Department of Obstetrics and Gynecology University of Utah Medical Center Salt Lake City, UT, USA. Department of Obstetrics and Gynecology Division of Maternal - Fetal Medicine University of Texas Medical Branch Galveston, TX, USA.
Flint Porter
Department of Obstetrics and Gynecology, University of Iowa School of Medicine Iowa City, IA, USA. 2 Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, Lehigh Valley Health Network, Allentown, PA, USA.
Introduction
Hospital admissions for preterm labor were twice as common for non-delivery hospital admissions (21.21%) than for delivery-related hospital admissions (10.28%). Hospital admissions for infection-related conditions were twice as common during periods without labor (11.65%) than during labor (5.75%).
Maternal m ortality
However, the mean hospital LOS for liver disease occurring in non-delivery hospitalizations was over 31 days, compared to a mean LOS of 3 days if the liver disease was related to delivery. The top 10 conditions associated with hospital admissions, separately for childbirth-related and non-childbirth-related events, are shown in Figure 1.1.
Pregnancy - r elated h ospitalizations
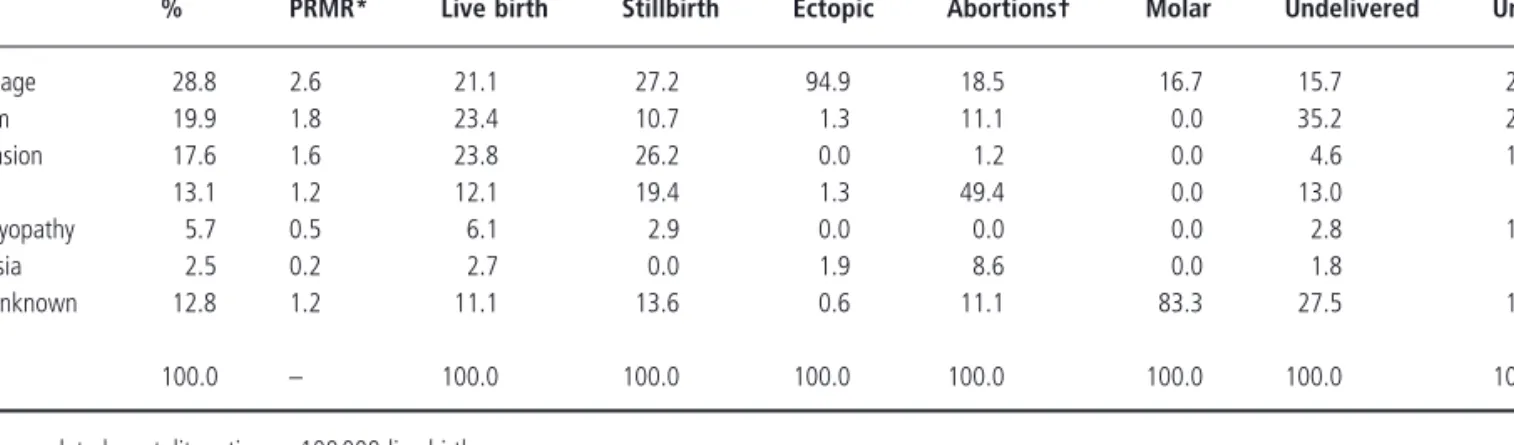
Coagulation-related disorders required 14.9 days of hospitalization if unrelated to labor, compared with a mean LOS of 4.9 days if the condition was labor-related. Among stillbirths (27.2%) and ectopic (94.9%) pregnancies, hemorrhage was the leading cause of death, while infections (49.4%) were the leading cause of abortion-related maternal death.

Perinatal m ortality
Most of the studies were small and just a few deaths could significantly affect the rates. They probably reflect part of the “learning curve” of critical care obstetrics, as well as differences in available technology [52].
Illnesses r esponsible for o bstetric i ntensive c are u nit a dmissions
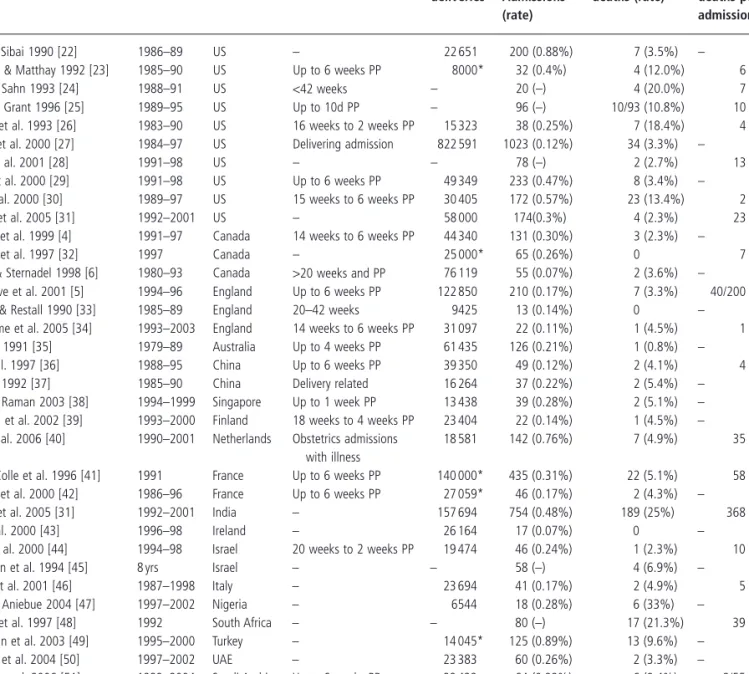
Reported maternal mortality for critically ill obstetric patients admitted to an ICU is approximately 8.4% (Table 1.4. These earlier studies represent the early stages of development of care mechanisms for critically ill obstetric patients.
Pregnancy - r elated i ntensive c are u nit a dmissions
This study found an almost 30% lower admission rate to ICUs for obstetric patients from community hospitals compared to large teaching hospitals. Regardless, the mortality rate from these ICU admissions is several orders of magnitude higher than the general US population maternal mortality rate of 11.5 per 100,000 live births.
Causes of m ortality in o bstetric i ntensive c are u nit a dmissions
Summary
Perinatal l oss 101th obstetric intensive care unit admissions
We also appreciate the efficient and excellent assistance of Susan Fosbre during the preparation of this manuscript and thank Laura Smulian for critical reading of the chapter.
Acknowledgments
Usefulness of Acute Physiology, Aging and Chronic Health Evaluation (APACHE III) score in maternal admissions in the intensive care unit. Risk factors for obstetric admissions in the intensive care unit in a tertiary hospital: a case-control study.
Relevance
As a result of these complexities, the critical care team has expanded to include many disciplines with varying levels of organizational leadership. An extension of these critical care models has been applied to obstetric medicine, which has a unique population of critically ill women.
Patient population
The organization of the intensive care unit has evolved from the time of Florence Nightingale, who wrote about post-operative areas near operating rooms with bedside attendants, to the technologically and medically advanced intensive care units we use today [1]. Pregnancy alters maternal physiology in relation to many organ systems with notable changes relating to intensive care in the hematological, cardiopulmonary, renal, endocrine and digestive systems.
Members of the team
Collaboration of the intensivist with the attending of record (admitting physician) maximizes the level of care delivered while maintaining continuity of care for the patient. The obstetrician specialist will play a key role in the management of the critically ill birth.
Unit design: a virtual space
The familiarity of the patient with the attending physician strengthens trust in medical management and helps to promote a positive psychosocial environment, which is important in treatment. The Virtual Maternity Unit is uniquely positioned to meet the specific medical needs of the critically ill maternity patient, eliminating the need to maintain a separate unit within the hospital.
Conclusion
The innate need for professional collaboration, communication and teamwork in the intensive care environment is enhanced. Case examples are presented to illustrate the application of critical care concepts in clinical nursing practice.
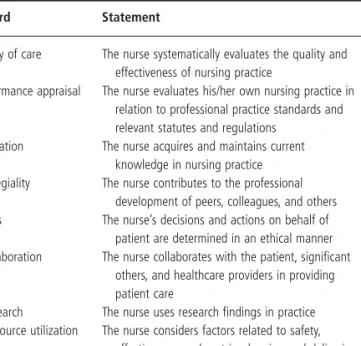
Standards of n ursing c are: f ramework for c ritical c are o bstetric n ursing
2 Women's Services, Labor & Delivery and High Risk Perinatal Unit, Inova Fairfax Hospital Women's Center, Falls Church, Virginia and Columbia University; New - York Presbyterian Hospital, Department of Obstetrics and Gynaecology, Department of Maternal - Fetal Medicine and Consultant, Critical Care Obstetrics, New York, USA. The essence of intensive care nursing lies neither in special environments nor in special equipment, but in the decision-making process of the nurse and the willingness to act on those decisions (Tables 3.1 and 3.2.
Critical c are t echnology: c ritical c oncepts and a pplication to c linical p ractice
Nursing standards are presented, which represent the framework of the entire professional practice of nursing. Finally, strategies for the adequate preparation of nurses to provide quality care to critically ill pregnant women are described.
Invasive h emodynamic m onitoring: c oncepts for i ntrapartum n ursing p ractice
In other words, physicians expect nurses to use the nursing process as a framework for patient care. The same concept applies to the practice of critical care, especially when technological tools such as invasive hemodynamic monitoring or mechanical ventilation are used in the care of a unique patient population.
Central v enous a ccess
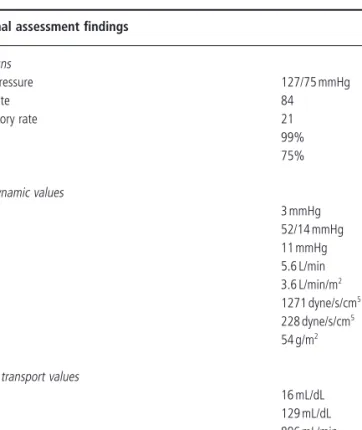
Based on these data, iced injectate is recommended if cardiac output is expected to be less than 3.5 L/min or greater than 8.0 L/min. In addition, formulas used to calculate essential oxygen transport parameters also include cardiac output.
Heparin fl ush
Thus, careful assessment of the presence of uterine contractions and appropriate timing of cardiac output measurements are crucial. Cardiac output factors in the formula for the calculation of significant hemodynamic parameters, including systemic vascular resistance, pulmonary vascular resistance and left ventricular stroke index.
Cardiac o utput e valuation
Assessment by the nurse of the pulmonary artery waveform revealed the presence of large V waves. Interventions to optimize cardiac output have focused on improving left ventricular contractility and correcting the patient's high left preload.

Mechanical v entilation d uring p regnancy
For these reasons, it is especially important that the nurse regularly assess the hemodynamic and oxygen transport status of the obstetric patient requiring mechanical ventilation. Ensure the condition of the pregnant stable to return to labor and delivery to stay in the room.
The result was a conflict between the duties of the intensive care nurse and the rights of the patient and family members. This facilitated involvement of the patient's husband and other family members in the overall plan of care.

Variables such as maternal age, multiple pregnancy, ethnicity and genetic factors influence the mother's ability to adapt to the demands of pregnancy. This chapter discusses in detail the normal physiological adaptations that occur in each of the major maternal organ systems.
Cardiovascular s ystem
Linhard [37] was the first to report a 50% increase in cardiac output during pregnancy using the indirect Fick method. A further increase in cardiac output was evident during contractions due to increases in both heart rate and stroke volume.
![Figure 4.1 Blood volume changes during pregnancy. (Reproduced with permission McLennon and Thouin [1] .)](https://thumb-ap.123doks.com/thumbv2/123dok/10531203.0/43.1039.512.919.151.370/figure-blood-changes-pregnancy-reproduced-permission-mclennon-thouin.webp)
Respiratory s ystem
In later pregnancy, the enlargement of the uterus leads to changes in the shape of the breast. Loss of glucose in the urine (glycosuria) is a normal finding during pregnancy, due to increased glomerular fi ltration and decreased distal tubular reabsorption [161].

Gastrointestinal s ystem
Filtered sodium load is significantly increased due to increased GFR and the action of progesterone as a competitive inhibitor of aldosterone. The increase in tubular sodium reabsorption is likely due to increased circulating levels of aldosterone and deoxycorticosterone [164].
Genitourinary s ystem
Indeed, urinary protein loss of up to 260 mg/day can be considered normal during pregnancy [163]. Despite this increased filtered sodium load, increased tubular reabsorption of sodium results in a net retention of up to 1 g of sodium per day.
Hematologic s ystem
In addition, pregnancy is associated with an increase in bile cholesterol concentration and a decrease in the concentration of selected bile acids (especially chenodeoxycholic acid), both of which contribute to the increased lithogenicity of bile. Pregnancy is associated with changes in the coagulation and fibrinolytic cascades that favor thrombus formation.
Endocrine s ystem
The observed decrease in fibrinolytic activity during pregnancy is likely due to the marked increase in the plasminogen activator inhibitors, PAI-I and PAI-2 [187]. However, these same physiological changes also place the mother at increased risk for thromboembolic events, both during pregnancy and postpartum.
Immune s ystem
Circulatory adaptation to pregnancy – serial studies of hemodynamics, blood volume, renin and aldosterone in the baboon ( Papio hamadryas. Appendicitis in pregnancy with changes in position and axis of the normal appendix in pregnancy.
Renee A. Bobrowski
Essential physiology
Oxygen supply depends on oxygenation of blood in the lungs, oxygen carrying capacity of the blood and heart volume. The level of oxygen supply at which oxygen consumption begins to decrease has been termed "critical DO 2 " [23].
Blood gas analysis
These parameters can be measured directly by drawing a blood sample from the distal port of the pulmonary artery catheter. Conditions that cause the curve to shift to the left cause the venous oxygen saturation to be normal or high even when the mixed venous oxygen content is low.
Blood gas interpretation
The shape of the oxy-hemoglobin dissociation curve allows P a O 2 to decrease faster than oxygen saturation until P a O 2 is approximately 60 mmHg. Total serum CO 2 (tCO 2 ) is measured by serum electrolytes and is the sum of the different forms of CO 2 in the serum.
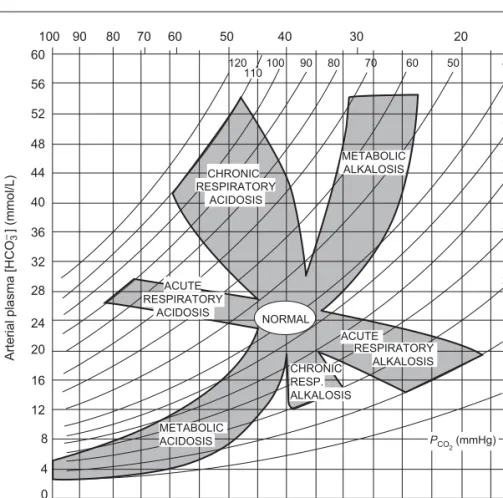
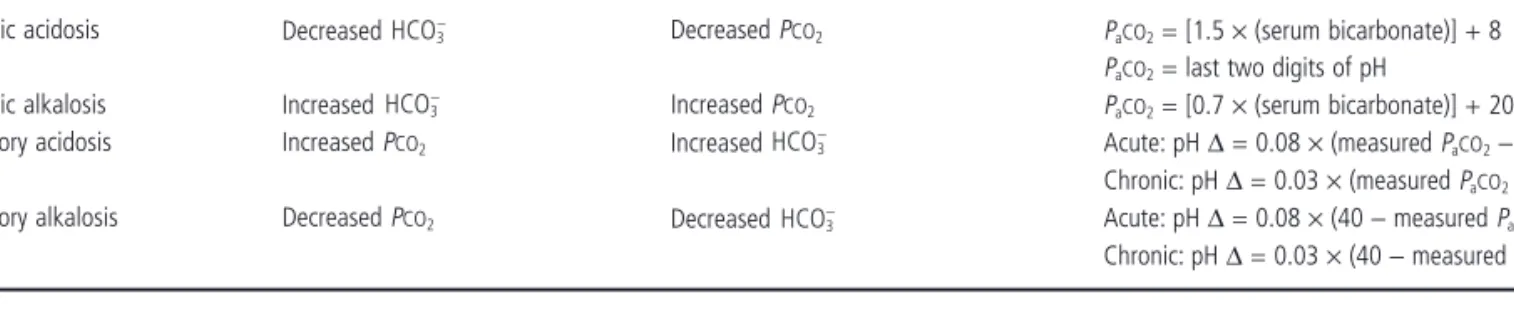
Disorders of acid – base balance
Once a metabolic acidosis is detected, serum electrolytes should be obtained to calculate the anion gap. Although an increased anion gap is traditionally associated with metabolic acidosis, it can also occur in the presence of severe metabolic alkalosis.

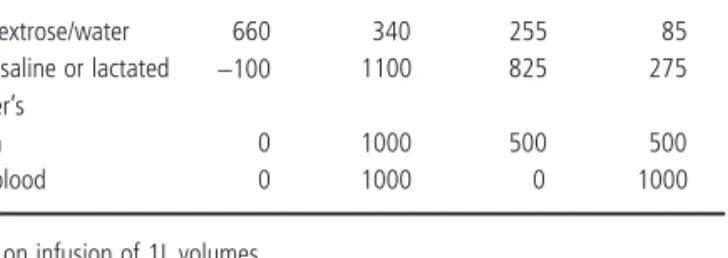
In healthy non-pregnant adults, approx. 25% of the infused volume in the intravascular space after 1 hour. However, in the critically ill or injured patient, only 20% or less of the infusion remains in the circulation after 1 – 2 hours [35,36].
Fluid r esuscitation
The use of albumin in patients with volume depletion, regardless of cause, is not without controversy. They increase COP, resulting in movement of fluid from the interstitial to the intravascular compartment.
Electrolyte d isorders
In acute, symptomatic, hypernatraemia, sodium can be reduced by 6 – 8 mEq/L in the first 4 hours. The mechanism of the increase in glomerular fi ltration rate in twelve-day pregnant rats.
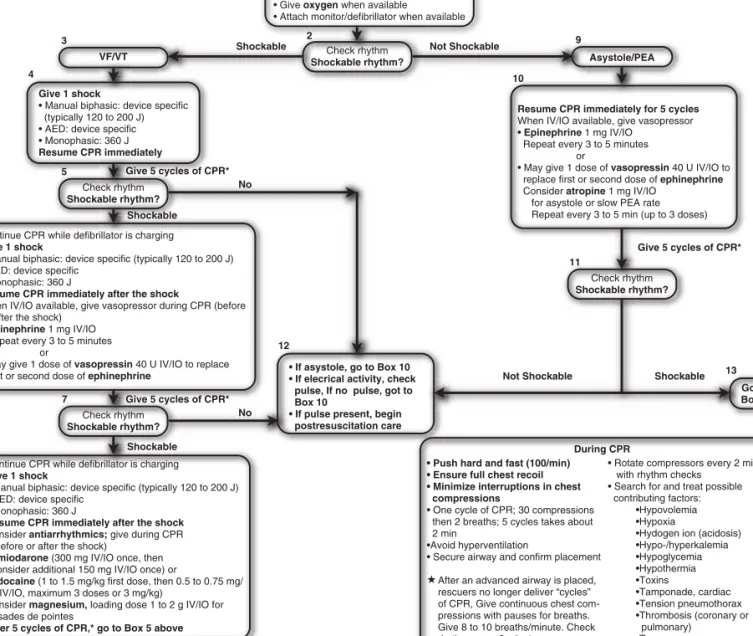
Current c ardiac c are r ecommendations
The overall outcome, especially full neurological recovery, is improved by early initiation of CPR and defibrillation. As mentioned in the general guidelines above, before an advanced airway is in place, rescuers should perform 5 cycles of post-shock CPR before the next rhythm check.
![Table 7.1 Summary of CPR ABCD s (modifi ed from “ Summary of BLS ABCD maneuvers for infants, children and adults ” ) [68]](https://thumb-ap.123doks.com/thumbv2/123dok/10531203.0/106.1039.119.624.170.465/table-summary-modifi-summary-maneuvers-infants-children-adults.webp)
One rescuer delivers 8 – 10 breaths per minute (1 every 6 – 8 seconds), while the other rescuer applies continuous compressions. The provider's general BLS algorithm is shown in Figure 7.1 and the ACLS algorithm without pulse in Figure 7.2.
Pregnancy - s pecifi c c onditions a ssociated with SCA
In the first half of pregnancy, airway obstruction can be eliminated with the Heimlich maneuver or abdominal thrusts. The unconscious victim is placed on his back, the heel of one hand rests against the victim's abdomen, in the midline slightly above the navel, but below the tip of the xiphoid.
The e ffect of p regnancy on c ardiopulmonary r esuscitation
Therefore, early in the resuscitation, resources should be mobilized to get blood products to replenish the vascular tree and deal with ongoing bleeding. But overzealous fluid resuscitation, especially with crystalloid fluids, before control of bleeding and in the early stages of.
Compensated respiratory alkalosis increases - Change in target values and increased ventilation required, avoid bicarb in resuscitation. Adenosine, lidocaine, procainamide and beta-blockers, which are also used in the treatment of tachyarrhythmias, appear to be safe in pregnancy [46].
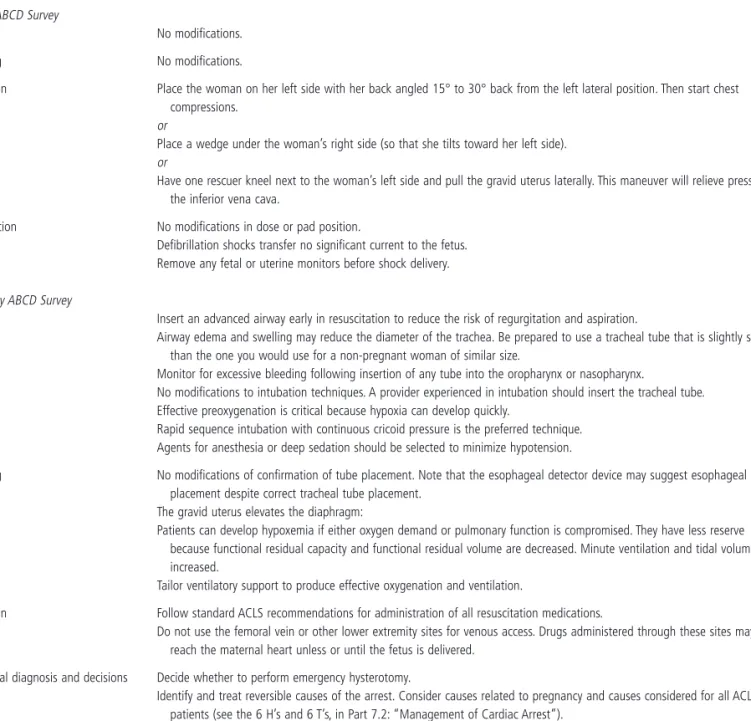
Modifi cations of b asic l ife s upport and a dvanced c ardiac l ife s upport in p regnancy
Its obvious disadvantage of the wedge is that it must be moved when defibrillation becomes necessary. Therefore, with prompt correction of the mother's metabolic acidosis, her respiratory compensation will cease as her PCO 2 normalizes to the nonpregnant state.
Thrombolytic t herapy
Perimortem c esarean d elivery
It should be emphasized that there are no data prospectively documenting the actual benefits of postmortem caesarean section for the mother. There are many anecdotal examples of improved maternal response to resuscitation after postmortem caesarean section.
The n eurologically i mpaired p atient f ollowing r esuscitation
In the context of a postmortem caesarean section performed on a fetus that is likely to be saved, staff must be well versed in neonatal resuscitation techniques, as these infants are likely to suffer from respiratory and circulatory depression at birth. Women with chronic conditions are less likely to have a normal surviving infant by perimortem caesarean section compared with previously healthy women who have suffered cardiac arrest after an acute obstetric event.
Case p resentation
Pulseless electrical activity (PEA) identified earlier during resuscitation supported this possibility. During the first 4 hours of resuscitation, she received a total of 10 units of packed red blood cells and 2 units of FFP.
Elements of b irth d epression
In a newborn without a connection to the placenta after the umbilical cord is attached, maintaining fetal circulation diverts blood away from the lungs, the only available organ for gas exchange. Thus, blood flow to the heart and brain vessels increases at the expense of "non-vital" organs.

The first two must be done before the expected delivery: (i) Raise the temperature. There is good evidence that overexpansion of the lung (volutrauma) is more concerning than trauma caused by high pressure (barotrauma) [18].

Special p roblems d uring r esuscitation
The urine output of any child experiencing a depressive episode should be carefully monitored. During the choking process, intestinal ischemia may occur due to vasoconstriction of the mesenteric blood vessels.
Immediate c are a fter e stablishing a dequate v entilation and c irculation
The child with a pneumothorax may present with uneven breath sounds and distant heart sounds, or the heart sounds may be shifted from the normal position on the left side of the chest. Careful attention must be paid to maintaining the pattern, which further impairs airway ventilation and oxygenation.

Screening for c ongenital a nomalies
Influences of arterial oxygen tension and pH on cardiac function in newborn lambs. The role of tidal volume, FRC and end-inspiratory volume in the development of pulmonary edema after mechanical ventilation.
Respiratory f ailure
The alveolar – arterial oxygen tension gradient (P (A – a) O 2 ) is a sensitive measure of impairment of oxygen exchange from lung to blood [3]. Under these circumstances, the alveolar–arterial oxygen tension gradient is less than 50 torr when F in O 2 is 1.0 (or less than 30 torr on room air).
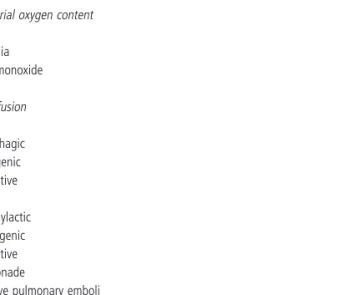
Oxygen d elivery and c onsumption
It should be borne in mind that the amount of oxygen available to the tissues is also affected by the affinity of the hemoglobin molecule for oxygen. Oxygen delivery may be impaired by conditions affecting cardiac output (flow), arterial oxygen content, or both (Table 9.2.
Assessing o xygenation
Continuous positive airway pressure (CPAP) is the most commonly used method of non-invasive positive pressure ventilatory support. Unlike CPAP, which provides no ventilatory support and delivers sustained positive pressure, non-invasive positive pressure ventilation delivers intermittent positive airway pressure through the upper airway and actively supports ventilation [25].
Impairment of o xygenation
Noninvasive approaches have been most effective in managing episodes of acute respiratory failure where rapid improvement is expected, such as during cardiogenic technique episodes, and are therefore useful as a continuous monitor of. These parameters can be measured directly by drawing a blood sample from the distal port of the pulmonary artery catheter when the catheter tip is well positioned for a wedge pressure reading and the balloon is not inflated (distal pulmonary artery branches).
Mechanical v entilatory s upport in p regnancy
Therefore, 100% oxygen should be administered either by mask or by ambubag when the patient requires intubation. Overenthusiastic hyperventilation should be avoided because the associated respiratory alkalosis may actually decrease uterine blood flow.
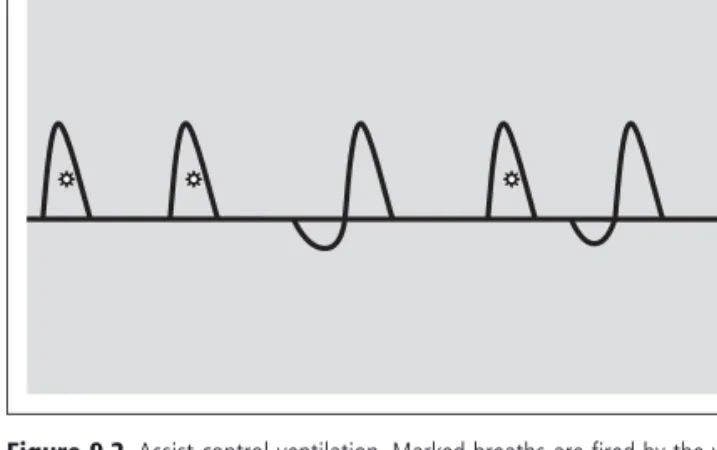
Ventilator m odes
Alternatively, the use of "in rapid sequences", induction of general anesthesia and the Sellick maneuver (cricoid pressure) can be used to prevent passive reflux of gastric contents into the pharynx [32].
Intubation
Each time the patient activates the ventilator, she will receive a predetermined amount of pressure support. Here, the tidal volume will be determined by the patient's effort and the predetermined amount of pressure support adjusted on the ventilator by the operator.
Alternative m aneuvers d uring m echanical v entilation
Since NO forms methemoglobin after interaction with oxyhemoglobin, it should not be administered to patients with methemoglobin reductase deficiency [77]. NO should not be used in patients with severe left ventricular failure as the predominantly pulmonary arterial vasodilation (as opposed to pulmonary venodilation) may lead to pulmonary edema [78].
Lung p rotective s trategy m echanical v entilation
As a surrogate of the latter, the plateau pressure can easily be measured at the bedside. Plateau pressure reflects the peak alveolar pressure and has been shown to be a better marker of the risk of VILI than peak airway pressure.
Special c onsiderations d uring m echanical v entilation
We recommend the use of lung protective mechanical ventilation in the critically ill pregnant woman with ALI/ARDS as an extrapolation from the general ARDS population. When feasible, early enteral feeding (within 48 hours of initiation of mechanical ventilation) should be initiated in the critically ill patient.
Pain c ontrol, s edation, and p aralysis
We do not recommend prolonged infusions of midazolam in patients with renal impairment due to the accumulation of the active metabolite 1 - hydroxylmethylmidazolam [141]. Patients in the study group had improved oxygenation; however, there was no difference in the duration of mechanical ventilation.
Acute a sthma
The bispectral index can be used as a guide for sedation in critically ill patients receiving pharmacologic paralysis. In the latter trial, five of eight patients with obstructive pulmonary disease demonstrated the occurrence of "paradoxical responses" to external PEEP.
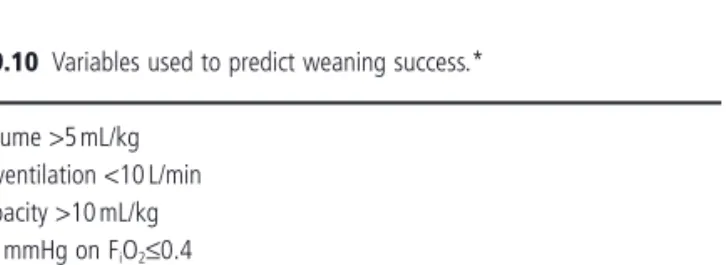
Weaning from m echanical v entilation
Mechanical ventilation in sepsis - induced acute lung injury acute respiratory distress syndrome: An evidence-based review. What is the optimal duration of ventilation in the prone position in acute lung injury and acute respiratory distress syndrome.
Catheter t ype
Ideally, reservoirs for implantable catheters should be placed in a safe, flat, non-mobile area, preferably over a rib. After the catheter has been inserted and secured, a dressing should be placed over the site.
Due to this slow release, the preparation must remain in contact with the skin for at least 2 minutes [20 – 22]. Shaving at catheter insertion sites is not recommended as it abrades the skin and promotes bacterial colonization.
Preparing for c atheter i nsertion
By pulling apart the sheath handles, the sheath is then simultaneously peeled in half along its long axis and removed while carefully holding the catheter in place. The heparinized saline is infused through the pressure bag at a rate of approximately 2 – 5 mL/h to prevent the catheter from clotting.
Special t echniques for c atheter i nsertion
The sharp needle is then removed and the polyurethane catheter is inserted over the wire into the vein. After the tract is dilated, the dilator-sheath assembly is pulled over the wire into the selected vein, and the wire and dilator are removed.
In general, the smaller the diameter of the catheter in relation to the vessel size, the lower the incidence of thrombosis. A triangular area created by two heads of the SCM and the clavicle is then identified (Figure 10.3.

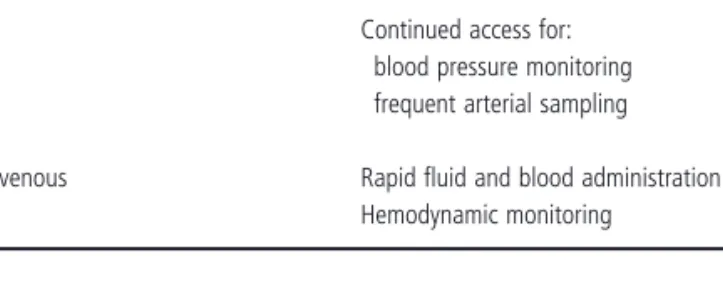
Specifi c v enous a ccess s ites
The EJV joins the SCV at a sharp angle below the area of the clavicle [46]. In the posterior approach, the needle is advanced along the lower abdomen of the SCM and aimed at the suprasternal notch.

Specifi c a rterial a ccess s ites
Often both vessel walls are perforated and the catheter will lie posterior to the vessel. Using an arm board prevents twisting of the elbow and twisting of the catheter.

Catheter - r elated i nfection
However, in its latest recommendation, the CDC suggests limiting the use of antimicrobial/antiseptic impregnated catheters to areas of the hospital with unacceptably high CRBSI rates (despite implantation of appropriate measures) or to patients who are expected to have the catheter in place for more than 5 days. Correct and safe use of central catheters requires knowledge of indication, careful sterile technique,
Acknowledgement
Contamination of central venous catheters: The skin insertion swab is a major source of contamination. Prospective randomized study of two antiseptic solutions for the prevention of central venous catheterization of arterial colonization and infection.
David A. Sacks
Blood d onation, c ollection, and s torage
By centrifuging the filtered product, erythrocytes with a reduced number of leukocytes and plasma can be retained. Cells can be retrieved from stored blood at any time during the shelf life of the unit.
![Table 11.1 Selected requirements for allogeneic blood donors, per AABB standards [1]](https://thumb-ap.123doks.com/thumbv2/123dok/10531203.0/178.1039.128.845.158.944/table-selected-requirements-allogeneic-blood-donors-aabb-standards.webp)
Whole b lood and c omponents: d escription and i ndications
The first step in receiving compatible blood is determining the ABO and Rh type of the recipient's red cells. Reagent red cells are certified to contain all clinically relevant antigens.
Transfusion p ractices
Hemoglobin concentration is the product of hematocrit and mean hemoglobin content (MCHC). We must not forget that only a third of the crystalloid remains in the intravascular space.
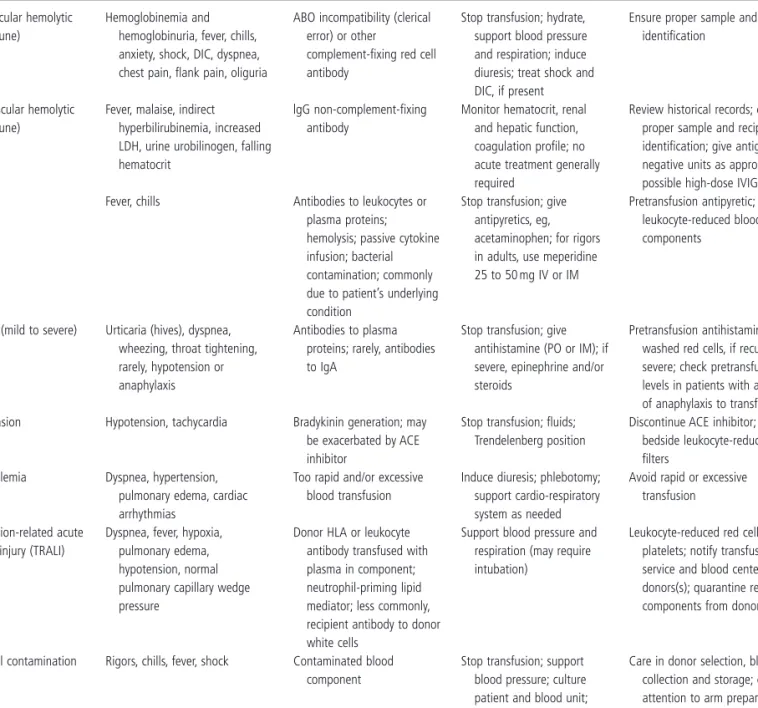
Transfusion r eactions
Obtain blood/urine for transfusion reaction workup
In an acute extravascular hemolytic transfusion reaction (AEHTR), the antibody against the transfused incompatible cells does not fix complement, but does bind to the corresponding antigens of the transfused cells. A febrile non-hemolytic transfusion reaction (FNHTR) is defined as a temperature increase of 1°C or more within 2 hours after a blood transfusion for which no cause can be found [4,5].
Send report of reaction, samples, blood bag, and administration j set to blood bank
Because of the marked reduction in complement and cytokine activation [60], hypotension, DIC, hemoglobinuria, and renal failure that characterize an AHTR are rarely found with an AEHTR [5]. Fever rarely accompanies an allergic reaction, a feature that distinguishes it from a hemolytic transfusion reaction and from sepsis.
Consult with blood bank physician before further transfusion
Managing the rare patient who has had a severe allergic reaction but requires transfusion of plasma products (eg, the patient with thrombotic thrombocytopenic purpura) is a serious challenge. The treatment of TRALI requires discontinuation of the transfusion and support with oxygen and ventilation.
Transfusion - transmitted d isease
Of interest is the observation that both donor platelets, which do not have the antigen, and recipient platelets, which do contain the antigen, are destroyed in PTP. The transfusion of antigen-matched platelets does not seem practical, as matching donors are unlikely to be found, and also because both donor and recipient platelets are destroyed in PTP [5,72] .
Concluding c omments
Hematocrit cutoffs for assessing the need for red blood cell transfusion in patients with hypovolemic anemia. The length of pregnancy and the unique nature of the fetomaternal unit require the mother to make significant adjustments to ensure optimal outcomes for the fetus and mother (Table 12.1.
Normal n utrition in p regnancy
In addition, the placenta has well-developed mechanisms to control the passage of substrate to the fetus (Table 12.2. The effectiveness of the passage of any substance through the syncytiotrophoblast depends on a number of factors listed in Table 12.3.
Malnutrition in p regnancy
Nature of transport mechanism (passive vs active transport) Specific binding or carrier proteins in maternal or fetal circulation Placental metabolism of the substance. 1 Normal values obtained in non-pregnant women cannot be readily extrapolated to the hemodilute pregnant patient.
Routes for n utritional s upport
4 Although nitrogen balance and creatinine clearance can be effective methods of assessing protein status in the nonpregnant patient, both are markedly altered by the increased glomerular filtration rate during normal pregnancy.
Nutritional a ssessment d uring p regnancy
The recommended dietary intake is an additional 300 kcal/day in singleton or 500 kcal/day in twin pregnancies in the second and third trimesters. CVN is generally well tolerated by the pregnant woman and is convenient for the medical staff.
Calculation of n utritional r equirements
A nutritionally deficient pregnant woman may require more than 300 kcal/day for supplementation in a singleton pregnancy. Monitoring the effectiveness of maternal nutritional support is accomplished by plotting maternal weight gain against standard charts and serial sonographic estimates of fetal growth.
Fat e mulsions
Fluids and e lectrolytes
Amino a cids
Carbohydrates
Small-for-gestational-age birth: maternal predictors and comparison with risk factors for spontaneous preterm birth in the same cohort.
Monitoring and c omplications
Effect of protein deficiency in pigs during all or part of gestation on birth weight, postnatal growth rate and nucleic acid content in brain and muscle of offspring. 1 Department of Obstetrics and Gynecology, Uniformed Services University of the Health Sciences, Old Madigan Army Medical Center, Tacoma, WA, USA.
The need for dialytic support during pregnancy, although uncommon, is by no means a rarity and may be seen more frequently with improvements in the care of renal failure patients.
Overview of d ialysis
![Table 1.5 Complications primarily responsible for admission to the intensive care unit for obstetric patients: data summarized from 26 published studies [4 – 6,22 – 26,28,31,32,35 – 37,39,40,42 – 51]](https://thumb-ap.123doks.com/thumbv2/123dok/10531203.0/20.1039.122.880.190.520/complications-primarily-responsible-admission-intensive-obstetric-summarized-published.webp)
![Table 1.6 Identifi ed primary causes of mortality in obstetric admissions to ICU s reported in 26 studies [4 – 6,22 – 26,28,31,32,35 – 37,39,40,42 – 51]](https://thumb-ap.123doks.com/thumbv2/123dok/10531203.0/21.1039.159.514.190.970/table-identifi-primary-mortality-obstetric-admissions-reported-studies.webp)