For children new to methylphenidate, the starting dose is 18 mg once daily in the morning. For ADHD patients new to methylphenidate, the starting dose is 20 mg once daily in the morning.
Adrenergic Agonists
Because these antidepressants are less effective and more dangerous than the stimulants, they are considered second-line drugs. However, these antidepressants are less effective than CNS stimulants and are not approved for ADHD.
KEY POINTS
Warn patients of cardiovascular reactions (palpitations, hypertension, angina, arrhythmias) and instruct them to notify the prescriber if these occur. Inform patients of signs of hypersensitivity (erythema, edema, papules, vesicles) and instruct them to inform the prescriber if these occur.
Summary of Major Nursing Implications a —cont’d
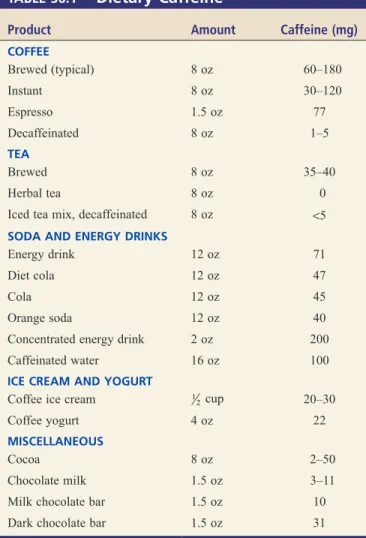
Advise patients to take the morning dose after breakfast and the last daily dose in the early afternoon to minimize interference with eating. Inform patients of cardiovascular reactions to caffeine (palpitations, rapid pulse, dizziness) and instruct them to discontinue caffeine if these occur.
Basic Considerations
DEFINITIONS Drug Abuse
DIAGNOSTIC CRITERIA REGARDING SUBSTANCE USE DISORDER
FACTORS THAT CONTRIBUTE TO SUBSTANCE USE DISORDER
Reinforcing Properties of Drugs
Substance Use Disorder
Other Definitions
Drug Availability
Vulnerability of the Individual
NEUROBIOLOGY OF SUBSTANCE USE DISORDER
Physical Dependence
Psychologic Dependence
Social Factors
PRINCIPLES OF SUBSTANCE USE DISORDER TREATMENT
DEA Schedules
Prescriptions
THE CONTROLLED SUBSTANCES ACT
Record Keeping
State Laws
Labeling
Physical dependence is a condition in which withdrawal syndrome will occur if drug use is stopped. Although physical dependence is not the same as SUD, physical dependence can certainly contribute to addictive behavior.
BASIC PHARMACOLOGY OF ALCOHOL Central Nervous System Effects
Not all cardiovascular effects of alcohol are harmful: there is clear evidence that people who drink moderately (2 drinks per day or less for men, 1 drink per day or less for women) have lower rates of ischemic stroke and coronary artery disease (CAD) , myocardial infarction (MI) and heart failure than teetotalers. Moderate drinking protects against cardiovascular disease, mainly by increasing high-density lipoprotein cholesterol (HDL).
Other Pharmacologic Effects
In addition to causing FASD and FAS, heavy drinking during pregnancy can result in stillbirth, miscarriage, and the birth of an alcohol-dependent baby. Therefore, regardless of the studies noted, the American College of Obstetricians and Gynecologists (ACOG) continues to maintain its long-held position that no amount of alcohol can be considered safe during pregnancy.
Impact on Longevity
If there is an amount of alcohol that is safe during pregnancy, that amount is very low. The information in Table 38.2 helps to explain why we cannot metabolize more than 1 alcoholic drink per hour.
Pharmacokinetics
Since the liver can metabolize about 15 mL of alcohol per hour, and since the average alcoholic drink contains 18 mL of alcohol, 1 drink contains almost as much alcohol as the liver can comfortably process every hour. Because alcohol in the brain quickly equilibrates with alcohol in the blood, blood alcohol levels can predict effects on the central nervous system.
Tolerance
The first effects (euphoria, reduced inhibitions, increased self-confidence) are observed when the blood alcohol content is approximately 0.05%. When blood alcohol levels exceed 0.4%, there is a significant risk of respiratory depression, peripheral collapse and death.
Drug Interactions
Safety Alert
Acute Overdose
Precautions and Contraindications
Pharmacodynamic tolerance is demonstrated by an increase in the blood alcohol level necessary for intoxication to occur. Alcohol should be avoided during pregnancy due to the risk of FASD (including FAS), stillbirth, miscarriage, and neurodevelopmental abnormalities.
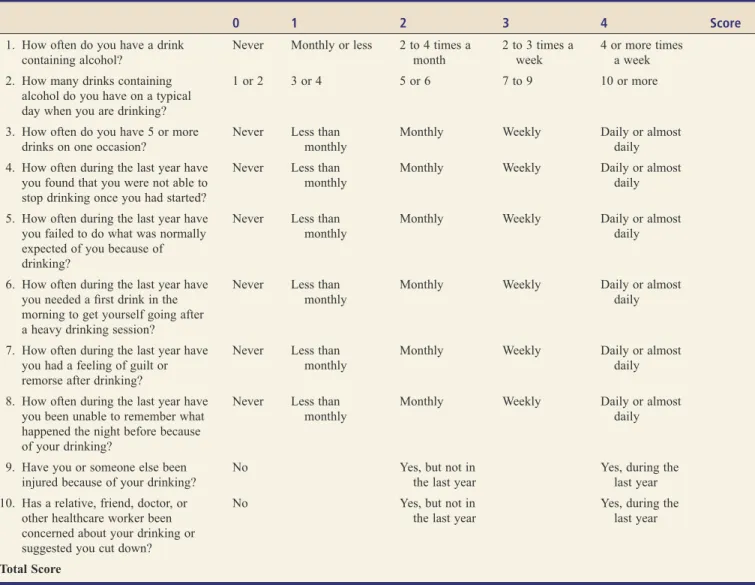
ALCOHOL USE DISORDER (AUD)
How often during the past year have you needed a first drink in the morning to get yourself going after a heavy drinking session. How often during the past year have you felt guilty or remorseful after drinking.
Drugs Used to Maintain Abstinence
Although all benzodiazepines are effective, agents with longer half-lives are generally preferred because they provide the greatest protection against seizures and breakthrough symptoms. Agents that have been tried include carbamazepine (an antiepileptic drug), clonidine (an alpha2-adrenergic agonist), and atenolol and propranolol (beta-adrenergic blockers).
DRUGS FOR ALCOHOL USE DISORDER
Drugs Used to Facilitate Withdrawal
The recommended dose is 2 tablets (666 mg) 3 times a day, taken with meals. The reason for administration with meals is to promote compliance - not to affect absorption or GI effects.) Dosing should begin immediately after detoxification is complete and should be continued even if relapse occurs. Acamprosate reduces tension, anxiety and other unpleasant feelings caused by alcohol withdrawal.
Nicotine and Smoking
BASIC PHARMACOLOGY OF NICOTINE Mechanism of Action
Pharmacologic Effects
Acute Poisoning
Chronic Toxicity From Smoking
Tolerance and Dependence
Prototype Drugs
A non-nicotine product -- bupropion extended-release (bupropion SR) [Zyban, Buproban] and varenicline [Chantix, Champix ] -- are taken to reduce nicotine cravings and to control withdrawal symptoms. The most effective drug therapies for smoking cessation are varenicline alone and the nicotine patch combined with a short-acting nicotine product (ie, nasal spray or gum).
PHARMACOLOGIC AIDS TO SMOKING CESSATION
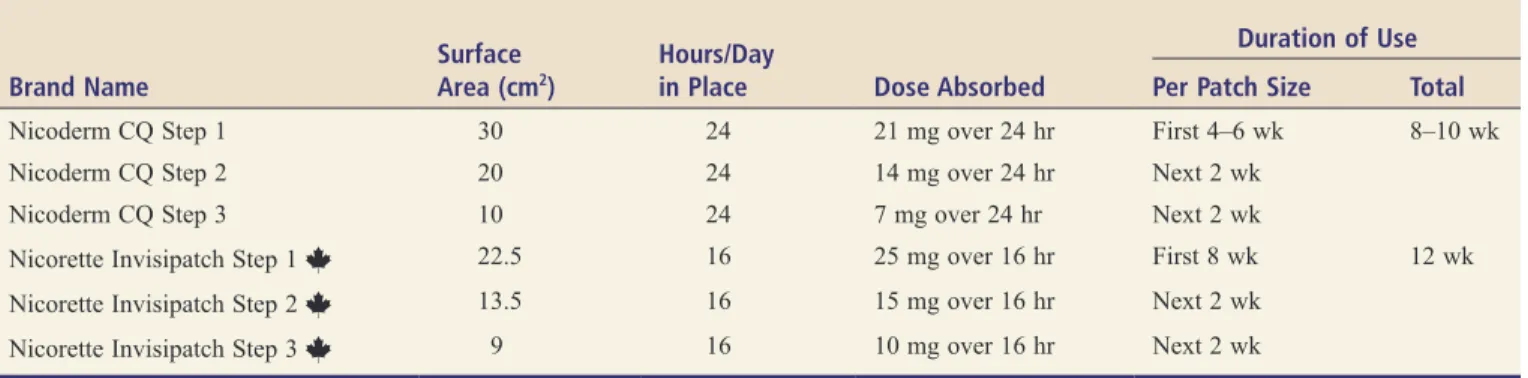
Nicotine-based products—nicotine gum, nicotine lozenges, nicotine patch, nicotine inhaler, and nicotine nasal spray—are used as nicotine replacement therapy (NRT). For additional information on smoking cessation, visit the websites for Canada and the United States listed in Table 39.2.
Nicotine Replacement Therapy
Like nicotine gum and other forms of NRT, nicotine tablets double your quitting success rate. With the nasal spray, nicotine levels in the blood rise quickly, just like when smoking.
Bupropion SR
Still, because the spray delivers nicotine without the added dangers of cigarettes, using a spray is clearly better than smoking.
Varenicline
To reduce nausea, each dose should be taken after a meal and with a full glass of water. However, all patients should be advised to contact their doctor if they experience a significant change in behavior or mental status.
Major Drugs of Abuse Other Than Alcohol and Nicotine
Patterns of Use
HEROIN, OXYCODONE, AND OTHER OPIOIDS
Preferred Drugs and Routes of Administration
Subjective and Behavioral Effects
This can be accomplished by taking a history of the extent of drug use and by observing the patient for withdrawal symptoms. Like methadone, buprenorphine can replace the opioid that a person with OUD is physically dependent on, thereby preventing withdrawal symptoms.
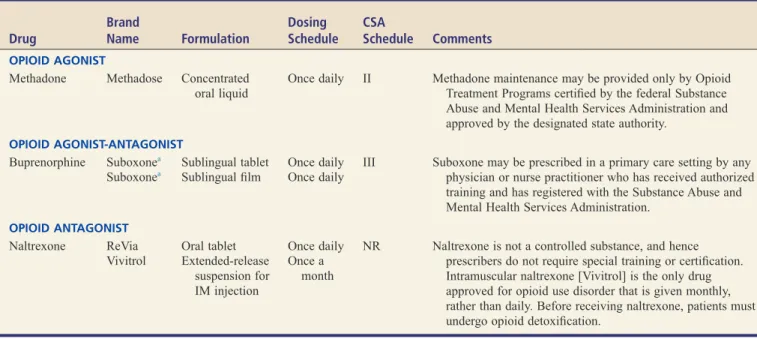
Drugs for Long-Term Management of Opioid Use Disorder
Once the individual is stabilized on buprenorphine, the dose is gradually reduced, thereby keeping withdrawal symptoms to a minimum. When administered to an individual physically dependent on opioids, clonidine may suppress some withdrawal symptoms.
Tolerance and Physical Dependence
Therefore, the extent of physical dependence must be assessed to ensure appropriate methadone dosing. The use of methadone for maintenance and suppression therapy is discussed later in this chapter.
Treatment of Acute Toxicity
When replacing methadone with another opioid, suppression of the withdrawal syndrome requires that the methadone dosage be closely matched to the existing degree of physical dependence. In both procedures, the patient is given an opioid antagonist (naloxone or naltrexone) to expedite immediate withdrawal and thereby speed up the withdrawal process.
Detoxification
Buprenorphine can be used as maintenance therapy and to facilitate detoxification (see earlier section in this chapter). However, sublingual administration is used very little for the long-term treatment of opioid use disorders.
Barbiturates
Benzodiazepines
Sequelae of Compulsive Opioid Use
GENERAL CNS DEPRESSANTS
Although there is no specific antidote for cocaine toxicity, most symptoms can be controlled with medication. If a serious overdose occurs, flumazenil [Romazicon, Anexate], a benzodiazepine antagonist, can reverse the signs and symptoms.
PSYCHOSTIMULANTS
Cocaine
Methamphetamine
Psychoactive Component
Mechanism of Action
Behavioral and Subjective Effects
Synthetic Cathinones
MARIJUANA AND RELATED PREPARATIONS
Pretreatment with propranolol prevents marijuana-induced tachycardia but does not block the subjective effects of the drug. To demonstrate physical dependence on marijuana, the drug must be administered in very high doses – and even then the degree of dependence is only moderate.
Therapeutic Use
In addition, chronic use is closely associated with the development of bronchitis, sinusitis and asthma. Multiple effects can be seen in infants and children exposed to marijuana in utero.
Physiologic Effects
In most of these states, eligible patients must have a debilitating medical condition plus documentation from their doctors that the medical use of marijuana "may be beneficial." Because marijuana is classified by the DEA as a Schedule I substance, doctors still can't prescribe the drug—all they can do is suggest that it might be beneficial.
Comparison of Marijuana With Alcohol
The Supreme Court ruled that the DEA law trumps the new state laws, and therefore people who use or dispense medical marijuana can still be prosecuted under federal law, even in states where medical marijuana has been legalized. Medical use of marijuana has been legal in Canada since 2001, when the Marijuana Medical Access Regulations came into effect.
Synthetic Marijuana
So even though patients may be violating federal law, the Justice Department will not prosecute them. Additionally, several deaths and many episodes of psychosis and toxicity may be related to synthetic marijuana use.
PSYCHEDELICS
The LSD user may feel a sense of wonder and awe at the beauty of everyday things. There can be a sense of overlapping realities and of being in multiple places at once.
Mescaline, Psilocin, Psilocybin, and Dimethyltryptamine
Users may lose consciousness of their own body and of the room they are in. They may feel as if they are floating, traveling through time and space, or merging with or transforming into objects.
DISSOCIATIVE DRUGS
Phencyclidine
Salvia
Physical restraint may be necessary to prevent self-inflicted harm and to protect others from abuse. Elimination of phencyclidine can be accelerated by continuous gastric lavage and by acidifying the urine with ammonium chloride.
Ketamine
Acidification of urine may promote the excretion of phencyclidine by reducing tubular reabsorption of this weak base.
DEXTROMETHORPHAN
By promoting muscle relaxation, dantrolene [Dantrium] can reduce heat generation and the risk of rhabdomyolysis. Treatment consists of rapid cooling, rehydration, and administration of dantrolene [Dantrium], a drug that relaxes skeletal muscle, thereby reducing heat generation and the risk of rhabdomyolysis.
Potential Medical Use
The risk of hyperthermia and dehydration can be greatly reduced by providing adequate fluids at dance parties known as "raves". Because of its amphetamine-like actions, MDMA can increase heart rate, blood pressure, and myocardial oxygen consumption.
INHALANTS
In this study, reductions in ligand binding correlated with the extent of MDMA use and not with the duration of abstinence.
Anesthetics
Volatile Nitrites
Time Course and Dosage
Who Uses MDMA and Why?
Adverse Effects
In addition, these compounds can cause visual hallucinations and disorientation with respect to time and place. For example, chloroform is toxic to the heart, liver and kidneys, and toluene can cause severe brain damage and bone marrow depression.
ANABOLIC STEROIDS
Organic Solvents
When physical dependence on barbiturates (and other CNS depressants) is severe, the associated withdrawal syndrome can be severe—sometimes fatal. Note that this is different from the situation with opioids.). Acute panic reactions to LSD can be managed by "talking it out" and by treatment with benzodiazepines.
VI ELECTROLYTE BALANCE
Physiology
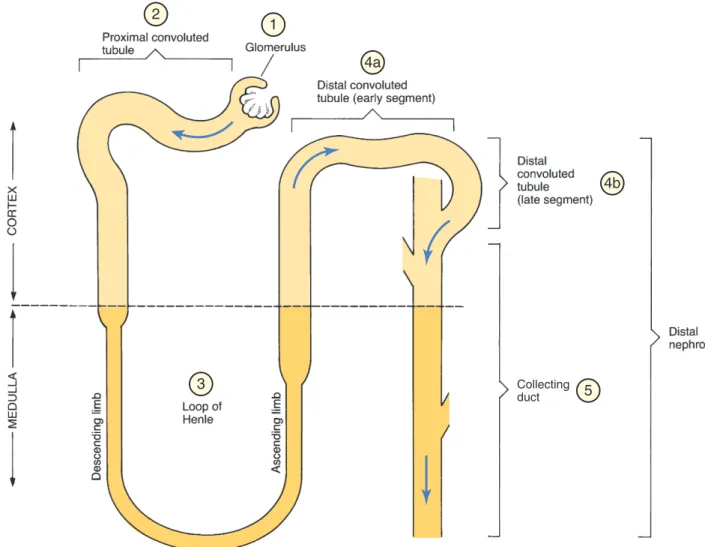
REVIEW OF RENAL ANATOMY AND PHYSIOLOGY
Anatomy
The percentages indicate how much of the filtered sodium and chloride is reabsorbed at each site. Approximately 10% of the filtered sodium and chloride are reabsorbed in the early segment of the distal convoluted tubule.
LOOP DIURETICS
Furosemide
INTRODUCTION TO DIURETICS How Diuretics Work
Adverse Impact on Extracellular Fluid
Classification of Diuretics
Potassium levels should be monitored regularly to reduce the risk of toxicity; potassium supplements or potassium-sparing diuretics should be given when indicated. Patients should be advised of gout symptoms (joint tenderness or swelling) and instructed to notify the prescriber if they occur.
THIAZIDES AND RELATED DIURETICS
Hydrochlorothiazide
In addition to hydrochlorothiazide, five other thiazides (and related agents) are approved for use in the United States (Table 41.2). However, these drugs are very similar to thiazides, both in structure and function, and are therefore included in the group.
POTASSIUM-SPARING DIURETICS
However, these agents are very similar to thiazides in both structure and function, and are therefore included in the group. . abnormal heart rhythm), spironolactone should be discontinued and potassium intake should be limited. Because of the risk of hyperkalemia, caution should be exercised when combining spironolactone with potassium supplements, salt substitutes (containing potassium chloride), or another potassium-sparing diuretic.
Triamterene
As a result, spironolactone can cause a variety of endocrine effects, including gynecomastia, menstrual irregularities, impotence, hirsutism, and deepening of the voice. When administered long-term to rats at doses 25 to 250 times higher than those used in humans, spironolactone caused benign thyroid and testicular adenomas, malignant mammary tumors, and proliferative changes in the liver.
Spironolactone
Potassium-sparing diuretics are used primarily to prevent potassium loss in patients taking loop of Henle diuretics or thiazides. The risk of hearing loss due to loop diuretics increases in the presence of other ototoxic drugs, especially aminoglycosides.
Volume Contraction
DISORDERS OF FLUID VOLUME AND OSMOLALITY
Conversely, by increasing bicarbonate secretion, the kidneys can lower pH and thereby compensate for alkalosis.
Respiratory Alkalosis
Respiratory Acidosis
Metabolic Alkalosis
Volume Expansion
ACID-BASE DISTURBANCES
Hypokalemia
Metabolic Acidosis
POTASSIUM IMBALANCES
Regulation of Potassium Levels
MAGNESIUM IMBALANCES
Hypomagnesemia
Hyperkalemia
Hypermagnesemia
VII VESSELS, AND BLOOD
Components of the Circulatory System
Distribution of Blood
What Makes Blood Flow?
OVERVIEW OF THE CIRCULATORY SYSTEM
How Does Blood Get Back to the Heart?
REGULATION OF CARDIAC OUTPUT
Determinants of Cardiac Output
Afterload is formally defined as the load against which a muscle exerts its force (i.e. the load a muscle must overcome in order to contract). For the heart, afterload is the arterial pressure that the left ventricle must overcome to eject blood.
Starling’s Law of the Heart
Cardiac afterload is mainly determined by the degree of peripheral resistance, which in turn is determined by constriction and dilation of arterioles. That is, when the arterioles contract, peripheral resistance increases, which also increases the AP (afterload).
REGULATION OF ARTERIAL PRESSURE
Overview of Control Systems
Factors That Determine Venous Return
Starling’s Law and Maintenance of Systemic-Pulmonary Balance
Renal Retention of Water
Postural Hypotension
Natriuretic Peptides
Steady-State Control by the ANS
Rapid Control by the ANS: The Baroreceptor Reflex
The Renin-Angiotensin- Aldosterone System
The release of ANP and BNP is caused by stretching of the atria and ventricles, which occurs due to increased preload.). The most important determinant of venous return is systemic filling pressure, which can be increased by narrowing the veins and increasing blood volume.
Angiotensin-Aldosterone System
Types of Angiotensin
Actions of Angiotensin II
PHYSIOLOGY OF THE RENIN-ANGIOTENSIN- ALDOSTERONE SYSTEM
Since renin catalyzes the rate-limiting step in angiotensin II formation, and since renin must be released into the blood to act, factors that regulate renin release regulate the rate of angiotensin II formation. Because ACE is abundant, the conversion of angiotensin I to angiotensin II occurs almost immediately after angiotensin I is formed.

Actions of Aldosterone
Thus, as blood pressure, blood volume, and plasma sodium content increase in response to renin release, further release of renin is suppressed. In this regard, we can consider renin release to be regulated by a classical negative feedback loop.
ANGIOTENSIN-CONVERTING ENZYME INHIBITORS
Regulation of Blood Pressure by the Renin-Angiotensin-
Tissue (Local) Angiotensin II Production
Receptor Blocker Losartan
In patients with less advanced nephropathy (30 to 300 mg proteinuria/day), ACE inhibitors may delay the onset of overt nephropathy. Not surprisingly, ACE inhibitors are contraindicated for patients with bilateral renal artery stenosis (or stenosis in the artery to a single remaining kidney).

RECEPTOR BLOCKERS
An ARB—losartan [Cozaar]—is approved for reducing the risk of stroke in patients with hypertension and LV hypertrophy. An ARB—telmisartan [Micardis]—is approved for reducing the risk of MI, stroke, and death from cardiovascular causes in patients age 55 and older, but only if they are intolerant to ACE inhibitors.
ALISKIREN, A DIRECT RENIN INHIBITOR
As with Tekturna, each daily dose must be taken at the same time in relation to meals. As with Tekturna and Tekturna HCT, each daily dose must be taken at the same time with meals.
ALDOSTERONE ANTAGONISTS
Eplerenone
ACE inhibitors may cause a sharp drop in blood pressure in patients with bilateral renal artery stenosis (or stenosis in the artery of one remaining kidney). ACE inhibitors are contraindicated during the second and third trimesters of pregnancy and in patients with (1) bilateral renal artery stenosis (or stenosis in the artery of one remaining kidney) or (2) a history of hypersensitivity reactions (especially angioedema). on ACE. inhibitors.
RECEPTOR BLOCKERS Azilsartan
Closely monitor infants who have been exposed to ACE inhibitors during the second or third trimester for hypotension, oliguria, and hyperkalemia. Use caution in patients receiving potassium supplements, salt substitutes, potassium-sparing diuretics, or ACE inhibitors.
Heart
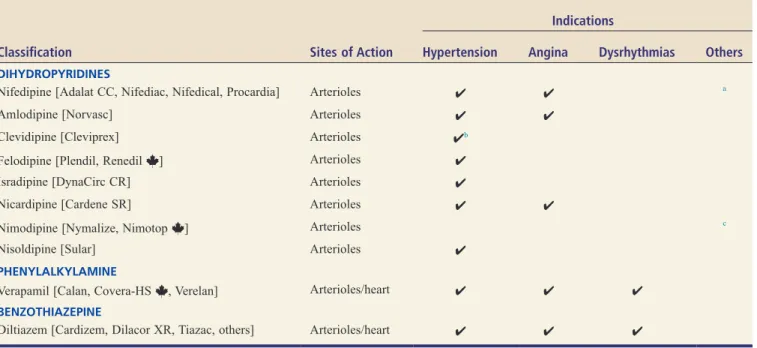
CALCIUM CHANNEL BLOCKERS
CLASSIFICATION AND SITES OF ACTION Classification
CALCIUM CHANNELS: PHYSIOLOGIC FUNCTIONS AND CONSEQUENCES
Vascular Smooth Muscle
The differences in selectivity between CCBs are based on structural differences between the drugs themselves and structural differences between calcium channels.
VERAPAMIL AND DILTIAZEM: AGENTS THAT ACT ON VASCULAR SMOOTH
Verapamil
Sites of Action
In the SA node, blockade of calcium channels can cause bradycardia; in the AV node, blockage can cause partial or complete AV block; and in the direct effects. Like verapamil, diltiazem (Cardizem, Dilacor XR, Tiazac, others) blocks calcium channels in the heart and blood vessels.
DIHYDROPYRIDINES: AGENTS THAT ACT MAINLY ON VASCULAR
Conversely, with the SR formulation, blood levels of nifedipine rise slowly, causing blood pressure to fall slowly and the reflex to be blunted. Please note, however, that the reflex increase in heart rate and contractile force is transient and occurs primarily with the IR formulation.
SMOOTH MUSCLE
Nifedipine
In toxic doses, nifedipine and other dihydropyridines can cause cardiosuppression, as can verapamil and diltiazem. Verapamil and diltiazem are indicated for hypertension, angina pectoris and cardiac arrhythmias (atrial fibrillation, atrial flutter and paroxysmal supraventricular tachycardia).
Overview of Therapeutic Uses
Adverse Effects Related to Vasodilation
BASIC CONCEPTS IN VASODILATOR PHARMACOLOGY
Selectivity of Vasodilatory Effects
The increase in volume represents an attempt by the body to return blood pressure to pre-treatment levels. Aldosterone then acts on the kidneys to promote sodium and water retention, thereby increasing blood volume.
PHARMACOLOGY OF INDIVIDUAL VASODILATORS
Prolonged use of arteriolar or venous dilators may cause an increase in blood volume (secondary to prolonged lowering of blood pressure). Second, by reducing arterial pressure, vasodilators decrease renal blood flow and glomerular filtration rate; because the filtrate volume decreases, the kidney is able to reabsorb an increased portion of the filtered sodium and water, which causes the blood volume to expand.
Hydralazine
To help prevent vasodilator-induced reflex tachycardia, patients can be pretreated with a beta-blocker (eg, metoprolol), which will block sympathetic stimulation of the heart. For example, if the volume is increased during the treatment of hypertension, the blood pressure will increase and the benefits of the therapy will be nullified.
Minoxidil
Daily doses greater than 200 mg are associated with an increased incidence of adverse effects and should be avoided. Nitroprusside is approved for producing controlled hypotension during surgery (to reduce bleeding in the surgical field) and for acute decompensated heart failure.
Sodium Nitroprusside
By adjusting the infusion rate, blood pressure can be reduced to almost any desired level. Drugs that dilate arterioles or veins can cause fluid retention, which can be blunted with a diuretic.
BASIC CONSIDERATIONS IN HYPERTENSION
CLASSIFICATION OF BLOOD PRESSURE
In people aged 40 to 70, the risk of cardiovascular disease doubles for every 20 mm Hg increase in SBP or every 10 mm Hg increase in DBP—starting at 115/75 mm Hg and continuing up to 185/155 mm Hg. Because the injury develops slowly and progressively, and because hypertension rarely causes concern, many people who have the disease do not know it.
MANAGEMENT OF CHRONIC HYPERTENSION
The degree of injury is directly related to the level of elevated pressure: the higher the pressure, the greater the risk. In addition, many people who know it refuse treatment anyway, mainly because they don't feel bad about their hypertension - that is, until it's too late.
BASIC CONSIDERATIONS Diagnosis
Benefits of Lowering Blood Pressure
TYPES OF HYPERTENSION
Primary (Essential) Hypertension
Secondary Hypertension
CONSEQUENCES OF HYPERTENSION
Treatment Goals
Therapeutic Interventions
LIFESTYLE MODIFICATIONS
Sodium Restriction
The DASH Eating Plan
Patient Evaluation
DRUG THERAPY
Alcohol Restriction
Aerobic Exercise
Smoking Cessation
Weight Loss
Maintenance of Potassium and Calcium Intake
Review of Blood Pressure Control
In addition to causing vasoconstriction, angiotensin II causes the release of aldosterone from the adrenal cortex. Third, we can prevent the conversion of angiotensin I to angiotensin II with an ACE inhibitor.
Antihypertensive Mechanisms: Sites of Drug Action and Effects Produced
Baroreceptors in the aortic arch and carotid sinus sense BP and relay this information to the brainstem
The RAAS increases blood pressure, beginning with the release of renin from juxtaglomerular cells of the kidney. Constriction of the renal blood vessels increases blood pressure by decreasing glomerular filtration, which causes salt and water retention, which in turn increases blood volume and blood pressure.
When BP is perceived as too low, the brainstem sends impulses along sympathetic nerves to stimulate the heart
Next, angiotensin converting enzyme (ACE) acts on angiotensin I to form angiotensin II, a compound that constricts systemic and renal blood vessels. As discussed in Chapter 43, the kidneys play a central role in the long-term regulation of blood pressure.
When BP has been restored to an acceptable level, sympathetic stimulation of the heart and vascular smooth
Therefore, blockade results in peripheral vasodilation, renal vasodilation, and suppression of aldosterone-mediated volume expansion. Blockade of aldosterone receptors in the kidneys promotes sodium and water excretion and therefore reduces blood volume.
Classes of Antihypertensive Drugs
Reserpine – the only available adrenergic neuron blocker – depletes norepinephrine from postganglionic sympathetic nerve endings, reducing sympathetic stimulation of the heart and blood vessels. If you are confused about spironolactone, yes, it is the same drug we previously discussed under potassium-sparing diuretics.
Fundamentals of Hypertension Drug Therapy
In patients with advanced renal insufficiency, thiazide diuretics are ineffective; therefore, a loop diuretic should be used. In patients with diabetic nephropathy, ACE inhibitors and ARBs may slow the progression of kidney damage and reduce albuminuria.
Individualizing Therapy
For each drug in the regimen, the dose should be low at first and then gradually increased. Nevertheless, beta blockers and ACE inhibitors should be used Regardless, it seems clear that ACE inhibitors are better than.
Promoting Adherence
High starting doses and rapid dose escalation may increase the incidence and severity of adverse effects. Therefore, large initial doses should be avoided, which can cause a rapid drop in blood pressure, but also cause adverse effects.
Minimizing Adverse Effects
DRUGS FOR HYPERTENSIVE EMERGENCIES
ACOG defines severe hypertension as SBP above 160 mm Hg or DBP above 110 mm Hg and mild hypertension as SBP 140 to 159 mm Hg or DBP 90 to 109 mm Hg.).
PREECLAMPSIA AND ECLAMPSIA
ACOG defines severe hypertension as SBP above 160 mm Hg or DBP above 110 mm Hg, and mild hypertension as SBP 140 to 159 mm Hg or DBP 90 to 109 mm Hg.) There is good evidence that treating severe hypertension reduces risk.
DRUGS FOR HYPERTENSIVE DISORDERS OF PREGNANCY
CHRONIC HYPERTENSION
Loop diuretics should be reserved for (1) patients who require greater diuresis than can be achieved with thiazides and (2) patients with low GFR (because thiazides are ineffective when GFR is low). These changes should be tried for 6 to 12 months before drug therapy is implemented, and continued even if medications are necessary.
PATHOPHYSIOLOGY OF HEART FAILURE
First, decreased cardiac output causes a reduction in renal blood flow, which in turn decreases glomerular filtration rate (GFR). In addition, angiotensin II causes constriction of systemic arterioles and arteries, thereby increasing venous and arterial pressure.
Cardiac Remodeling
Physiologic Adaptations to Reduced Cardiac Output
Classification of Heart Failure Severity
The Vicious Cycle of “Compensatory”
Physiologic Responses
Signs and Symptoms of Heart Failure
Unlike the thiazides and loop diuretics, the potassium-sparing diuretics (eg, spironolactone, triamterene) promote little diuresis. Because angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor blockers (ARBs) also carry a risk of hyperkalemia, caution is necessary if these drugs are combined with a potassium-sparing diuretic.
Drugs That Inhibit the RAAS
Consequently, when treatment with an ACE inhibitor or ARB is initiated, the potassium-sparing diuretic should be discontinued. A potassium-sparing diuretic - spironolactone - prolongs survival in patients with HF primarily by blocking receptors for aldosterone, not by causing diuresis.
OVERVIEW OF DRUGS USED TO TREAT HEART FAILURE
Unlike thiazides, these drugs can promote fluid loss even when GFR is low. Like the thiazides, these drugs can cause hypokalemia, increasing the risk of digoxin toxicity.
Diuretics
In addition, these drugs can cause kidney failure in patients with bilateral renal artery stenosis. Because of their ability to elevate potassium levels, ACE inhibitors should be used with caution in patients taking potassium supplements or a potassium-sparing diuretic (eg, spironolactone, triamterene).
Receptor Blockers
The main adverse effects of ACE inhibitors are hypotension (secondary to arteriolar dilation), hyperkalemia (secondary to decreased aldosterone release), intractable cough, and angioedema. In theory, their benefits in HF should be equal to those of ACE inhibitors and ARBs.
Beta Blockers
As discussed in Chapter 8, testing was limited largely because of regulatory and market incentives, not because there was evidence to suggest that it would not work for others. The effects have been described as equivalent to "pharmacological phlebotomy". In HF, nitroglycerin is used to relieve acute severe pulmonary edema.
Ivabradine (Corlanor)
In patients with severe refractory HF, the drug may reduce congestive symptoms and improve exercise capacity. Among patients with HF, the main side effects are (1) fluid retention and worsening of HF, (2) fatigue, (3) hypotension, and (4) bradycardia or heart block.
Inotropic Agents
Thereby, the drug can increase myocardial contractility and can thereby improve cardiac performance. The region of the molecule consisting of the steroid core plus the lactone ring (ie, the region without the sugar molecules) is responsible for the pharmacological effects of digoxin.
Mechanical Effects on the Heart
When used for heart failure, digoxin can reduce symptoms, increase exercise tolerance, and reduce hospitalizations. Because the benefits are limited to symptomatic relief and because the risk of toxicity is high, digoxin is now considered a second-line drug for the treatment of HF.
DIGOXIN, A CARDIAC GLYCOSIDE
Following the action potential, the Na+/K+-ATPase pumps Na+ out of the cell and takes in K+. By inhibiting the Na+/K+-ATPase, digoxin prevents Na+ efflux, causing Na+ to accumulate within the cell.
ATTENTION: DIGOXIN MAY BE HAZARDOUS TO WOMEN’S HEALTH
Neurohormonal Benefits in Heart Failure
Electrical Effects on the Heart
Hemodynamic Benefits in Heart Failure
If the potassium level is low or near normal, potassium (IV or PO) should be administered. However, if potassium levels are high or if AV block is present, no more potassium should be given.
Adverse Effects II: Noncardiac Adverse Effects
Since heart disease is the reason for taking digoxin, it should come as no surprise that people taking the drug are at risk for dysrhythmias. The possibility that the dysrhythmia is a direct result of heart disease should be considered.
Adverse Effects I: Cardiac Dysrhythmias
Cholestyramine and activated charcoal, agents that also bind digoxin, can be administered orally to suppress the absorption of digoxin from the gastrointestinal tract. In the past, there was considerable variation in the absorption of digoxin from tablets prepared by different manufacturers.
Adverse Effects III: Measures to Reduce Adverse Effects
In addition, verapamil may inhibit myocardial contractility, thus negating the benefits of digoxin. The term digitization refers to the use of a loading dose to rapidly achieve high digoxin plasma levels.
MANAGEMENT OF HEART FAILURE
Rather, this information should be viewed as only one factor among several to be considered when evaluating clinical responses. Intramuscular administration should be avoided because of the risk of tissue damage and severe pain.
Stage A
If the heart rate is less than 60 beats/min or if a change in rhythm is detected, digoxin should be withheld and the prescribing physician notified. For patients who cannot tolerate ACE inhibitors (due to intractable cough or angioedema), ARBs remain the recommended alternative.
Stage B
Digoxin can be used in combination with ACE inhibitors (or ARBs), diuretics and beta blockers to improve clinical status. For patients who cannot tolerate ACE inhibitors or ARBs, substitution of ISDN/hydralazine is considered reasonable.
Stage C
Antidysrhythmic agents - These drugs have cardiosuppressive and prodysrhythmic effects that can worsen HF. In addition, NSAIDs can reduce the effectiveness and intensify the toxicity of diuretics and ACE inhibitors.
Stage D
By doing so, they may increase the risk of hyperkalemia in patients taking ACE inhibitors or ARBs. In patients with HF, ARBs should be reserved for patients who are intolerant to ACE inhibitors (usually due to cough).
Potassium Channel Blockers (Drugs That Delay Repolarization), p. 551
Potassium Channel Blockers (Drugs That Delay Repolarization), p. 559
CARDIAC ELECTROPHYSIOLOGY, DYSRHYTHMIAS, AND THE
The function of these fibers is to conduct electrical excitation very quickly to all parts of the ventricles. Because impulses travel rapidly through this system, all regions of the ventricles are stimulated almost simultaneously, causing synchronized ventricular contraction with the resulting forceful ejection of blood.
Cardiac Action Potentials
Impulses originating in the atria must travel through the AV node to reach the ventricles. These impulses are rapidly conducted down the bundle of His, enter the right and left bundle branches, and then disperse into many fine branches of Purkinje fibers (see Fig. 49.1).
ELECTRICAL PROPERTIES OF THE HEART
In the healthy heart, impulses arriving at the AV node are slowed down before proceeding to stimulate the ventricles.
Impulse Conduction: Pathways and Timing
The PR interval is defined as the time between the onset of the P wave and the onset of the QRS complex. The QT interval is defined as the time between the start of the QRS complex and completion of the T wave.

GENERATION OF DYSRHYTHMIAS
In addition to the features just described, the ECG has three other components of interest: the PR interval, the QT interval, and the ST segment. The ST segment is the part of the ECG that lies between the end of the QRS complex and the beginning of the T wave.
Disturbances of Automaticity
The Electrocardiogram
In a re-entrant circuit (Fig. 49.4B) there is a region of unidirectional conduction block of one branch of the Purkinje fiber. First, drugs can improve conduction in the diseased branch of the Purkinje fiber and thereby eliminate the unidirectional block (Fig. 49.4C).
CLASSIFICATION OF
The impulses that move towards each other meet midway between the two branches of the Purkinje fiber. This stimulation causes an impulse to travel backwards up the blocked branch of the Purkinje fiber.
ANTIDYSRHYTHMIC DRUGS
In normal impulse conduction, electrical impulses travel down both branches of the Purkinje fiber to cause muscle excitation at two sites (Fig. 49.4A). However, in this new situation, as the impulse travels toward the damaged branch of the Purkinje fiber, it does not meet any impulse coming from the other direction and continues, resulting in stimulation of the terminal end of the first (blocked) branch.
Sodium Channel Blockers
This area prevents the conduction of impulses downward (to the muscle), but does not prevent impulses from going upward. Impulses can travel back through the block because impulses in the muscles are very strong and can therefore pass through the block, while impulses in the Purkinje fiber are weaker and so cannot pass.) An area of one-way block is essential for reactivation. As an impulse flows through the Purkinje fiber, it is blocked in one branch but continues unhindered in the other branch.
Beta Blockers
As described earlier, the impulse in the muscle moves to the right and to the left, away from the place of origin. Alternatively, drugs can suppress conduction in the diseased branch, converting a unidirectional block into a bidirectional block (Fig. 49.4D).
Disturbances of Conduction
Since the muscle in the wake of both impulses is in a refractory state, neither impulse can proceed, so both impulses stop. Since blockade of conduction in that branch is one way (downward only), the impulse can pass upward through the region of the block and then back down the unblocked branch, causing reentrant activation of that branch.
PRODYSRHYTHMIC EFFECTS OF ANTIDYSRHYTHMIC DRUGS
Potassium Channel Blockers (Drugs That Delay Repolarization)
Calcium Channel Blockers
Other Antidysrhythmic Drugs
Supraventricular Dysrhythmias
OVERVIEW OF COMMON
DYSRHYTHMIAS AND THEIR TREATMENT
If there are no additional signs of heart disease, PVCs are benign and are usually not treated. However, in the event of acute myocardial infarction, PVCs may predispose the patient to ventricular fibrillation.
PRINCIPLES OF ANTIDYSRHYTHMIC DRUG THERAPY
Digoxin causes dysrhythmias by increasing automaticity in the atria, ventricles, and His-Purkinje system, and by decreasing conduction through the AV node. The main factor associated with the development of torsades de pointes is prolongation of the QT interval, which can be caused by a variety of drugs, including class IA and class III antidysrhythmic agents.
Balancing Risks and Benefits
Torsades de pointes is an atypical, rapid, undulating ventricular tachycardia dysrhythmia that can progress to potentially fatal ventricular fibrillation.
Ventricular Dysrhythmias
Long-Term Treatment: Drug Selection and Evaluation
Minimizing Risks
PHARMACOLOGY OF THE ANTIDYSRHYTHMIC DRUGS
SODIUM CHANNEL BLOCKERS
Class IA Agents
Phases of Treatment
Quinidine PO widens QRS, prolongs QT Broad spectrum: used for long-term suppression of ventricular and supraventricular dysrhythmias. Sotalol PO, IV Prolongs QT and PR, bradycardia Life-threatening ventricular dysrhythmias, atrial fibrillation/flutter.
Drugs That Delay Repolarization
Amiodarone PO, IV Prolongs QT and PR, widens QRS Life-threatening ventricular dysrhythmias, atrial fibrillationa Dronedarone PO Prolongs QT and PR, widens QRS Atrial flutter, atrial fibrillation. Digoxin PO, IV Prolongs PR, Suppresses ST Control of ventricular rate in patients with supraventricular tachydysrhythmias.
Calcium Channel Blockers
Lidocaine has three major effects on the heart: (1) like other class I drugs, lidocaine blocks the sodium channels of the heart, thereby slowing conduction in the atria, ventricles, and His-Purkinje system. 2) the drug reduces automaticity in the ventricles and the His-Purkinje system by a mechanism that is poorly understood;. In addition, complete blood counts should be obtained promptly at the first sign of infection, bruising, or bleeding.

Class IB Agents
Therefore, the drug should be used with caution in patients with heart failure, AV block or asthma. Due to its pro-arrhythmic action, propafenone is reserved for patients who have not responded to safer drugs.
BETA BLOCKERS
For the immediate-release tablets, the dose is initially 150 mg every 8 hours, and can be gradually increased to 300 mg every 8 hours. For the extended-release capsules, the dose is initially 225 mg every 12 hours; this can be gradually increased to 425 mg every 12 hours.
Propranolol
Due to its cardiac and pulmonary effects, propranolol should be used with caution in patients with asthma, and is contraindicated in patients with sinus bradycardia, high-grade heart block and HF. Accordingly, acebutolol should be used with caution in patients with asthma, and is contraindicated in patients with HF, severe bradycardia and AV block.
POTASSIUM CHANNEL BLOCKERS (DRUGS THAT DELAY
In the United States, oral amiodarone is only approved for long-term treatment of two life-threatening ventricular dysrhythmias: recurrent ventricular fibrillation and recurrent hemodynamically unstable ventricular tachycardia.
Amiodarone
In contrast to oral amiodarone, which affects several aspects of cardiac function, IV amiodarone primarily affects the AV node. However, maintenance infusions can be continued for up to 3 weeks before switching to oral amiodarone.
Dronedarone
Drugs and dietary supplements that prolong the QT interval (eg phenothiazines, tricyclic antidepressants, class I and class III antidysrhythmics) may intensify dronedarone-induced QT prolongation and may thereby increase the risk of torsades de pointes. Therefore, the drug should not be used in patients with a QT interval greater than 500 msec or in patients taking medications or supplements that cause QT prolongation.
CALCIUM CHANNEL BLOCKERS
If the arrhythmia does not change within 10 minutes of stopping the infusion, another 1-mg infusion may be attempted.
OTHER ANTIDYSRHYTHMIC DRUGS Adenosine
The QT interval represents the time between the beginning of the QRS complex and the end of the T wave. Widening of the QRS complex (by 50% or more) and excessive prolongation of the QT interval are warning signs.
CHOLESTEROL
In contrast, all lipoproteins that transport lipids from nonhepatic tissues back to the liver (ie, that remove lipids from tissues) contain apolipoproteins A-I.
Classes of Lipoproteins
PLASMA LIPOPROTEINS
Structure and Function of Lipoproteins
Conversely, because HDL appears to protect against atherosclerosis, it is often called good cholesterol or healthy cholesterol.
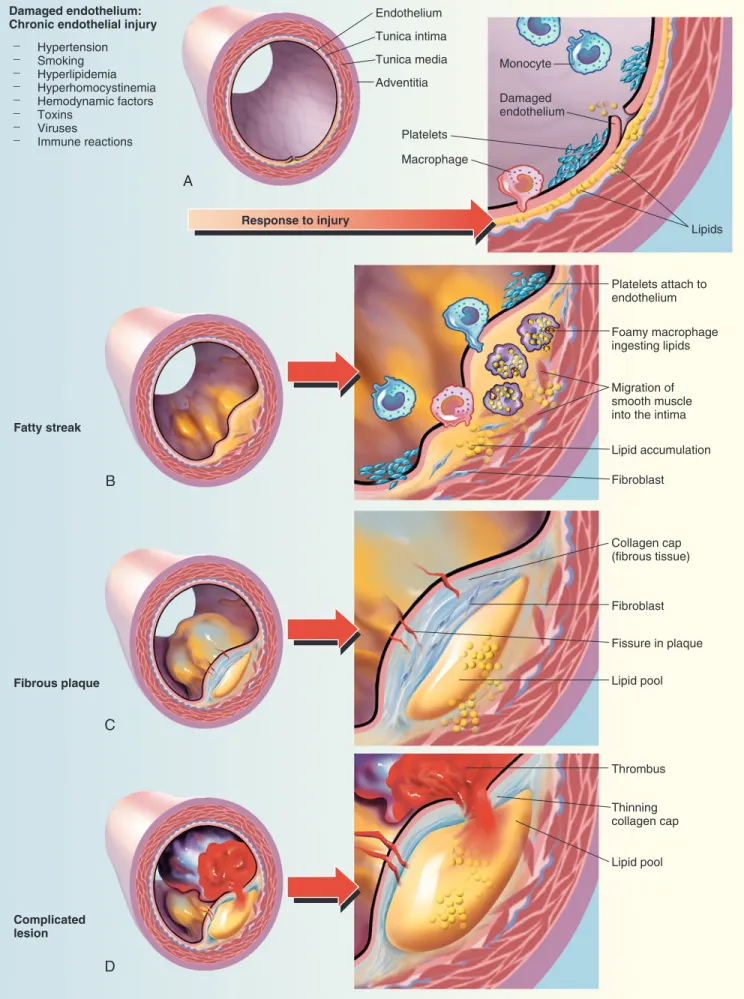
ROLE OF LDL CHOLESTEROL IN ATHEROSCLEROSIS
LDL Cholesterol Versus HDL Cholesterol
2013 ACC/AHA GUIDELINES ON THE TREATMENT OF BLOOD CHOLESTEROL
CARDIOVASCULAR RISK
Cholesterol Screening
Identifying an individual's ASCVD risk category According to the 2013 ACC/AHA cholesterol guideline, there are four categories of patients who would benefit from statin therapy for cholesterol (see Table 50.2). Final note: Each type of dyslipidemia that a patient has independently contributes to ASCVD risk. Patients likely have more than one type of dyslipidemia—.
Treatment of High LDL Cholesterol
An ASCVD risk equivalent is a condition that carries the same risk of a major coronary event as established ASCVD does (ie, greater than 20% risk of a major event within 10 years). Category assignment is based on (1) the presence or absence of ASCVD (or an ASCVD risk equivalent, such as diabetes), (2) the number of risk factors the individual has (other than high LDL cholesterol), and (3) the individual's 10-year ASCVD score.
ASCVD Risk Assessment
Cigarette smoking raises LDL cholesterol and lowers HDL cholesterol, thereby increasing the risk of ASCVD. Drugs, on the other hand, should only be used if TLCs cannot reduce LDL cholesterol to an acceptable level - and only if the combination of elevated LDL cholesterol and the patient's ASCVD risk category justifies drug use.

Secondary Treatment Targets
Although the term metabolic syndrome is widely used, there is debate about its clinical relevance. Consequently, until there is more evidence that the metabolic syndrome actually exists, they believe that the term serves no clinical purpose and should therefore be avoided.
HMG-CoA Reductase Inhibitors (Statins)
DRUGS AND OTHER PRODUCTS USED TO IMPROVE PLASMA LIPID LEVELS
In patients with evidence of existing ASCVD (angina pectoris or previous MI), statins reduce the risk of death from cardiac causes. The study found that rosuvastatin can reduce the risk of coronary events in people with normal LDL levels but high CRP levels and other ASCVD risk factors.

A Word Regarding Niacin (Nicotinic Acid)
Six statins—lovastatin, pravastatin, atorvastatin, fluvastatin, rosuvastatin, and simvastatin—are now available as generic products, and are therefore cheaper than all other statins.
Bile-Acid Sequestrants
The older active substances - cholestyramine and cholestipol - can reduce the absorption of fats and thereby reduce the intake of fat-soluble vitamins. Although cholestyramine and cholestipol are very safe, they often cause constipation, abdominal discomfort, and flatulence.
Ezetimibe
Cholestyramine and colestipol have been available for decades, but have largely been replaced by colesevelam because colesevelam is better tolerated, does not interfere with absorption of fat-soluble vitamins, and has minimal effects on other drugs. The dose for the granules is 5 to 30 gm/day administered in one or more doses.
Fibric Acid Derivatives (Fibrates)
However, there is no evidence that combining the drug with a statin reduces the risk of a serious CV event. Fenofibric acid is available in delayed-release capsules (45 and 135 mg, sold as TriLipix; 35 and 105 mg, sold as Fibricor).
Monoclonal Antibodies (Proprotein Convertase Subtilisin/Kexin Type 9
In patients with mild to moderate renal impairment, a low dose (45 mg/day) should be used. Regular exercise can reduce LDL cholesterol and raise HDL cholesterol, reducing the risk of ASCVD.
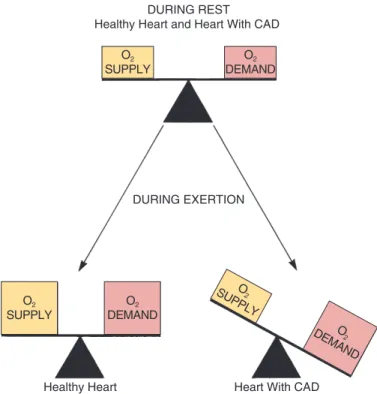
DETERMINANTS OF CARDIAC OXYGEN DEMAND AND OXYGEN SUPPLY
Oxygen Demand
Oxygen Supply
ANGINA PECTORIS: PATHOPHYSIOLOGY AND TREATMENT STRATEGY
Chronic Stable Angina (Exertional Angina)
In the healthy heart, as the heart's oxygen demand increases, the coronary arteries dilate, increasing blood flow. 51.1 ■ Effect of exercise on the balance between oxygen supply and oxygen demand in the healthy heart and the heart with CAD.
ORGANIC NITRATES
An angiotensin-converting enzyme inhibitor - for patients with left ventricular dysfunction or congestive heart failure. Eptifibatide [Integrilin] or tirofiban [Aggrastat] (both are glycoprotein IIb/IIIa inhibitors) - but only in high-risk patients with ongoing ischemia, and only if angioplasty is not planned.
Variant Angina (Prinzmetal’s Angina, Vasospastic Angina)
Angiotensin receptor blockers are a reasonable alternative in patients who are intolerant to angiotensin-converting enzyme inhibitors. Anticoagulant therapy consists of subcutaneous low-molecular-weight heparin (eg, enoxaparin [Lovenox]), direct thrombin inhibitors (bivalirudin [Angiomax]), factor Xa inhibitors (fondaparinux [Arixtra]), or IV unfractionated heparin.
Unstable Angina
Nitroglycerin
To end an acute angina attack, sublingual nitroglycerin should be administered as soon as pain begins. To reduce the risk of tolerance, these products should only be taken once or twice a day.

BETA BLOCKERS
Accordingly, when the use of ranolazine plus a CCB is indicated, amlodipine is the only CCB that should be used. Ranolazine [Ranexa] is formulated in extended-release tablets (500 and 1000 mg) that are to be swallowed intact, with or without food.
TREATMENT MEASURES
Drugs that prolong the QT interval (eg, quinidine, sotalol) may increase the risk of torsades de pointes in patients taking ranolazine and should be avoided. Ranolazine may be used in combination with a nitrate, beta blocker or amlodipine (CCB) and other angina medications.
Guidelines for Management of Chronic Stable Angina
RANOLAZINE
Systemic hypertension Beta-blockers (long-acting slow-release CCBs) Migraine or vascular headache Beta-blockers (verapamil or diltiazem). Mild peripheral vascular disease Beta blockers or long-acting slow-release CCBs Severe peripheral vascular disease s.
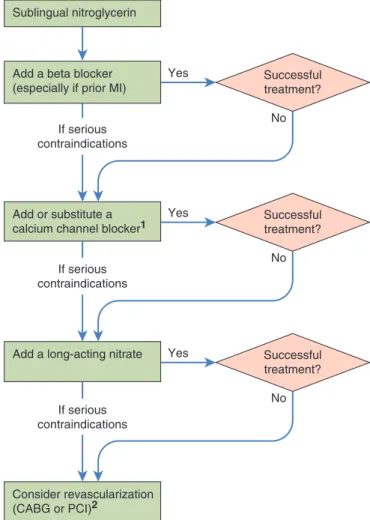
Management of Variant Angina
Instruct patients to call 911 or go to an emergency department if pain is not relieved within 5 minutes. Sustained protection against angina attacks. patients to remove any remaining ointment before administering a new dose.