, no specific treatment is available for this type of injury.
SINUS
ANATOMY OF THE SINUSES
Each sinus communicates with the nose by its own narrow opening called an ostium, and through these, the sinuses are permanently open to the atmosphere. More often it reflects the pathology of the middle ear and for this it should be referred to chapter 9.
THE MECHANISM OF SINUS BAROTRAUMA
During ascent, blood and tissue fluid from the sinus barotrauma of descent may enter the nose or back of the throat as gas expands in the sinus, causing an apparent epistaxis on the same side as the injured sinus. If the sinus opening is obstructed during ascent, the expansion of gas flattens the sinus lining against the bony wall, causing pain and injury to this delicate tissue.
CLINICAL FEATURES
This tissue fluid and blood, which may take days or weeks to be absorbed, provides a rich nutrient medium for bacterial growth, promoting sinus infection (see Chapter 28).
TREATMENT
PREVENTION
PULMONARY BAROTRAUMA
Air bubbles trapped in the skin circulation cause white or purple spots (marbling). Anything that prevents air from leaving all or part of the lungs can cause pulmonary barotrauma.
OTHER
BAROTRAUMAS
FACIAL BAROTRAUMA OF DESCENT
This condition is easily prevented by blowing out the face mask during descent to equalize the mask with the water pressure. Face masks can cause similar bleeding of the eyes, but then the tissues around the face are also bruised.

SKIN BAROTRAUMA OF DESCENT
BODY BAROTRAUMA OF DESCENT
SUIT BAROTRAUMA OF ASCENT
GASTROINTESTINAL BAROTRAUMA
DENTAL BAROTRAUMA
DECOMPRESSION PHYSIOLOGY and
SUSCEPTIBILITY
GAS UPTAKE
As the tissue takes up the gas, uptake slows down because the partial pressure gradient is reduced. Half-life is the time it takes for a tissue to reach half its saturation level.
GAS ELIMINATION
Other tissues such as ligaments, tendons and fat, with a relatively small blood flow, have a relatively slow N2 uptake. A fast tissue may have a half time as little as a few minutes, while a slow tissue may have a half time of several hours.
SATURATION
BUBBLE FORMATION
At the onset of DCS, the N2 pressure in the tissue is supersaturated (greater than ambient pressure) so there is an immediate diffusion (pressure) gradient of N2 which then diffuses into any bubbles (or nuclei) present, caused their expansion. . Many other biochemical and physiological changes of ill-defined consequences occur in tissues and blood vessels during decompression and DCS.
DIVE PROFILES
FACTORS INFLUENCING DCS
In theory, it may be better to keep yourself cool during the dive and warm during the decompression, unless blistering occurs. Even with repeated dives, there may be residual physiological effects from the previous dive, increasing the likelihood of decompression sickness.
DECOMPRESSION TABLES & METERS
Towards the end of the last century, recreational diving increasingly included repetitive and multi-level diving. However, the decompression of infinitely variable multi-level diving is almost entirely based on theory.
DECOMPRESSION METERS and COMPUTERS
By removing the tables rounding the safety factors, the price divers pay for their increased duration underwater is that they can dive much closer to the DCS limit. Most of the new DCs are (like the old SOS gauges) conservative for short single shallow dives.
PREVENTION of DCS
Do not assume that the DC is accurate for diving at altitude or for altitude exposure (flying). For those divers who are more important, or more susceptible to DCS (age, sex, fitness, weight, medications, injuries, DCS history, etc.) or who undertake more dangerous dives (depth, duration, decompression obligation, temperature, currents, repetitive, multiple takeoffs, etc.), the more conservative modes on the DC should be selected.
DECOMPRESSION SICKNESS
ACUTE DECOMPRESSION ILLNESS (ADI)
CLASSIFICATION OF SYMPTOMS
ONSET OF SYMPTOMS
JOINT PAIN
MUSCULO-SKELETAL DCS, BENDS)
NEUROLOGICAL DCS
Swelling of the brain (cerebral edema), as well as the expansion of the nitrogen bubbles themselves, often leads to a constant worsening of this condition. The part of the brain responsible for coordination (the cerebellum) can also be affected, causing a lack of coordination known as "wandering".
INNER EAR DCS
Numbness or tingling (paresthesias), weakness or paralysis of a limb or one side of the body, speech problems, visual disturbances, confusion, loss of consciousness or convulsions are all possible symptoms of this serious condition. It can also be preceded by 'girdle pain' - or pain around the chest or abdomen.
LUNGS or PULMONARY DCS
SPINAL DCS has a common association with DCS bubbles in the blood and lungs, commonly known as "chokes". Movement disorders such as weakness or paralysis or sensation disorders such as numbness or tingling are also common.
HEART or CARDIAC DCS
GASTROINTESTINAL DCS
SKIN MANIFESTATIONS of DCS
GENERAL SYMPTOMS of DCS
DELAYED SYMPTOMS of DCS
EVOLUTION OF SYMPTOMS
Give the patient an address and ask him or her to repeat this at the end of the test. What is the name of the hospital or the number of the place of residence where the patient is located.
FIRST AID
As a general rule, 100% O2 should be given for at least an hour before the patient is allowed to sit or stand. After this, the diver can be allowed to assume any comfortable position, but must be kept relatively still and on 100% O2.
TRANSPORT OF PATIENT WITH DCS
If this is not feasible, care should be taken not to overload the patient with fluids. Anti-epileptics and other drugs such as diazepam ("Valium") may be needed to control seizures (seizures) and confusional states.
DEFINITIVE TREATMENT OF DCS
Treatment in water with the diver's breathing air has been used in many parts of the world and water treatment tables are contained in some naval diving manuals. Although success has often been reported and delay in treatment can be avoided, this form of treatment has serious theoretical and practical problems that can lead to worsening of the diver's condition.
PREVENTION OF DCS
Repetitive recreational dives on the same day should have long surface intervals between dives, preferably 4 or more hours if possible, and a maximum of 3 dives per day. Driving over mountain ranges or hills by vehicle can expose divers to the same hazards as flying and should likewise be avoided for 24 hours.
DYSBARIC
OSTEONECROSIS
DIVERS BONE DISEASE, AVASCULAR NECROSIS OF BONE,
ASEPTIC BONE NECROSIS, BONE NECROSIS, BONE ROT,
CAISSON DISEASE OF BONE)
This can involve the joints as the underlying bone is destroyed and the joint surface collapses. As the condition progresses, severe osteoarthritis develops and the joint can eventually become frozen and incapacitated, due to pain.
NITROGEN NARCOSIS
COMPRESSED AIR INTOXICATION,
RAPTURE OF THE DEEP, INERT GAS NARCOSIS, NARCS)
CAUSES OF NITROGEN NARCOSIS
He activated his BCD's dump valve instead of the inflation valve, and drowned with minimal effort. Safe diving beyond 30 meters requires awareness of the ever-increasing risk of this condition and its impact on human performance and judgment.
HIGH PRESSURE NEUROLOGICAL
SYNDROME
HIGH PRESSURE NERVOUS SYNDROME, HPNS,
HELIUM TREMORS)
A tremor mainly affects the hands and arms and resembles shivering due to cold (which can also cause inhalation of helium). It is probably due to an excitation of part of the brain by the direct mechanical effect of pressure.
TREATMENT AND PREVENTION
HYPOXIA
ANOXIA)
CLASSIFICATION OF HYPOXIA
This is generally due to the heart failing to pump blood adequately to the tissues (eg from a heart attack or air embolism). This is generally due to insufficient amounts of circulating functional hemoglobin, usually from blood loss or carbon monoxide poisoning (see Chapter 23).
HYPOXIA IN BREATHHOLD DIVING
Poor circulation in the extremities in cold conditions can cause localized hypoxia in these areas without generalized hypoxia. The partial pressure of O2 in the lungs falls as they expand during ascent from a breath-hold dive.
HYPOXIA IN COMPRESSED GAS DIVING
Since the lung will still contain gas (mostly nitrogen), the diver will not be aware of the danger. The diver is often unaware that there is a problem and may even become overconfident.
OXYGEN TOXICITY
MECHANISM
If the patient has convulsions, he should be placed on his side to protect the airway from obstruction or aspiration of gastric contents. His airway should be protected and he should be managed according to the principles described in Chapter 42.
CONCLUSIONS
However, if it is essential to continue O2 therapy, a reduction in the partial pressure of O2 delivered will slow the development of toxicity. Short periods of 'air breathing' (or Heliox), 5 minutes every half hour, are often used by experienced clinicians to delay oxygen toxicity during O2 therapy.
CARBON DIOXIDE PROBLEMS
CARBON DIOXIDE INSUFFICIENCY (HYPOCAPNOEA OR HYPOCAPNIA)
A person who is hyperventilating due to anxiety is usually unaware of the altered breathing pattern, although it may be obvious to an observer. Symptoms include tingling or "pins and needles" (paresthesia) in the fingers, dizziness and lightheadedness, altered consciousness, or confusion.
CARBON DIOXIDE TOXICITY (HYPERCAPNOEA)
Since rebreathing is not possible with scuba equipment, CO2 toxicity is generally not a problem for scuba divers unless there is excessive resistance to breathing (regulatory resistance, increased gas density at depth) or reduced respiratory response of the diver to CO2 (possibly due to voluntary control or "skip breathing", adaptation, nitrogen narcosis or high oxygen levels). These depend on the initial velocity and the actual partial pressure of the inhaled CO2.
CARBON MONOXIDE TOXICITY
Severe brain damage is a frequent complication of significant CO toxicity due to prolonged hypoxia of the brain. The high partial pressure of O2, which occurs in a hyperbaric chamber, will dissolve enough O2 in the blood plasma to meet the body's needs without the participation of the hemoglobin system.
BREATHING GAS CONTAMINATION
PREPARATION OF COMPRESSED AIR
GAS PURITY STANDARDS
Since many of the divers can get their air supply from the same source, it is not uncommon for similar symptoms to spread among the diving group. A member of the diving club received the cylinders and reinstalled them in the bank.

DROWNING SYNDROMES
GENERAL
Damage to the walls of the alveoli also causes the capillaries to leak blood and protein into the lungs. The resulting inhalation of a bolus of water usually induces coughing and closure of the larynx, producing involuntary breathing followed by unconsciousness.


