The development of principles and practices presented in this second edition will enable midwives and other health professionals to keep health promotion at the forefront of their midwifery practice. The popularity of this and other publications proves that midwifery and health promotion are very comfortable partners in the minds and hearts of midwives.
PREFACE
ACKNOWLEDGEMENTS
I would like to thank my partner Jean-Luc and children Anäis and Luc for their kind-hearted sharing of my time and focus for this chapter, and editors Jan and Vicky for their good-natured help.
LIST OF TABLES
PUBLIC HEALTH, MIDWIFERY AND GOVERNMENT POLICY
BACKGROUND TO MIDWIFERY, PUBLIC HEALTH AND GOVERNMENT POLICY
WHY NOW? FACTORS INFLUENCING GOVERNMENT OPINION ON MIDWIFERY AND PUBLIC HEALTH
Many of the women who died were not followed up properly because they did not seek care despite known risk factors. They talk about public health and the role of motherhood in preventing disease and prolonging life.
CURRENT POLICY ON PUBLIC HEALTH
DoH (2004b, p. 5) There is also confirmation within the NSF of the government's objective to involve local communities in the development and planning of services. Meaningful engagement with the local community in service planning will be a challenge to the strength of service providers.
IMPLEMENTING PUBLIC HEALTH: WHAT MIGHT IT MEAN?
A possible model for strengthening community involvement could come from the Sure-Start initiative, where local committees are made up of local parents (who are elected at annual meetings) and local service providers. In addition, Sure-Start committees can decide the direction of the local Sure-Start scheme and its budgets.
Organizational change
Helping pregnant women to quit smoking, encouraging good nutrition (particularly through the Healthy Start Welfare Food Scheme) and increasing breastfeeding rates are also mentioned in the NSF. The NSF suggests that the length of time women and their families receive care from midwifery-led services should be at least a month and up to 3 months, depending on individual need.
The focus of maternity care
Multidisciplinary working
To enable midwives to multidisciplinary working Edwards et al. 2005) advocates the establishment of networks that have a common link through the consultant midwife in public health. Through the activity of a consultant midwife, the obstetric services are more integrated into local public health initiatives.
BARRIERS TO THE EXPANSION OF AN ENHANCED MIDWIFERY PUBLIC HEALTH ROLE
The failure to expand the role of midwives in public health may be a result of the ambiguity of midwives. A piece of research relevant to the development of a midwifery role in public health is that conducted by Hunt (2004).
POSITIVE FACTORS IN THE EXPANSION OF THE PUBLIC HEALTH ROLE OF THE MIDWIFE
Another factor that may limit the feasibility of the public health initiatives proposed in the NSF is the ability of midwives to increase the level of partnership. A lack of good quality research into effective interventions to improve public health is also a problem when deciding how the role of the midwife in public health should develop (Wanless 2004).
SUMMARY OF KEY POINTS
HEALTH PROMOTION AND THE MIDWIFE
CONCEPTS OF HEALTH
Health is also influenced by a host of external factors such as wealth, education, housing, employment and social networks. This holistic view of health has led to a new approach to health promotion called salutogenesis, which the Royal College of Midwives (RCM) is using in its campaign for normal birth (RCM 2002).
Reflection – 1
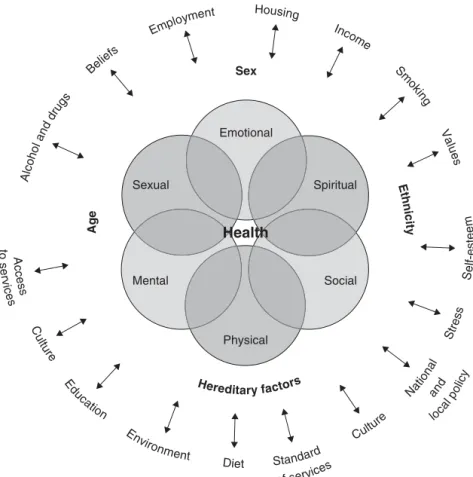
The World Health Organization (WHO) used all three concepts as the underlying basis of its constitution in 1946 when it declared that health is 'a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity. ' (WHO 1946, p. 2). The physical, sexual, emotional, mental, social and spiritual aspects of health are interrelated and codependent.
THE INFLUENCES ON HEALTH
Lifestyle behavior and one's ability to assess health risk and make a healthier choice is a compelling argument when discussing influences on health (Dufty 2005). Social and environmental influences will shape an individual's ability to assess health risks and influence the ability to make the healthier choice.
WHAT IS HEALTH PROMOTION?
Health promotion is a positive concept that emphasizes social and personal resources and physical capabilities. Therefore, health promotion is not only the responsibility of the health sector, but goes beyond a healthy lifestyle and well-being.
SALUTOGENESIS: A HOLISTIC APPROACH TO HEALTH PROMOTION IN MIDWIFERY?
The same applies to the health promotion activities carried out by the midwife who works one-on-one with her clients; exploring and respecting each woman's knowledge and opinions is vital if a woman is to feel that these health promotion activities and indeed her midwifery care have value to her (Milburn 1996). Health promotion can only be effective if it is understood that health depends on a multitude of factors with complex and as yet poorly understood interrelationships.
NEEDS IN HEALTH PROMOTION
In addition, a normative need identified by a professional may differ significantly from the client's needs. With a comparative need, there is a comparison between two different groups, some receiving a health promotion activity or project and some not - the latter being identified as being in need.
THE AIMS OF HEALTH PROMOTION
The goals of a health promotion activity or project should reflect the needs of the users, not the needs of the midwife. Milburn M (1996) The importance of lay theorizing for health promotion research and practice. Health Promotion International 11: 41–6.
FURTHER READING
Teenage Pregnancy Unit (2003) Sure Start Plus pilot program – National evaluation of Sure Start Plus.London: Teenage Pregnancy Unit. Wiggins M, Austerberry H, Rosato M, Sawtell M, Oliver S (2003) Start Plus National Assessment Service Delivery Study: Interim Findings.
FACTORS AFFECTING HEALTH PROMOTION
WHAT MAKES WOMEN DIFFERENT?
However, regardless of gender, there is evidence that it is too easy to assume that information provided for health education is accepted unconditionally. We know that health education information is interpreted and this interpretation depends on existing beliefs (Joffe 2002).
FAMILY, HOME AND EXPECTATIONS
If health education does not necessarily change behavior by changing beliefs, there is a need to look beyond this simplistic relationship and consider the health promotion model. There are mediating factors that are specific to women and will influence their response to health education or health promotion.
WOMEN’S PLACE IN SOCIETY
Although this would not necessarily be recognized as a core health promotion priority, it certainly is for these women. Women may also have priorities that they believe promote health, which may be outside the purview of the biomedical model of health.
WOMEN AND POVERTY
This theory has been criticized for placing too much emphasis on the individual at the expense of an understanding of the place of family, community and environment in mediating women's health choices. The constraints of being poor can also mean that women's priorities are at odds with prevailing health promotion priorities, thus making promotion messages irrelevant in women's everyday lives.
BLACK AND ETHNIC MINORITY WOMEN
At the clinic there is usually a long waiting time, and as your appointment is at 11.30 you will be there over lunchtime; there is also nowhere for children to play. Think about how local prenatal clinic services can be reorganized to make your life easier.
FINDING WAYS TO REACH WOMEN
Practical change: making healthy choice easier
As can be seen from the list above, there are ways to make it easier for women to make healthier choices and in its broadest sense this is health promotion. It could be argued that it is unreasonable to expect women to make healthy choices, in response to increased knowledge or awareness, without practical changes.
Empowerment
The alternative timing of the clinics appeared to increase the number of women attended (Pearce and Mayho 2004). The aim of the project is for advocates to provide support, health promotion and referrals where necessary.
USING HEALTH PROMOTION MODELS AND APPROACHES IN MIDWIFERY
DEFINING TERMS
This is a single physical representation of a set of ideas, often schematic, that helps guide our thinking and understanding of the underlying philosophical issues of both theory and practice. This is an organized or integrated set of propositions, which may or may not have been tested for their validity in relation to other theories put forward to explain the same situation.
WHY USE MODELS AND APPROACHES IN HEALTH PROMOTION?
Therefore, ideology determines not only which model of health promotion to use, but also whether an intervention to promote health is desirable, worthwhile, or even ethical (Seedhouse 2003).
APPLYING HEALTH PROMOTION MODELS AND APPROACHES TO MIDWIFERY CARE
Ewles and Simnett developed a framework of five approaches to health promotion in 1985, which was further developed in 1992 (Ewles and Simnett 1992). We must select for ourselves the purpose and activities we undertake, in accordance with our own professional code of conduct (if any), our own carefully considered needs and our own assessment of the needs of our clients.
The medical approach
In our opinion, there is no "right" goal for health promotion and no right approach or set of activities.
The behaviour change approach
The educational approach
The client-centred approach
The societal change approach
The difference between the two is that Ewles and Simnett (2003) construct their design from the perspective of the health promoter, while Downie et al. 1996) perspective is that of the outcomes of health promotion. The main criticism of Ewles and Simnett's approach must be that, when describing it from the health promoter's perspective, it does not take into account possible outcomes of health promotion.
USING HEALTH PROMOTION MODELS AND APPROACHES IN MIDWIFERY
Similar themes run through many of the health promotion models and approaches currently in practice, but each has a different area of focus. Health promotion models and approaches provide an incentive to examine and rethink practice and its underlying assumptions.
EVALUATING HEALTH PROMOTION ACTIVITIES
WHAT IS EVALUATION AND WHY DO IT?
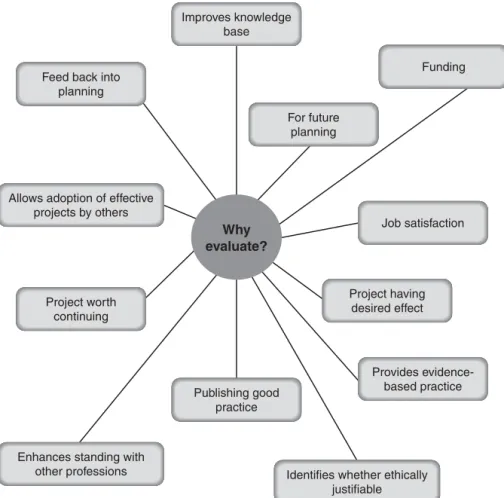
There are various criteria that can be used when evaluating a health promotion activity for its value. Despite this debate, there are many possible reasons why evaluation is required and needed within health promotion and Figure 5.1 identifies the possible reasons for evaluation.
WHO IS IT FOR AND WHO SHOULD DO IT?
USER EVALUATION
Training of professionals must also be considered to enable them to understand lay perspectives and work effectively with users in different situations (Entwistle et al. 1998, Trivedi and Wykes 2002).
HOW BEST TO EVALUATE SUCCESS?
- Problem definition
- Solution generation
- Testing innovation
- Intervention demonstration
- Intervention dissemination
- Programme management
Evaluation of a health promotion project is usually about identifying the effects of the project. At this stage, the evaluation tasks are totally directed towards the maintenance of the project.
CHALLENGES TO EVALUATION IN HEALTH PROMOTION
It would be very difficult to prevent the health promotion project from 'trickle-down' beyond the intended target group (Naidoo and Wills 2000). As a result of the health promotion process, a health promotion project may have different outcomes at different times during the life of the project.
ATTITUDES, VALUES AND HEALTH BEHAVIOURS
DEFINING BELIEFS, VALUES, INSTINCTS, DRIVES AND ATTITUDES
Belief
These beliefs are shaped and influenced by many factors, such as personality, family, friends, culture and education, and may not be supported by reliable facts as in the second example mentioned above or by the majority of the population. They are based on the individual's own evaluation of the situation or item and take time to change (Naidoo and Wills, 2000, Katz and Perberdy, 2001).
Values
Instincts
Drives
Attitudes
FACTORS AFFECTING BELIEFS, VALUES AND ATTITUDES
Gender
Culture
Peer groups
Personality
Those high in extraversion are more likely to engage in positive health behaviors, but strong peer pressure can influence negative health behaviors such as smoking, unsafe sex, and drug use. Those with high levels of agreeableness and conscientiousness were found to have positive health behaviors and a more sustained approach to positive health behavior changes.
HOW ARE ATTITUDES FORMED?
Those who report high levels of openness may also report negative health behaviors such as drug use. Maslow developed the widely used 'hierarchy of needs', which encapsulates the development of personality from birth to adulthood, based on the philosophy that under normal circumstances people are motivated or moved to achieve more and more sophisticated needs in order to find self-fulfillment and 'self-actualisation' – the feeling of being comfortable with oneself.
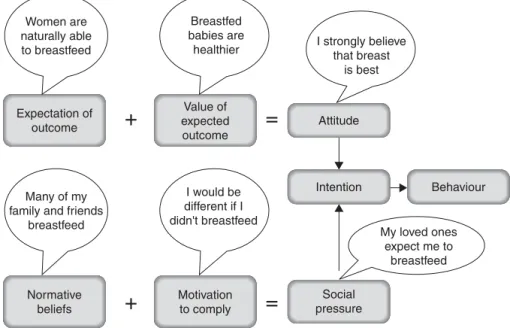
THE RELATIONSHIP BETWEEN ATTITUDES AND HEALTH BEHAVIOURS
Individuals differ in the extent to which they believe they can change their lives. Although Ajzen and Fishbein (1980) suggest that their theory can be used to predict and understand attitudes and behavior, the theory does not include basic instincts or drives.
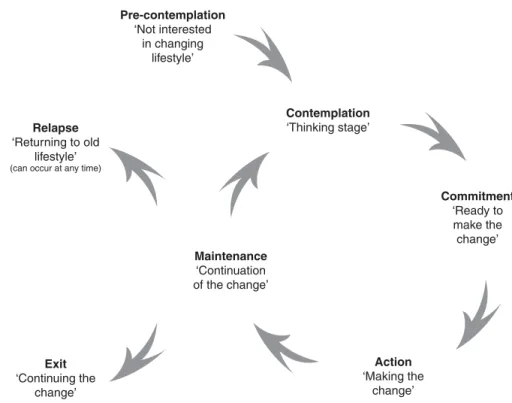
THE TRANSTHEORETICAL APPROACH TO HEALTH BEHAVIOUR CHANGE
- The pre-contemplation stage
- The contemplation stage
- The commitment stage
- The action stage
- The maintenance stage
- The exit stage
- The relapse stage
This is where the health behavior change starts and can take up to 6 months (Prochaska 2005). A woman entering this phase of the approach is making a serious decision to change her negative health behaviors.
INFORMATION GIVING IN HEALTH PROMOTION
COMMUNICATING HEALTH
ENSURING QUALITY OF INFORMATION
The quality of presentation was discussed; now the quality of the information itself must be reviewed. This is a big issue because there is a consistent bombardment of 'health' messages all day - information is provided by many different parties, e.g.
Exercise – 1
The way the health risk or health change is presented can 'manipulate' how the person receiving the information perceives it, and this in turn can influence decision-making and health behaviour. However, if the topic is considered unimportant, the end of the message will be remembered more than the beginning.
Exercise – 2
Reliability: The source of the content is trustworthy and the content is kept up to date. Timeliness: Content is delivered or available when the audience is most receptive or needs specific information.
FACE-TO-FACE COMMUNICATION
You may need to set aside time to review the quality of information provided by your department so that you can discuss the issues with the woman in confidence. This includes accepting the woman and her family without judging who they are or their lifestyle.
INFORMATION FROM THE MEDIA
The use of oral presentations, video and leaflets in the relevant language have all proven very useful in improving communication. The use of mass media to convey health messages has had mixed success (Tones and Tilford 2001, Slater 2005).
Exercise – 3
Many of you may remember the HIV “don't die of ignorance” campaign in the early 1980s. Many different means of communication are used to convey this health message to a wide audience.
Leaflets and the printed word
Leaflets are considered expert opinion, but there is some evidence to show that different leaflets on the same subject are not always consistent in the information they provide, e.g. The answer to these questions depends on the target group and the purpose of the leaflet.
Exercise – 4
There is an ongoing tension about what information should be given – general advice or specific information – and how much (Payne 2002). When giving a leaflet, the midwife should be aware of its contents and so be able to talk to the woman or her family about the contents and where they can go for further information.
INFORMATION TECHNOLOGY
Searching for health information using a search engine is the third most common use of the Internet (Bernstam et al. 2005). In a review of 273 instruments, none were found to be user-friendly (Bernstam et al. 2005).
Exercise – 5
For midwives, the internet can be an invaluable resource, but ensure the quality of the information. Midwives who propose to use the Internet should be available to discuss questions that may arise based on the information found and to review the quality of the information obtained.
INTERNET SITES
HEALTH PROMOTION IN MIDWIFERY TRAINING
PHILOSOPHY OF CARE AND EDUCATION IN THE CURRICULUM
This in turn will facilitate them to recognize the concept that learning is a lifelong process so that they will continue to develop as individuals and midwives after registration.
WHAT INFORMED THE CURRICULUM?
The courses in the program reflect the health promotion role of the midwife, as outlined in the numerous documents mentioned above, and seek to prepare students for their role as autonomous practitioners. The clinical placements and the midwives who mentor the students play an important role in the preparation of the student.
PREPARING STUDENT MIDWIVES FOR THEIR HEALTH PROMOTION ROLE
In this module students look at the theory and approaches of health promotion and public health. Women's mental health is an extremely important element of health promotion in midwifery (see Chapter 13).
PARTNERSHIP WORKING AND THE MIDWIFE
A BRIEF HISTORY OF PUBLIC HEALTH AND PARTNERSHIP WORKING
There have also been a number of recent publications identifying the important role of midwives in public health. The most important confirmation of the role of the midwife in public health and in working in partnerships can be found in the National Service Framework for Children, Young People and Maternity Services, where strengthening partnership is a key objective (DoH 2004b).
THE CONCEPT OF PARTNERSHIP WORKING
Key national policies – Making a Difference (DoH 1999a), Saving Lives: Our healthier nation (DoH 1999b) – have further identified an increasing focus on public health for obstetrics to strengthen the public health agenda. The success of collaborative projects with midwives within the Sure-Start and Sure-Start Plus programmes, such as the safer sex enterprise in Powys, Wales (Lewis 2004), provides a strong practical example of all these policy recommendations regarding the role of the midwife in public health. .
STRUCTURE AND FORMAT OF PARTNERSHIPS
PARTNERSHIP WORKING AND SOCIAL CAPITAL
BENEFITS TO PARTNERSHIP WORKING
CHALLENGES OF PARTNERSHIP WORKING
This is especially true in relation to the untapped potential that midwives have to contribute to partnership and public health. Midwives play an important role in reducing health inequalities and contribute to the public health agenda.
SEXUAL HEALTH PROMOTION IN MIDWIFERY PRACTICE
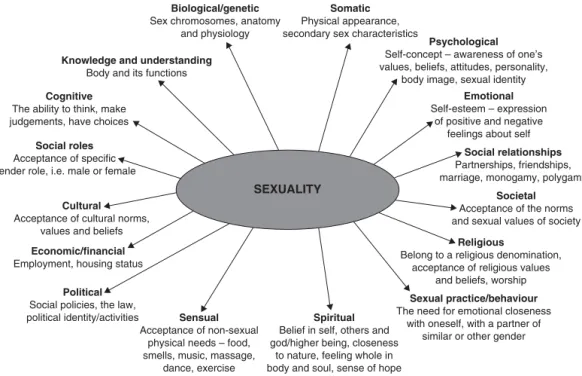
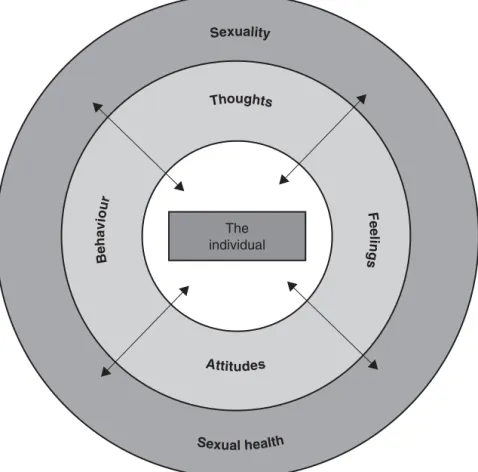
THE CONCEPT OF SEXUAL HEALTH
The definitions suggest that sexual health is defined and experienced personally and can mean different things to different people. An individual's commitment to achieving and maintaining their sexual health is influenced by their worldview and life experiences.
Perceptions of self
It is important that individuals recognize and acknowledge their current position on the continuum and take appropriate action if they are to achieve and maintain optimal sexual health. Definitions of sexual health also suggest that it is a multidimensional concept underpinned by a number of dynamic and changing entities that identify a person as a unique human being, including the following aspects.
Expressions of sexuality
Sexual values and belief system
Sexual attitudes
Sexual behaviours
Perceptions of ‘sex’
THE CONCEPT OF SEXUAL HEALTH PROMOTION
SEXUAL HEALTH PROMOTION AND THE MIDWIFE
CHALLENGES TO SEXUAL HEALTH PROMOTION
Ultimately, they may believe that a comprehensive and more holistic approach to sexual health promotion is the responsibility of other health care professionals in other care settings, and nothing to do with them. Some midwives may also view the lack of substantive guidance, from the Royal College of Midwives or employed NHS trusts, on standards for effective and efficient sexual health promotion, as indicative of low professional emphasis.
KNOWLEDGE, ATTITUDES AND SKILLS FOR SEXUAL HEALTH PROMOTION IN MIDWIFERY PRACTICE
At the end of the assessment, the woman's sexual health priorities should be agreed and care planned accordingly. World Health Organization (1998) Definition of reproductive sexual health – available online at www.who.int (accessed March 2005).
PROMOTING BREASTFEEDING
WHAT WORKS?
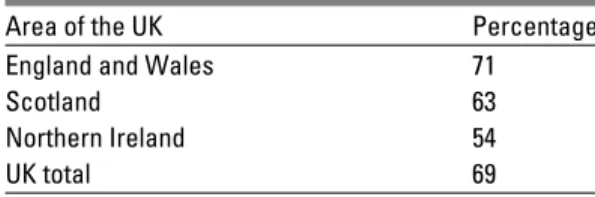
INFANT FEEDING 2000 SURVEY
The survey is based on an initial nationally representative sample of almost 9,500 mother-baby pairs born in the UK during 2000 and makes interesting reading, providing some of the best available insight into breastfeeding trends. The survey provides figures for the whole of the United Kingdom and divides the United Kingdom into three sections: Scotland, Northern Ireland and England and Wales.
Incidence of breastfeeding
Prevalence of breastfeeding
Duration of breastfeeding and effect of events around birth
HEALTH PROMOTION: WHOM ARE WE TARGETING?
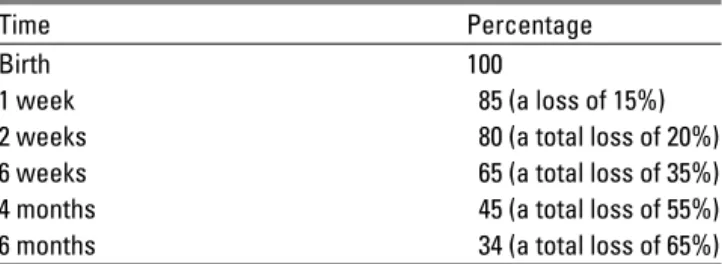
The ‘lost 20 per cent cascade’ and becoming part of it
MIDWIVES, ATTITUDES, KNOWLEDGE AND SKILLS
The UNICEF UK Baby Friendly Initiative
EFFECTIVE CLINICAL PRACTICES AND ANTENATAL EDUCATION
Ask a female relative or friend who is over retirement age about their experience feeding their baby(s).
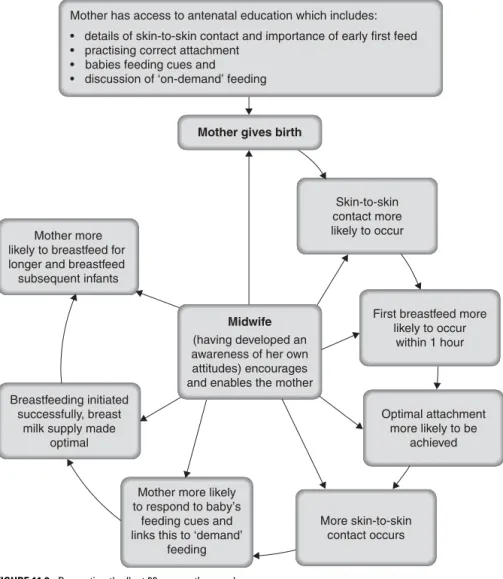
MOTHER AND BABY SKIN-TO-SKIN CONTACT AND EARLY INITIATION OF BREASTFEEDING
OPTIMAL POSITIONING AND ATTACHMENT AT THE BREAST
MOTHER AND INFANT POSITIONS
Stages of achieving optimal attachment using a cross-cradle hold
- Figure 11.4a)
- Figure 11.4b)
- Figure 11.4c)
- Figure 11.4d)
- Figure 11.4e)
- Figure 11.4f)
This is seen in clinical practice as the mother's nipple 'flattening' and losing its shape when the baby detaches from the breast. When signs of optimal attachment are present and the mother feels comfortable, she can gently let go of her breast and bring her hand to the diaper so that the baby is cradled in her hand with his head nestled in the crook of her arm. on her elbow.
THE ‘DEMAND’ FEEDING CONCEPT AND THE INFLUENCE OF ATTITUDES
WHICH BABIES CAN BE RELIED UPON TO LEAD THEIR OWN FEEDING?
Reflection – 2
These mother-baby pairs need to be observed and assessed by the midwife for hours before deciding whether intervention is needed. Red means that the baby cannot reliably 'self-feed' and that intervention is required to establish breastfeeding.
Green’
Amber’
Red’
WHICH MOTHERS CAN RESPOND APPROPRIATELY TO THEIR BABY’S FEEDING CUES?
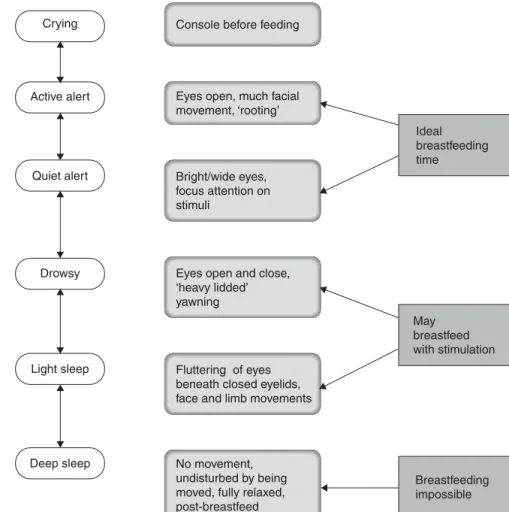
Feeding cues and sleep states
Reflection – 3
The Infant Feeding 2000 survey (Hamlyn et al. 2002) provides the most comprehensive overview of breastfeeding prevalence in the UK. The Baby Friendly Initiative (BFI) has proven to be an effective initiative in promoting breastfeeding.
General breastfeeding texts
Broadfoot M, Britten J, Tappin DM, MacKenzie, JM (2005) The baby-friendly hospital initiative and breastfeeding rates in Scotland. Thomson ME, Hartstock TG, Larson C (1997) The importance of immediate postnatal contact: its effect on breastfeeding.
Examining the research base for care
Correct attachment
Sleep states and feeding cues
Demand’ feeding
Skin-to-skin contact
FURTHER RESOURCES
SMOKING, PREGNANCY AND THE MIDWIFE
GOVERNMENT POLICY AND TARGETS FOR SMOKING CESSATION
The Children, Young People and Maternity Services Framework (NSF) (DoH 2004b) states that pregnant women and their partners who smoke should receive clear information about the dangers of smoking, as well as support from cessation services. of tobacco, such as the National Health Service (NHS) Stop Smoking Service. This is where advice and support can be provided before conception, as well as information about the dangers of second-hand smoke or second-hand smoke.
Smoking cessation targets
Around one third of perinatal deaths are attributed to smoking and this can be minimized if care is provided by integrated multidisciplinary and multi-agency teams (DoH 2004b).
SERVICE RECOMMENDATIONS
If women are not asked about their smoking, referrals to specialist midwives or smoking cessation specialists will not be made. Despite referral to the PCT smoking cessation unit, many women do not respond and some may prefer care from their named midwife or require telephone calls or home visits from the smoking cessation midwife, particularly if they have young children and experience difficulty going out. (West et al. 2003b).
EFFECTS OF SMOKING TOBACCO
Women who do not smoke at all or deny that they smoke present a challenge to the woman giving birth. Regardless, as mentioned earlier, the midwife must first identify women and their partners who may be ready to quit smoking.
MOTIVATIONS AND DIFFICULTIES ENCOUNTERED BY SMOKERS
ATTITUDES TOWARDS TOBACCO SMOKING
The woman can be encouraged by the midwife's success in quitting smoking and remaining a non-smoker so that strategies can be discussed more personally. The presence of a pregnancy or the planning of a pregnancy can be sufficient motivation for the woman and her partner to quit smoking.
STRATEGIES FOR SMOKING CESSATION
Having adopted a positive frame of mind and established a good rapport, to share information about the effects of smoking and the benefits of quitting with the woman and her partner, the midwife uses the knowledge and skills to spend quality time, perhaps for the first time. address these health promotion issues. The midwife will use her interpersonal skills to determine the best approach to take in each subsequent interaction to convey messages.
Case study – 1
The midwife can begin these strategies by referring the client to a smoking cessation service, or by relying on the midwife as the main healthcare provider involved with the woman in her quest to quit smoking (NICE 2002, West et al. 2000, RCM 2002). The midwife plays an important health promotion role in identifying pregnant women who smoke and harnessing their eagerness to quit once all the facts are known.
USEFUL INFORMATION AND CONTACTS
Pullon S, McLeod D, Benn C et al. 2003) Smoking cessation in New Zealand: education and resources for midwives for women who smoke during pregnancy. Woods SE, Lake JR, Springett J (2003) Addressing health inequalities and the HAZ smoking cessation programme: the perfect match.
THE CHALLENGE OF MENTAL HEALTH PROMOTION
THE BACKGROUND TO MENTAL HEALTH AND MIDWIFERY
A psychiatrist should evaluate all women with a previous history of mental health in the antenatal period and initiate a plan of care. Future research should seek to collect information from mental health services in cases where mental illness is the cause of maternal death.
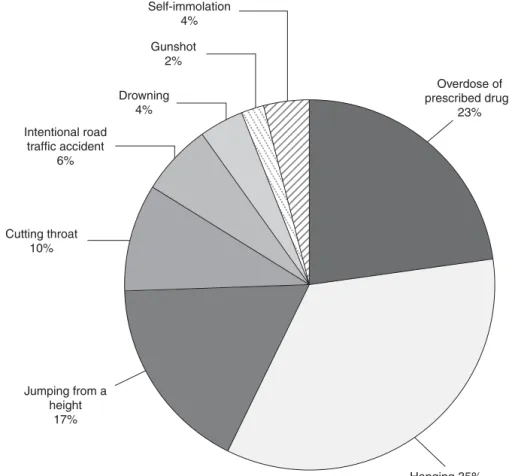
Chosen methods of suicide
DEFINING MENTAL HEALTH AND MENTAL HEALTH PROMOTION
This reveals the subjective nature of the concept of mental health and the difficulty in trying to develop an independent definition. It may be easier, in practical terms, to look at the opposite of mental health and define mental illness instead.
FACTORS AFFECTING MENTAL HEALTH
VULNERABLE GROUPS
Psychosocial factors
Biological factors
Psychiatric/emotional factors
Many of the women who experience severe baby blues develop PND (O'Hara 1997). A qualitative study by Green (1990) that looked at mood rather than depression found that women who were happy to be pregnant remained happy in the puerperium.
Obstetric/gynaecological factors
FACTORS THAT MAY AFFECT MATERNAL MENTAL HEALTH
ATTITUDES AND MENTAL HEALTH The midwife’s attitudes
THE EFFECTS OF MENTAL HEALTH LOSS Antenatal mental ill-health
On mother–infant interaction
THE ROLE OF THE MIDWIFE
Mental health promotion, screening for mental illness and supporting women with mental health issues
Mental problems will affect the health of the women, her partner and her child. Mental health promotion is an urgent area that midwives must address in their practice.
WEBSITE
Williams A, Ware J, Donald C (1981) A Model of Mental Health, Life Events and Social Support Applied to General Populations.
DOMESTIC VIOLENCE AND HEALTH PROMOTION: MIDWIVES CAN MAKE
OVERVIEW AND EPIDEMIOLOGY OF DOMESTIC VIOLENCE
Unlike many other industrialized countries, there is no national UK prevalence study of domestic violence. Domestic violence is also more likely to result in injury than other forms of assault.
PHYSICAL HEALTH EFFECTS OF DOMESTIC VIOLENCE
DOMESTIC VIOLENCE AND WOMEN’S SEXUAL HEALTH
Sexual violence crosses the domains of women's health, sexuality, and childbirth, and research on domestic violence and abuse of women has capitalized on this overlap. These findings highlight the seriousness of sexual violence, not only in terms of prevalence during pregnancy, but also the multiple victimization of women.
DOMESTIC VIOLENCE DURING PREGNANCY