List of Illustrations
The image on the right shows 3 aspects of the temporal window: 1) the middle; 2) behind; and 3) the front.
Critical Care Nursing
Monitoring and Treatment for Advanced Nursing Practice
The publisher and author make no representation or warranty as to the accuracy or completeness of the content of this work and specifically disclaim all warranties, including without limitation any implied warranty of fitness for a particular purpose. The fact that an organization or website is mentioned in this work as a citation and/or a possible source of further information does not mean that the author or publisher.
Contributors
Fitzpatrick, RN, MSN, CCRN Clinical Nurse Specialist for Surgical Intensive Care & Intermediate Care Units.
Introduction
In this text, chapter editors have attempted to examine the evidence base of monitoring and care delivery practices in critical care. Nursing practice in intensive care will always be based on human ethics and respect for individualized care.
Philosophy and treatment in US critical care units
US critical care units
The critical care team is generally quite complex and includes medical management increasingly supported by intensivists, residents, acute care nurses (ACNPs), clinical nurse specialists (CNSs), and other nursing staff. The Society of Critical Care Medicine (2013a) has identified rising costs of critical care medicine in the United States, with current projections of $81.7 billion (13.4% of hospital costs) to care for over 5 million patients per year in the country's intensive care units. .
Organization of critical care delivery
This is also supported by the Society of Critical Care Medicine (SCCM, 2013a). 2003) also made recommendations for postgraduate education and/or certification by critical care nurse managers within the leadership structure. Despite the fact that these guidelines were advanced more than 10 years ago, critical care practice remains varied across the country, in part due to the availability of key personnel, the organization of the state emergency system, system limitations due to population and area coverage and cost constraints.
Monitoring and surveillance in critical care
Revolutionary changes in patient outcomes have been achieved with the development of selected technology, including pulse oximetry, bispectral index for depth of anesthesia, and noninvasive measurement of cardiac output and stroke volume (Young and Griffiths, 2006). Particularly in the area of hemodynamic monitoring, studies have been inconclusive about the effectiveness of monitoring data in influencing patient outcomes (see Chapter 5).
Surveillance
More monitoring may not be the answer to improving the care of critically ill individuals, but individualized monitoring of the right parameters to guide therapy and improve patient outcomes is the goal of the ICU. Henneman, Gawlinski, and Giuliano (2012), in a review of practices recently studied in acute and critical care nursing, examined the use of checklists, interdisciplinary rounds, and other clinical decision support and monitoring systems important for surveillance and prevention of errors.
Nursing certification and
Overcoming barriers to integrating research at the bedside remains a challenge for all providers concerned with improving the quality of critical care (Leeman, Baernholdt, & Sandelowski, 2007; Penz & Bassendowski, 2006). In rapidly changing environments such as intensive care units, sustained change is difficult to maintain and improved systems are needed for better integration of evidence-based care.
US national critical care organizations
AACN promulgates nursing standards and is affiliated with a certification society dedicated to the certification of critical care nurses (AACN, 2013b). Current certifications available through the AACN certification program include specialty certifications in emergency/critical care nursing (adult, neonatal, or pediatric), obtaining certification as a registered nurse (CCRN).
Acute care advanced practice nursing
Significant differences included a focus on individual patients in the ACNP role (74 vs. 25.8% for CNS) and a relatively small amount of advanced practice nursing time spent on interventional skills in both APRN roles.
Clinical nurse specialists
Outcome assessment in complex settings has become an important part of advanced practice for CNSs and an integral part of graduate programs. In this document, expanding advanced practice competencies to the doctoral level includes an emphasis on expanded translational research, interprofessional collaboration, and many other competencies identified by the National Organization for the Advancement of Clinical Practice in Nursing (NACNS, 2009).
Acute care nurse practitioners
Many current ACNP programs require registered nurse licensure and clinical experience in critical care prior to entry onto the NP track, although a number of programs nationally allow second baccalaureate or higher degree entry and accelerated progress over several years to graduation. The richness of multiple students with a wide range of experiences adds value to the learning environment and promotes interdisciplinary communication, an important factor in safe practices in critical care, although this is an area that is still understudied.
Critical care and ACNP outcomes research
As critical care settings evolve, nurses and researchers continue to study changing health care systems. 2009) recommend a reconceptualization of core elements of NP education and practice, with an emphasis on stronger teaching and clinical work in health promotion and disease prevention. Advanced practice nurses, particularly those with advanced training and practice in critical care settings, can make significant contributions to these evolving models of care.
Evolution of families in the critical care unit
2011) credit Foote Hospital in Jackson, Michigan, as the first to implement an official hospital policy supporting family presence during resuscitation. A strong advocacy role is needed for APRNs in promoting policies that support family presence and other evidence-based interventions in critical care settings.
Progression and development of rapid response teams
Tarassenko, Hann, and Young (2006) investigated the use of integrated monitoring systems for early warning of patient deterioration and activation of RRTs. In one evaluation of a system designed to trigger team activation, an early warning system assigned five vital sign measures and data fusion to create a single status measure.
Activities performed by acute and critical care advanced practice nurses: The American Association of Critical Care Nurses Study.American Journal of Critical Care. Acute care nurse practitioners: creation and implementation of a model of care for a general hospital medical service.American Journal of Critical Care.
Vital measurements and
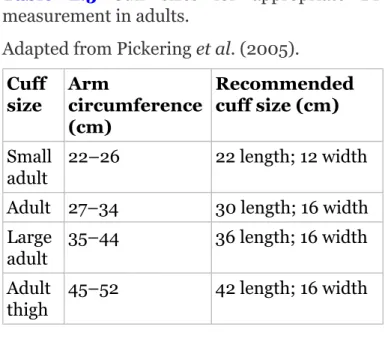
Monitoring basic vital signs
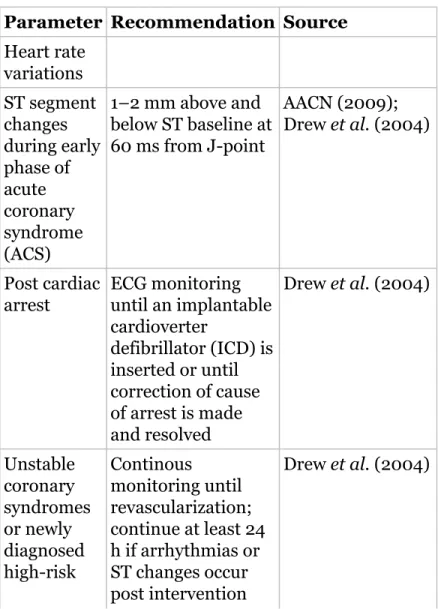
In general, the most accurate methods of temperature measurement include the use of a pulmonary artery thermistor, bladder probes, esophageal probes, and rectal probes (O'Grady et al., 2008). The use of EKG is ubiquitous in the intensive care unit and its use allows analysis and monitoring of heart rate, rhythm and waveform.

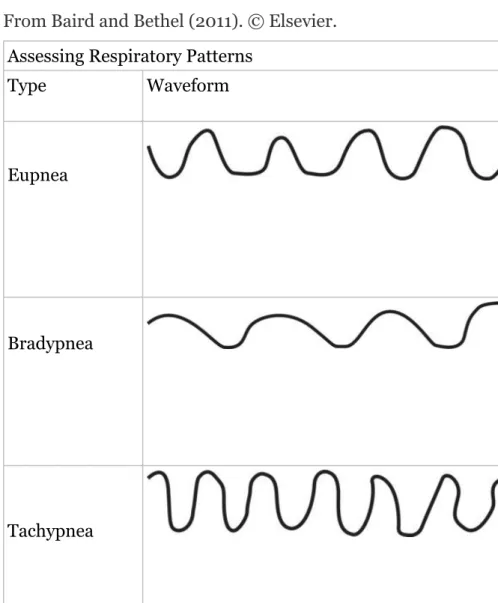
Respiratory monitoring
Ccapnography provides waveform displays of the entire respiratory cycle and continuous numerical displays of the partial ones. Monitoring and surveillance require an understanding of the relationship between the phases of the ventilation cycle and exhalation of CO2, the clinical condition of the patient and the ability to resolve alarm conditions.
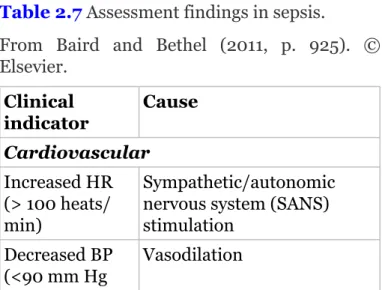
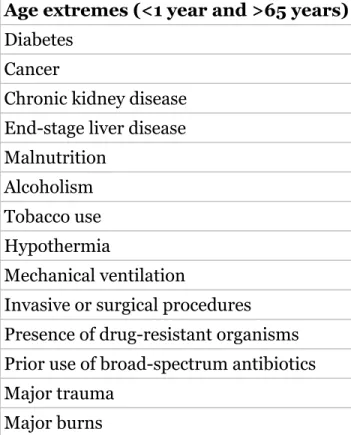
Shock conditions in critically ill adults
I recommendations for the treatment of cardiogenic shock include emergency revascularization (percutaneous intervention or coronary artery bypass grafting (CABG)) or fibrolytic therapy in patients unable to undergo interventional strategies and class II recommendations, including the use of intra-aortic balloon pump (IABP) (O 'Garaet) al., 2013). Central catheters in patients who have fever alone (no signs of SIRS or sepsis) should not be routinely removed (O'Grady et al., 2008).
Other infectious complications in critically ill adults
Direct fluorescent antibody staining for influenza A and B should be performed in patients with respiratory symptoms in the autumn and spring months (Mandelet et al., 2007). Diagnostic thoracentesis should be performed to obtain cultures in patients with pleural effusion associated with adjacent infiltrates to rule out aerobic or anaerobic empyema (Mandelet et al, 2007).
Monitoring during transport
Conclusion
Tissue hypoperfusion caused by sepsis. Critical Care Nursing Clinics of North America Who benefits most from mild therapeutic hypothermia in the era of coronary intervention. Guidelines for the evaluation of new-onset fever in critically ill adult patients: 2008 update from the American College of Critical Care Medicine and the Infectious Diseases Society of America.
Monitoring for respiratory dysfunction
Acid-base disturbances & anion gap
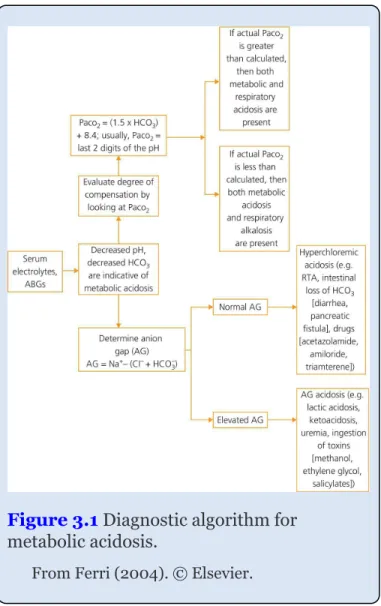
Metabolic acidosis
Clinical pearls
Reversal of sedatives or narcotics, as well as underlying pathology such as stroke, seizure, atelectasis, or drug overdose effects, should also be considered when devising a strategy to increase the patient's rate or depth of respiration to reverse acidosis. See Figure 3.3. for a more detailed diagnostic algorithm for respiratory acidosis. Determining whether or not a mixed disorder exists begins with the fact that for every 10 points there is CO2 or HCO3.

Oxygenation
Clinical Pearls
FiO 2 (P/F) ratio
Anything greater than 250 Torr is considered normal, and the shunt worsens as the P/F ratio decreases. P/F ratios less than 200 are associated with severe shunting, such as adult respiratory distress syndrome (ARDS).
Capnography
Monitoring of PetCO2 levels is considered a more objective method of assessing ventilation than respiratory depth or the subjective evaluation of respiratory depth (American Academy of Pediatrics, Committee on Drugs, 2002; American Society of Anesthesiologists Task Force on Sedation and Analgesia by non-anesthesia , 2002; Cacho et al., 2010; Greensmith and Aker, 1998; Lightdale et al., 2006; Sotoet al., 2004; Vargoet al., 2002). Waveform characteristics reveal information regarding ventilation, for example, hypopnea (small waveform), apnea (no waveform), or obstructive disease such as asthma ("shark fin" type pattern).

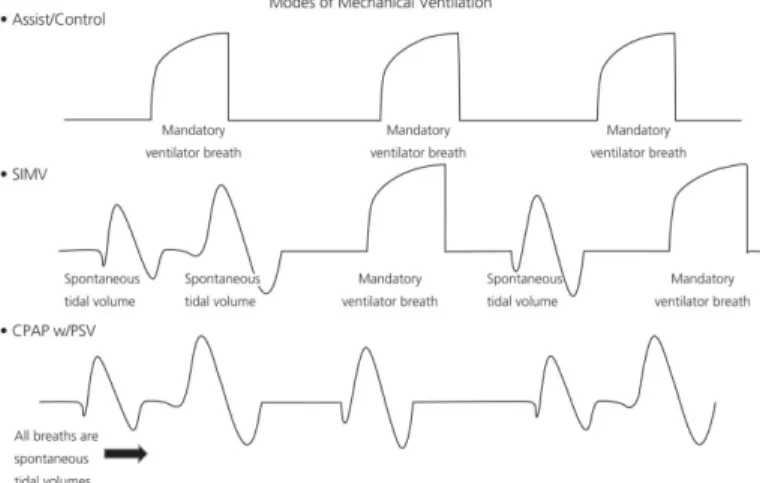
Modes of mechanical ventilation
This mode is associated with respiratory rates of 150–300 breaths per minute (i.e. Hertz, or .. cycles” per minute) and tidal volumes of approximately 50 ml (determined by the. This mode is often used in severe ARDS in order to avoid the risk of volutrauma and barotrauma that may be associated with AC or pressure control modes.
Monitoring for complications during mechanical ventilation
If bagging the patient is NOT difficult, the patient can be placed back on the ventilator. If it is difficult to bag the patient, the airway must be assessed for obstruction or otherwise.
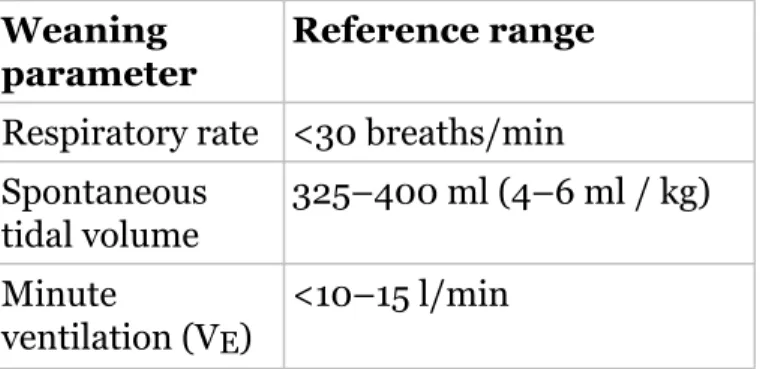
Weaning from mechanical ventilation
Auto-PEEP can be corrected by adding extrinsic (set) PEEP, decreasing tidal volumes, calming in some cases, and increasing the expiratory times (or shortening the inspiratory time) of the ventilator I/E ratio. Regardless of the specific weaning strategy used, the ultimate goal is to wean to extubation as soon as the patient can safely tolerate it.
Sleep-disordered breathing in the critical care unit
OSA is characterized by excess soft tissue in the upper airway, restricting airflow and causing obstruction, which is associated with postoperative complications, increased intensive care unit admissions, onset of delirium, and increased length of stay in the hospital (Chung et al., 2008). . Although difficult to use in the intensive care setting, polysomnographic studies have shown significant disruptions of sleep architecture in ICU patients (Cabello et al., 2008; Parthasarathy and Tobin, 2002).