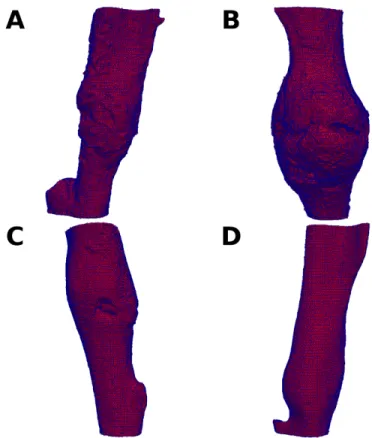
Transplanted MSC express BMP-2 in the fracture and localize to the endosteal site of the callus. Fracture healing is a postnatal repair process that recapitulates aspects of the embryonic development of the skeleton. MicroCT analysis of fracture callus relies on three-dimensional reconstruction of the serial microCT axial images.
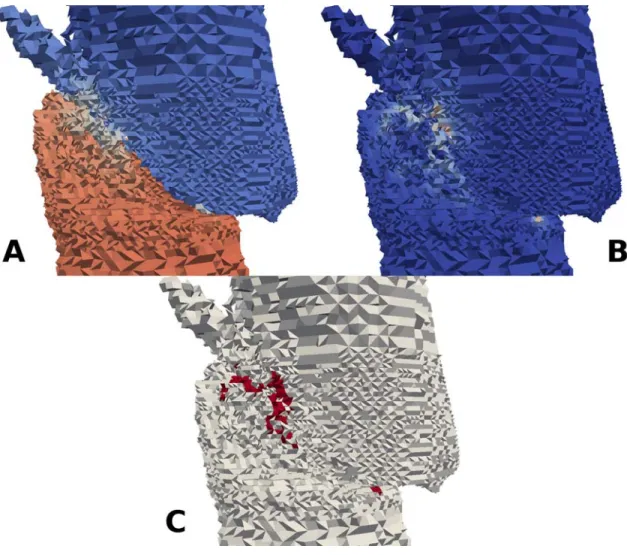
However, due to the atypical and inhomogeneous nature of the fracture callus, as seen in Figure 2, such machining and homogenization is incorrect. The rest of the surface nodes are assigned as stress-free (Neumann boundary conditions or Type II). Assessment of the recovery of load-bearing function is the central goal in the study of the healing process of fractures.
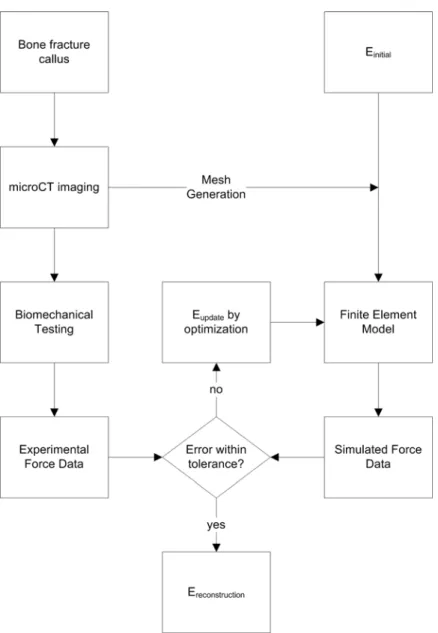
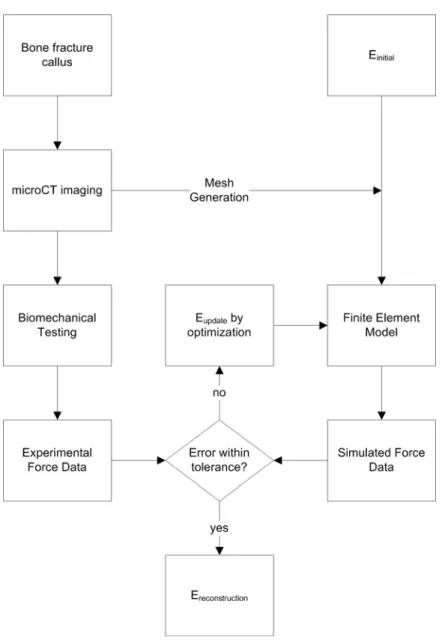
Under equal displacement conditions, inverse process estimates of callus material properties are generated and compared to other fracture healing metrics. An inverse FEA procedure was developed to determine callus stiffness based on microCT imaging and BMT data. This suggests that transducer noise plays little role in the overall method error.
However, due to the atypical and inhomogeneous nature of fracture callus, such processing and homogenization is inappropriate.

MicroCT Metrics
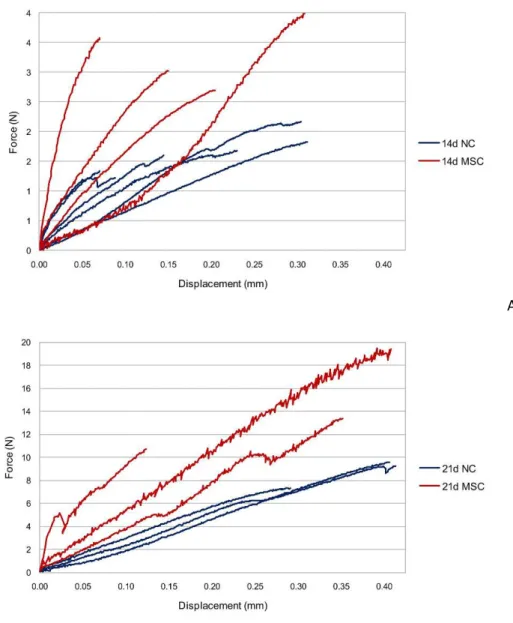
Post-test pairwise statistical comparisons are shown only for the bold comparisons from Table 5. Data from biomechanical testing (force versus displacement) of NC and MSC at 14 and 21 days post-fracture are shown in Figure 22. A large variation in the curves is observed both among and among all test groups, representing a wide range of extrinsic biomechanical properties.
A quantitative analysis of the biomechanical testing metrics of ultimate load, toughness, and apparent stiffness was generated for these samples, and the results are shown in Table 7 and Figure 23. Statistical comparisons and associated p-values are reported as a composite with all other measurements in Table 8. According to large differences between biomechanical testing data, a statistically significant increase in apparent stiffness was observed only in wild-type mice from early to late stages of healing.
These data show that extrinsic whole-bone BMT measures are improved longitudinally from 14 to 21 days after fracture and that MSC transplantation improves only a few of. However, without accounting for the geometric changes induced by time and MSC treatment on calluses, it is impossible to separate the improvement in whole-bone BMT behavior from either geometric morphological changes or tissue-level mechanical improvement. Post-test pairwise statistical comparisons are shown only for comparisons listed in bold from Table 5.
Post-test pairwise statistical comparisons are shown only for comparisons listed in bold from Table 5.
BMT and Inverse FEA Metrics
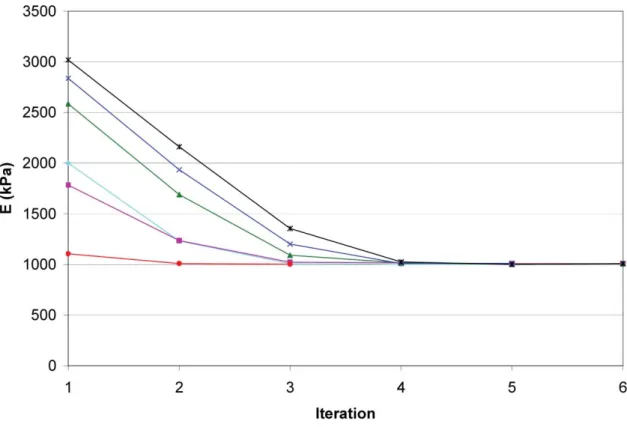
Inverse FEA generated reconstructions of material properties were performed as described to generate estimates for the Young's modulus of the callus material. However, in the GNL approach, each step provides new information about the geometric relationship of the callus constituents. In previous work, the approach was reported using a linear Hookean elastic model of the callus [86].
In this case, the solution of the second problem does not need to be constituted, because it represents only a scaling of the first (in this case, only multiplying the first solution by a scale factor of 2 is sufficient). The result returned is the mechanical properties of the bone fracture callus, which serves as a biomarker for fracture healing. The underlying CRM architecture is a client-server relationship in which the client communicates with the server to provide computing services to the user.
On the server side, the CRM is designed to (a) manage requests from the clients, (b) invoke the computation routines, (c) allocate computation resources, and (d) monitor the status of the computation routines. After completing all steps, the user is presented with the reconstructed elastic modulus of the fracture callus tissue, which represents a biomarker for bone fracture healing. Force versus displacement curves for (A) callus hyperelastic and linear elastic material FEA model comparisons, and (B) experimental biomechanical testing of the same sample.
Validation of the inclusion of a commercial FE package within the inverse procedure is shown in Table 12. As the callus is the weakest part of the bone specimen, failure will predictably occur within the callus region. Although not statistically significant (due to low sample numbers and an inherently noisy genetic system), this observation seems to fit within the logic of the experimental system.
The utility of the inverse analysis methodology presented in this work is in the improved functional assessment of fracture callus tissue. This study demonstrates the details of the fracture healing animal model as well as details regarding the MSC transplantation system. MSC were also isolated from the BM of the CMV-R26R or BMP-2-Lac-Z mice and.
Tibia fractures were dissected 14 days after fracture and after removal of the pin and microCT scanned (Scanco Medical µCT40). Paraffin sections (6 um thick sections), of the Beta-gal stained callus were subjected to in situ hybridization for Osteocalcin. Within the woven bone, some of the Lac-z positive MSC (blue staining cells) are double stained for osteocalcin (brown staining) as indicated by arrows.
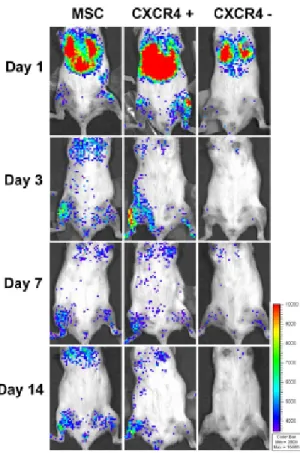
To determine the contribution of MSC to the initial phase of callus formation, we analyzed whether transplanted MSC were able to express BMP-2 in the callus.


![Figure 7. Predicted and experimental torsional rigidity of rat femur. Adapted from [46]](https://thumb-ap.123doks.com/thumbv2/123dok/10730319.0/32.918.313.713.629.971/figure-predicted-experimental-torsional-rigidity-rat-femur-adapted.webp)