1 Rationale for orthodontic treatment at an early age 2 Dentition development and dental occlusion 3 Examination, early detection and treatment planning. At the beginning of the 20th century, there was optimism about the influence of orthopedic force on skeletal growth.
General objectives
With a thorough understanding of the biological facts and the availability of new intraoral and extraoral devices and techniques, clinicians can gain a better understanding of when and how to apply early intervention to prevent the problems and control future adverse effects on the patient's growth pattern. The concept of orthodontic treatment in early age includes all interventions and treatments that can be performed during the primary or mixed dentition, with the aim of eliminating or minimizing dentoalveolar and skeletal disharmonies that can interfere with the normal growth and development of occlusion, function, aesthetics, and children's psychological well-being.
General strategy
Preventive orthodontic treatment includes treatments that prevent the development of a malocclusion before it occurs, such as space maintenance or habit control. Early age orthodontic treatment may include preventive, interceptive or corrective treatment as well as combinations of the three types applied during the primary or mixed dentition period, before the full development of the malocclusion.
One-phase versus two-phase orthodontic treatment
This can be time-consuming and pose serious risks to the health of the teeth and surrounding tissue structures. The most important stage of the dental occlusion is the transitional dentition; consequently, most dentoskeletal disorders begin and develop during the primary or mixed dentition.
Mechanisms affecting occlusal development
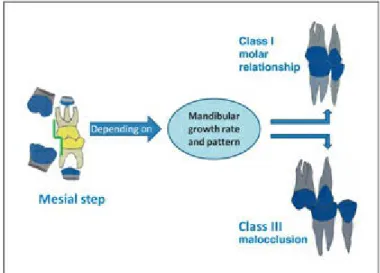
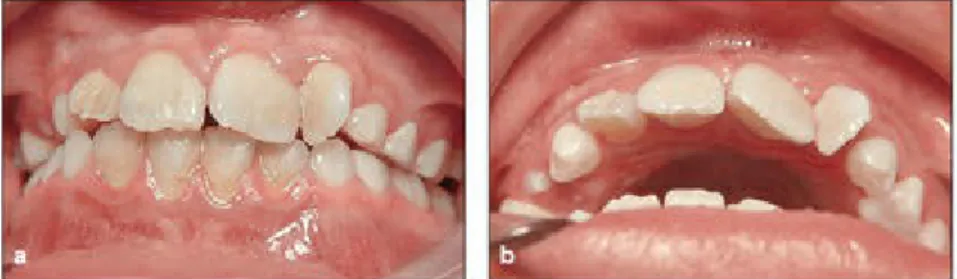
During this long process, craniofacial growth also interacts with the development of the dentition. Collapsed maxillary arch, occurring during the primary or mixed dentition, which can prevent normal sagittal and transverse growth and displacement of the maxillary arch (Fig 1-1).

Current interest in early-age treatment
Rationale
The challenge is to select the right type of intervention at the right time for each individual case. To apply the right treatment at the right time, it is necessary to first look at the principles and strategy of early orthodontic intervention (for more details, see Chapter 11).
Goals of early orthodontic treatment
If the answer to any of these questions is "yes," then it's time to start early intervention.
Phases of early orthodontic treatment
Some patients benefit from a single treatment phase, usually beginning around the late mixed dentition and ending during the permanent dentition. One-phase treatment is one phase of comprehensive treatment to correct abnormalities in deciduous, mixed or permanent dentition.
Monitoring the dentition
Another example of a two-phase treatment is early intervention and control of abnormal habits, which can be initiated during primary or mixed dentition and followed by an intermediate phase of monitoring during transitional dentition, until eruption of the permanent dentition for phase 2- therapy. Many other abnormalities, such as hypodontia and hyperdontia, anterior and posterior crossbite, eruption problems (impaction and transposition ankylosis), abnormal oral habits and abnormal frenum attachment, require early intervention as phase 1 treatment during primary or mixed dentition and a second treatment . phase during the permanent dentition.
Clinical evidence
In a review of the literature, Kluemper et al20 similarly argued that both the one-phase and two-phase approaches are effective in correcting Class II malocclusion. Whether the type of class II malocclusion (dental, skeletal, or combined) was determined for all subjects.
Misconceptions about early treatment
The types of treatments and services that can be provided to young children during the dental and skeletal growth stages are enormous. Many dental and skeletal anomalies can be prevented or intercepted during the primary or mixed dentition.
Benefits to patients
Younger children seem to have less resistance to moving bones and teeth and complain less. The total cost of early orthodontic treatment is lower than the comprehensive treatment of permanent teeth, because the therapy is less extensive, there is less time spent in the chair per visit and the appointment intervals are longer.
Benefits to practitioners
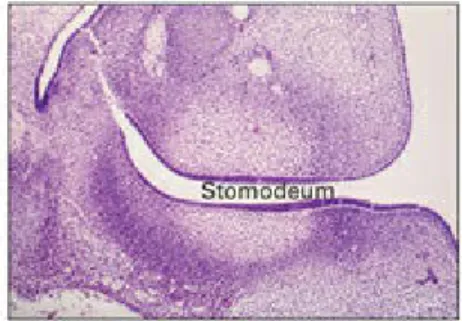
The development of occlusion begins during the 6th week of intrauterine life and ends after the age of 20 years. Neural crest cells begin migrating during the embryonic period, forming most of the facial structure.
Initiation stage
Odontogenesis (tooth development) begins with the budding of the dental lamina and continues into the next week of life. The vestibular lamina is another proliferation of the oral epithelium; occurs outside the dental lamina (buccal and labial).
Bud stage (proliferation stage)
Hypodontia: Congenital absence of a tooth may result from a lack of initiation or a stoppage of the proliferation of dental lamina cells. Hyperdontia: Overbite teeth are the result of a hyperactivity of the dental lamina and continued nodulation of the enamel organ.

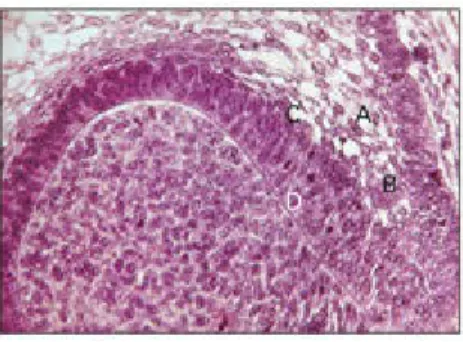
Cap stage (proliferation stage)
When epithelial resting cells are stimulated and become active, they take over secretory functions, which can result in cyst formation.
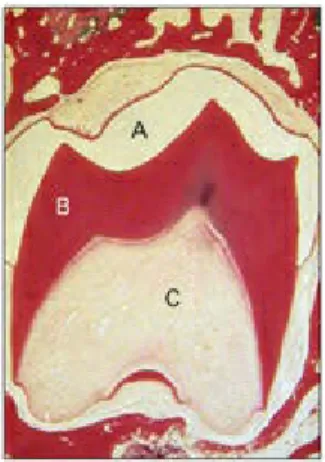
Early bell stage (histodifferentiation stage)
Odontoblasts differentiate under an organizing influence derived from cells of the inner dental epithelium. During this stage, cells of the dental papilla differentiate into odontoblasts, and cells of the inner dental epithelium differentiate into ameloblasts (Figures 2-11 and 2-12; see also Figs 2-6).
Late bell stage (morphodifferentiation stage)
Disturbances during the histodifferentiation phase of tooth formation cause abnormalities in the differentiation of the forming cells of the tooth germ. This, and the accompanying ectomesenchymal response, forms the tooth germs of the first, second, and third molars.
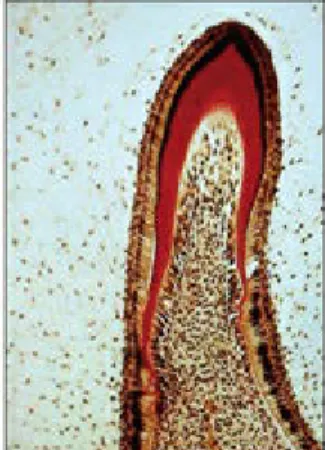
Mineralization of dental hard tissues (calcification stage)
As already mentioned, the formation of dentin always precedes the formation of enamel and marks the beginning of the crown phase of tooth development. This phase is associated with the formation of dental hard tissues, which begins around the 18th week (Fig. 2-14).
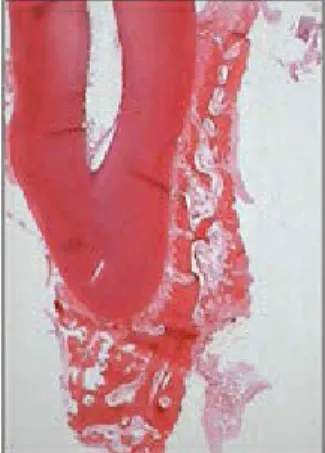
Root formation
The dental follicle lies outside the root sheath and forms the cementum, periodontal ligament (PDL) and alveolar bone. As the inner epithelial cells of the root sheath gradually envelop more and more of the expanding dental papilla, they initiate the differentiation of odontoblasts from cells at the periphery of the dental papilla.
Molecular level of tooth development
Ectomesenchymal cells in the dental follicle penetrate between the epithelial fenestrations and close to the newly formed dentin. When the root sheath fragments, ectomesenchymal cells in the dental follicle penetrate between the epithelial root sheath and the newly formed dentin of the root.
Role of form and function in occlusal development
Role of craniofacial growth in development of the dentition
Dental ankylosis, which leads to delayed tooth eruption and slows alveolar bone growth. The key importance of mandibular growth is also clear in the normal development of occlusion and facial growth.

Gum pads
The length and anterior width of the mandibular gum pad increases while the posterior width decreases. There is no relationship between the anterior openings of the gum pads and future open bite tendency.

Natal teeth
During the first year, the gum pads enlarge and the arches get bigger to accommodate all the teeth. The space between the gum pads is occupied by the tongue, which at this age is advanced in development and larger than the surrounding jaws.
Development of tooth germs
At the same time, rapid growth of the basal part of the jaw occurs in three dimensions. In the maxilla, the sagittal and transverse growth of the jaw is ensured by the rapid growth of the tuberosity and the middle palatine suture.
Tooth eruption
In transitional dentition, it is very important to preserve the perimeter of the dental arch of the primary tooth. A baby tooth without a gap is followed 40% of the time by crowding in a permanent tooth.

Terminal plane
Importance of the primary dentition
Exfoliation of the primary teeth
Marks and Cahill40 conducted an experimental study in dogs evaluating the effect of permanent tooth crowns. Thus, the pattern of primary root resorption depends on the position and size of the permanent follicle.
The average tooth accommodation resulting from interdental spacing is approximately 3.8 mm in the maxillary arch and 2.7 mm in the mandibular arch. The anterior position of the maxillary permanent incisors provides an increase of about 2.2 mm in the upper tooth and about 1.3 mm in the mandibular arch.

Maxillary permanent lateral incisors are also located behind the tip of the primary lateral incisors. Another problem after eruption of the lateral incisors is severe proclination accompanied by interdental spacing.
This phenomenon plays an important role in phase III of the transitional tooth, during the transition of canines and premolars. This situation can cause mesial displacement of the permanent first molar and loss of space for the premolars.
Dimensional arch changes during the transitional dentition
Crowding and third molars
Dental and skeletal malocclusions (sagittal, vertical and transverse malocclusions), such as Class I, Class II and Class III occlusions alone or in combination with other abnormalities such as.
Acknowledgment
The development of the teeth forms the basis for the clinical application of orthodontic treatments at a young age. A preliminary study of the morphology of the upper gingival pad at 6 months of age.
Patient’s chief complaint
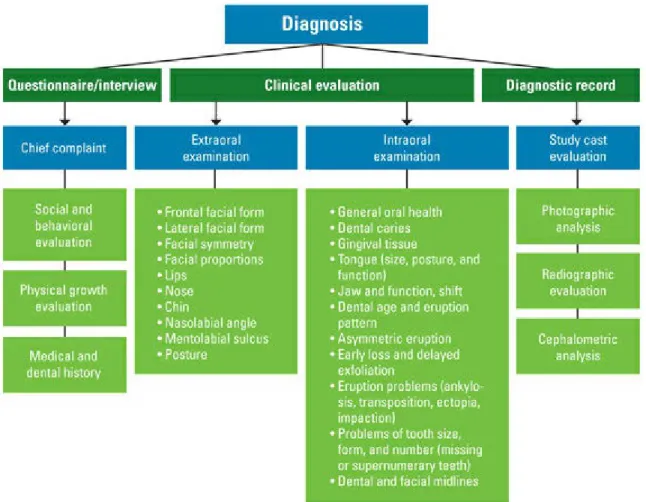
This type of form can be completed by patients or parents in advance to determine the patient's wishes, expectations and goals for orthodontics. The questionnaire can be divided into four sections: (1) the patient's chief complaint, (2) social and behavioral evaluation, (3) evaluation of physical growth, and (4) medical and dental history.
Social and behavioral evaluation
The main goal is to assess the patient's and parents' wishes and their social and behavioral statuses. Pre-treatment assessment of the patient's social and behavioral statuses is also important to understand the patient's expectations, especially for adult patients.
Physical growth evaluation
For this reason, asking about the patient's progress at school or the patient's relationship with friends or siblings may be helpful. Recognizing the patient's emotional or learning disability will help modify the treatment approach according to the patient's ability.
Medical and dental history
These components affect our perception of the face and must be carefully evaluated during diagnosis and treatment planning for orthodontic treatment. Esthetic evaluation of the patient's frontal and lateral appearance deserves special attention, especially in orthodontic treatment at an early age.
Frontal facial evaluation
Next, facial symmetry can be assessed by comparing the left and right sides of the face from the midline plane of the face (Fig. 3-2). The area from the subnasal to the stomion should be approximately one third of the total lower third of the face (subnasal to menton)11 (Fig. 3-5).

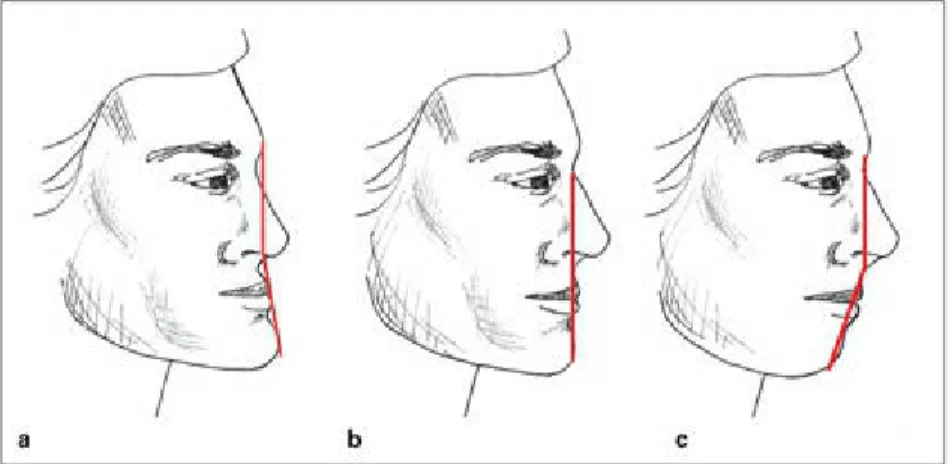
Lateral (sagittal) facial evaluation
The area from the subnasal to the stoma should be approximately one third of the entire lower third of the face. The morphology of the patient profile is another important area that can change the treatment plan.
Evaluation of the dentition
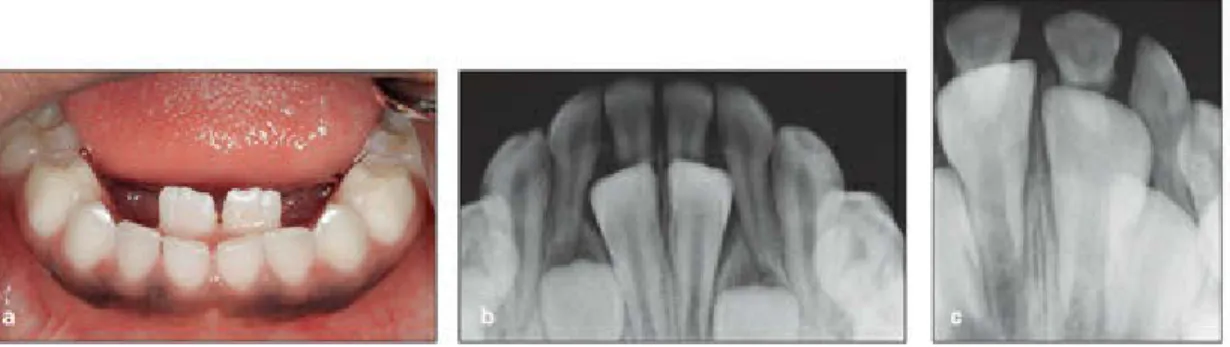
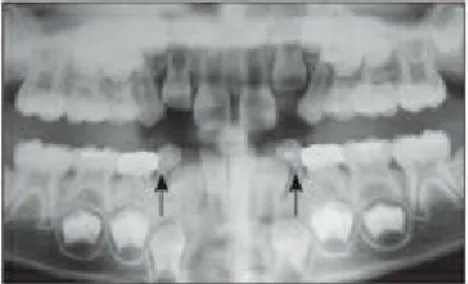
Other eruption problems, such as ankylosis, tooth transposition, ectopic eruption, and tooth impaction, should be evaluated clinically and radiographically (see Chapter 10). Problems of tooth size, shape and number (missing or supernumerary teeth) are other factors that can interfere with normal eruption and tooth movement.
Evaluation of soft tissues
The tongue has several necessary functions for life and at the same time can play an important role in the development of the occlusion. One of the factors that play an important role in the development of the occlusion is the balance between the tongue and the perioral muscle chain.

Assessment of TMJ function
The relationship between malocclusion and speech problems is another aspect of the patient's situation that must be evaluated before treatment planning. "Sunday bite" is another abnormal mandibular position that can be seen in some patients with skeletal class II malocclusion.
Type of occlusion
A set of good examination casts is part of the patient's record and is a useful tool for occlusal assessment and analysis in diagnosis and treatment planning. Vertical evaluation of study casts involves assessment of the vertical overlap of incisors, which is measured and recorded either in millimeters or as a percentage of the total height of the overlapping maxillary incisors above the mandibular incisors.
Arch form and symmetry
The vertical relationship of the posterior segment of the dentition should also be evaluated because some forms of buccal bite or Brodie syndrome involve increased overlap of the incisors. This type of asymmetry can be distinguished from arch asymmetry by careful evaluation with the symmetrograph, which can also reveal the mesiodistal shift of the dentition.
Mixed dentition space analysis
Correction of the Spee curve also requires additional space, which must be considered in space analysis. One purpose of space analysis under the mixed dentition is an estimation of the total mesiodistal width of unerupted permanent teeth to determine the space necessary for a well-aligned dentition.
Extraoral photography
The bridge of the nose, the base of the upper lip, and the chin are used to assess the patient's profile proportions. Both sides of the face relative to the midline of the face are equal and symmetrical vertically and horizontally (Fig. 3-19).

Intraoral photography
An important purpose of the intraoral photograph is to record the condition of the hard and soft tissues before treatment. In addition, a good set of intraoral photographs is a perfect tool for showing different views of the dental occlusion and any soft and hard tissue defects, such as enamel white spot lesions, hyperplastic areas, gingival problems and other soft tissue pathological conditions. .
Intraoral radiography
Good periapical radiography can also be used to accurately measure the mesiodistal crown width of unerupted canines and premolars for various spatial analyses. Occlusal radiography can also be used in evaluating the bucco-palatal relationships of supernumerary teeth or odontomas to other teeth in the arch.
Extraoral radiography
Good results were obtained, but there was some root resorption of the maxillary left lateral incisor. Accelerating eruption of the maxillary left premolar, an obstruction to the left canine, could have facilitated the eruption of the maxillary left canine.
Cephalometric radiography
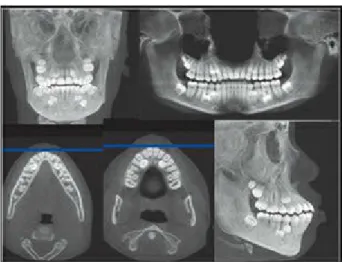
Another advantage of the cephalometric technique is prediction of the patient's growth pattern before treatment planning in early orthodontics. Another important role of cephalometry in orthodontics is the identification and classification of the patient's type of malocclusion.
Etiology of early primary tooth loss
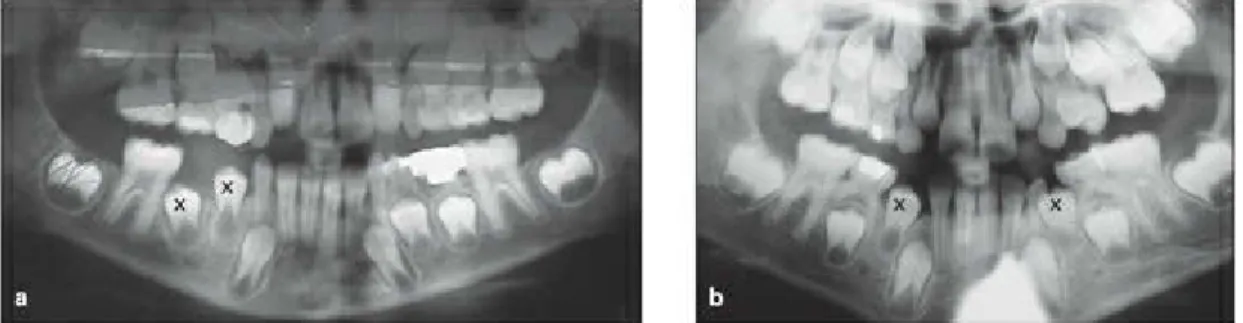
Effects of primary molar extraction on succedaneous teeth
After the age of 5 years, a gradual decrease in the delayed eruption of the premolars was observed in these patients, and at the ages of 8, 9 and 10 years, the eruption of the premolars was greatly accelerated. This study confirmed the delayed eruption of premolars and acceleration at the age of 8 to 10 years after early extraction of primary molars.
Incidence and nature of space closure
There is complete agreement that maxillary space closure is primarily caused by mesial movement of teeth behind the extraction space. In the mandible, space closure is primarily caused by the distal movement of the teeth in front of the space.
Prediction of tooth emergence
Factors influencing time of eruption
Factors influencing mesial or distal drift
For example, premature loss of the second primary molar, either in the maxilla or mandible, causes mesial displacement of the first permanent molar. Early loss of first primary molars can cause mesial displacement of posterior teeth and distal movement of anterior teeth (in the mandible mainly distal and in the maxilla mainly mesial).
Diagnostic procedures
The ratio of the 6 mandibular anterior measurements to the 6 maxillary anterior measurements (sum of mandibular 6 divided by the sum of maxillary 6, multiplied by 100) is the anterior ratio. The presence of any interdental space in the arch should be carefully measured and considered to ensure the accuracy of the overall space analysis.
Indications
Space maintenance is a procedure performed in the primary and mixed teeth to preserve the available space before any closures occur in the arch length. The use of a space maintainer device or restoration of a proximal carious lesion in the primary dentition at the right time can avoid the consequences of loss of arch length and the need for complex orthodontic treatment at a later stage.
Contraindications
Failure to maintain space
Ankylosis of the primary teeth, especially when they are below the level of occlusion, can result in the curvature of the adjacent teeth and loss of space, as well as excessive protrusion of the opposing tooth.
Qualities of a good space maintainer
Types of space maintainer
The front part of the bar is located in the deepest part of the palate. Another consequence of early loss in the mandible is the possibility of retroclination and overeruption of the permanent incisors (increased overbite and overbite).

Types of space regainer
It can be activated by slightly opening the loop to elevate the adjacent teeth (Fig 4-19). The rods attached to the palatal molar tube can be removed and the pusher coil can be reactivated (Fig. 4-23).

Tooth extraction
Sequential selective enamel stripping
Sagittal expansion
As Nance16 indicated, labial movement of the incisors can be extremely detrimental in some cases. The other option to increase the arch length in the sagittal direction is proclination of the incisors.
Transverse expansion
The removable distalizer is a Hawley appliance with an acrylic resin portion and a labial arch serving as anchorage. A jack screw is embedded in the acrylic resin and connected to the molars with some clamps (see Fig. 4-26). The screw is activated every 3 to 5 days to distalize the molar.