Pediatric nutrition in practice / volume editor, Berthold Koletzko ; co-editors, Jatinder Bhatia, Zulfiqar A. Bhutta, Peter Cooper, Maria Makrides, S.A. World Review of Nutrition and Dietetics; vol. 113). The statements, opinions and data in this publication are solely those of the individual authors and contributors and not of the publisher and editors.
List of Contributors
Department of Neonatology Institute of Child Health Sir Ganga Ram Hospital New Delhi 110060 (India) E-Mail [email protected] Sanja Kolaček. South Australian Medical and Health Research Institute Women's and Children's Health Research Institute 72 King William Road.
Preface
Child Growth
There is evidence that a high protein intake during the first years of life is associated with an increased risk of developing overweight and obesity later in life [8, 9]. This is a valuable tool for surveillance, monitoring trends of undernutrition and overweight and obesity in the population.
![Fig. 1. The infancy-childhood-puberty growth model by Karlberg [1] .](https://thumb-ap.123doks.com/thumbv2/123dok/10720884.0/18.807.432.734.86.466/fig-1-infancy-childhood-puberty-growth-model-karlberg.webp)
Nutritional Assessment
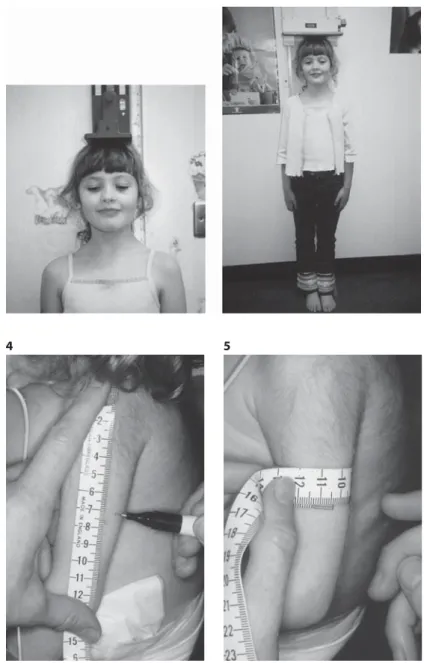
- Clinical Evaluation and Anthropometry
- Diet History and Dietary Intake Assessment
- Use of Technical Measurements in Nutritional Assessment
- Use of Laboratory Measurements in Nutritional Assessment
Weight for height compares a child's weight with the average weight of children of the same height, i.e. it is important to involve the child and parents or guardians at all stages of the process.

Nutritional Needs
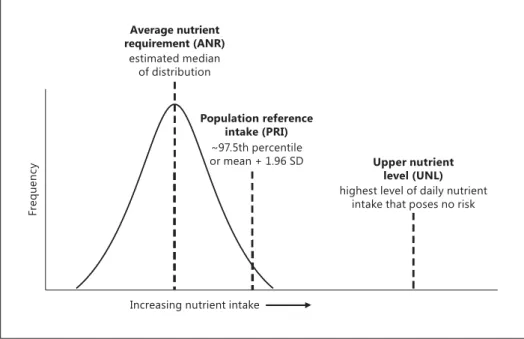
- Nutrient Intake Values: Concepts and Applications
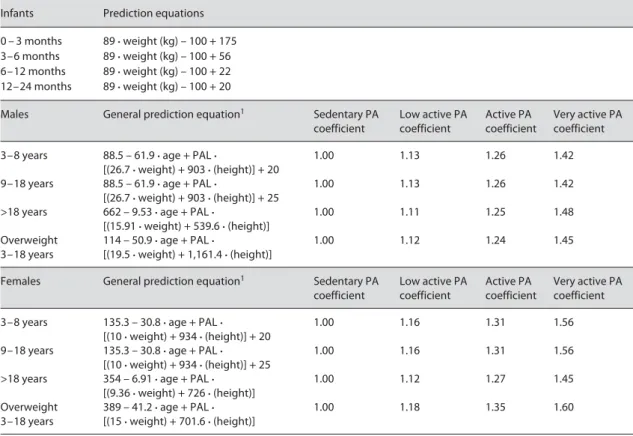
- Energy Requirements of Infants, Children and Adolescents
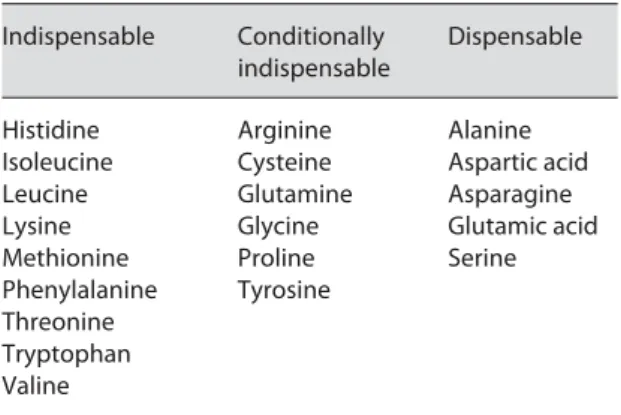
- Protein
- Digestible and Non-Digestible Carbohydrates
- Fats
- Fluid and Electrolytes
- Vitamins and Trace Elements
The derivation of the NIV from observed nutrient intakes (e.g. the nutrient supply provided by breast milk) or extrapolation from other age groups has significant limitations. Regardless of the etiology, more than 90% of dehydration can be treated safely and. eds): Pediatric nutrition in practice.
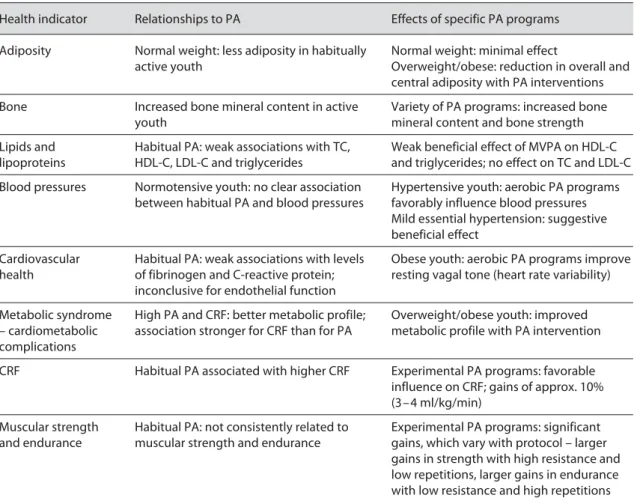
Physical Activity, Health and Nutrition
An important issue is the prevention of unhealthy weight gain in early childhood and the possible role of PA. The beneficial effects of PA are more visible among 'unhealthy' young people - on adipose tissue in youth. eds): Child nutrition in practice. A key issue is the prevention of unhealthy weight gain in early childhood and the potential role of PA [14].
Early Nutrition and Long-Term Health
Metabolic programming of long-term health · Developmental origins of adult health · Breastfeeding and obesity · Perinatal nutrition · Prevention of disease risks. Nutritional and metabolic factors during sensitive, limited periods of early human development have a long-term programming effect on health, well-being, and performance in later life, extending into adulthood and old age. The concept of early metabolic programming of long-term health is supported by physiological, epidemiological and clinical research [1–3].

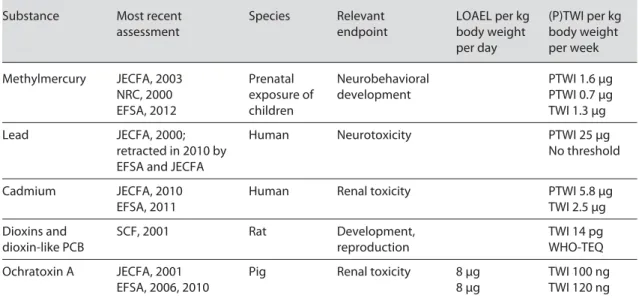
Food Safety
By dividing the NOAEL by the actual consumer exposure, the safety margin can be estimated. A typical example of the importance of HACCP principles in food production and of sanitary measures to be applied by consumers is the case of Enterobacter sakazakii (Cronobacter spp.) in powdered infant formula. The microbial safety of food is the responsibility of the manufacturer as well as the person preparing and serving it.
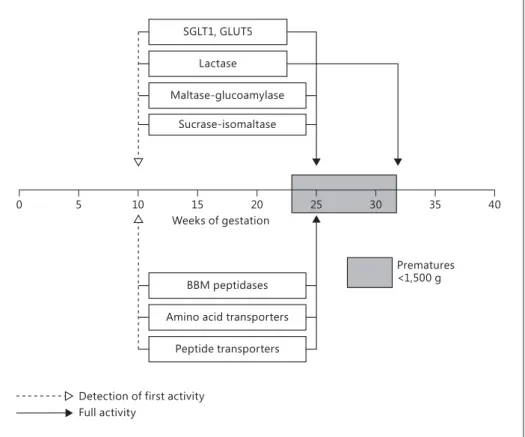
Gastrointestinal Development, Nutrient Digestion and Absorption
The development of the gastrointestinal tract during intrauterine life is a prerequisite for survival in the external life of a human fetus. As the number of premature babies under 1000 grams is increasing, knowledge of the digestive and absorptive functions of the gastrointestinal tract is crucial. In parallel with the morphological changes during fetal development, the digestive and absorptive functions of the gastrointestinal tract begin.
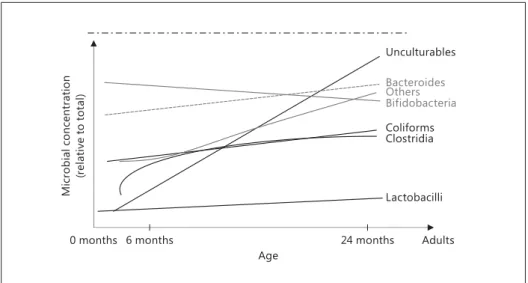
Gut Microbiota in Infants
An early change of the microbiota to the adult type may be associated with the development of eczema [9]. Compositional abnormalities are associated with multiple disease states. promoting the bifidogenic environment via prebiotic galacto-oligosaccharides and microbes in breast milk and introducing environmental bacteria through contact with the infant. • Both the sequence of microbial communities. during the first years of life and the consequences of these events need to be elucidated in more detail. • The first colonization steps play a crucial role. in the child's microbiota and later health. Bifidobacteria play a key role in this process. • Mother-child contact plays an important role. impact on the initial development of the microbiota, with the critical first inoculum being provided before birth, followed by another inoculum at parturition, and then progressing during lactation. • The possible use of specific probiotics. and/or prebiotics to influence microbiota development for the treatment and prevention of diseases also warrants further evaluation.
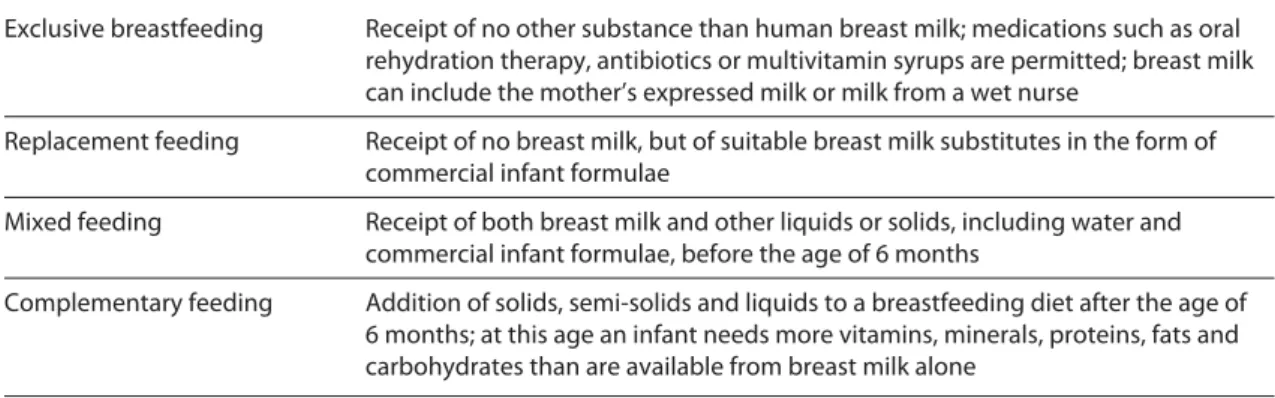
Breastfeeding
These non-nutrients are involved in many of the short- and long-term effects that breastfeeding has on the baby. In high-income countries, the risk of diarrhea in breastfed infants is only about one third of the risk in non-breastfed infants [2]. Traditional hospital routines with separation of the mother and the baby, scheduled feeding intervals and provision of other drinks have a negative impact on the prevalence of breastfeeding.

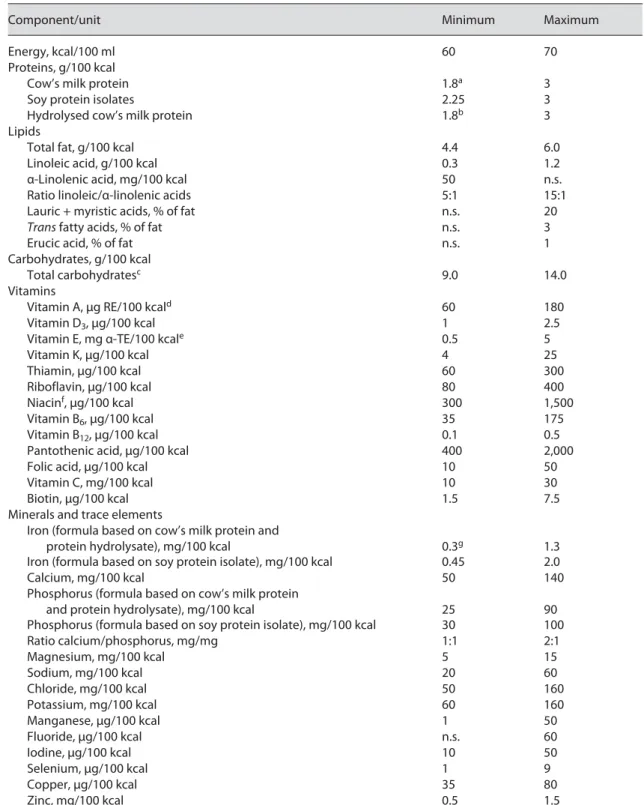
Formula Feeding
Infant formula is required as a substitute for breast milk for infants who are not fully breastfed • Infant formula must meet all nutritional needs. The composition of infant formulas should follow current science-based recommendations • Special infant formula such as soy protein-. base and thickened formulas should be used according to specific indications. 5 Codex Alimentarius Commission: Standard for infant formula and formulas for special medical purposes intended for infants.
Marketing of Breast Milk Substitutes
It is now recognized that voluntary initiatives alone are not sufficient to implement the International Code of Marketing of Breast-milk Substitutes. The International Code of Marketing of Breast-milk Substitutes must be monitored and implemented in all countries. 6 Taylor A: Violations of the International Code of Marketing of Breast-milk Substitutes: Prevalence in Four Countries.
Complementary Foods
However, since many infants receive human milk substitutes from the first weeks of life, other authorities have suggested that the term 'complementary foods'. They should not be introduced before 17 weeks of age, but all babies should start complementary foods at 26 weeks of age. Complementary foods should not be introduced before 17 weeks of age, but all babies should start complementary foods at 26 weeks of age.
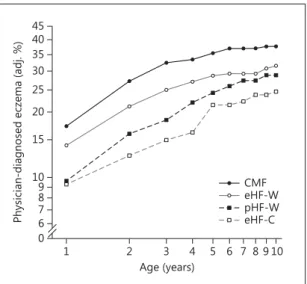
Allergy Prevention through Early Nutrition
In infants with a positive family history of allergy who are not exclusively breastfed, the use of infant formulas based on hydrolysed cow's milk proteins reduces the risk of atopic eczema. However, there is some evidence that the mother's consumption of fatty fish during pregnancy and breastfeeding reduces the risk of allergic diseases in the offspring [3]. Very early introduction of solid food within the first 3 months of life seems to increase the risk of eczema and possibly also of food allergy.
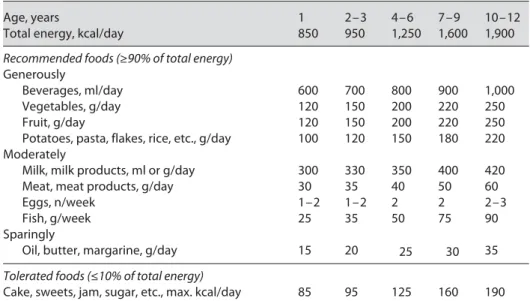
Toddlers, Preschool and School Children
A healthy diet for children should be created on the basis of scientific and practical considerations. The amounts shown in table 1 should not be consumed every day; the goal should be the average amount consumed per week. Fish is an important source of iodine and long-chain n-3 fatty acids and should be eaten at least once a week.
Adolescent Nutrition
School-based nutrition education interventions to prevent and reduce childhood and adolescent obesity are effective in reducing rates of overweight and obesity and in increasing fruit and vegetable consumption [ 12 , 13 ]. The effect of aerobic exercise on non-high-density lipoprotein cholesterol in children and adolescents has not yet been established. Parental participation in weight-related health interventions for children and adolescents: a systematic review and meta-analysis.
Nutrition in Pregnancy and Lactation
Vitamin B12 deficiency during pregnancy and lactation can cause megaloblastic anemia and neurological defects in Some caffeine is transferred to the fetus through the placenta and to the infant through breast milk. Alcohol is transferred to the fetus through the placenta and to the baby through breast milk.
![Table 1. The 2009 Institute of Medicine gestational weight gain recommendations for singleton and twin pregnan- pregnan-cies [2]](https://thumb-ap.123doks.com/thumbv2/123dok/10720884.0/144.807.99.737.127.350/table-institute-medicine-gestational-recommendations-singleton-pregnan-pregnan.webp)
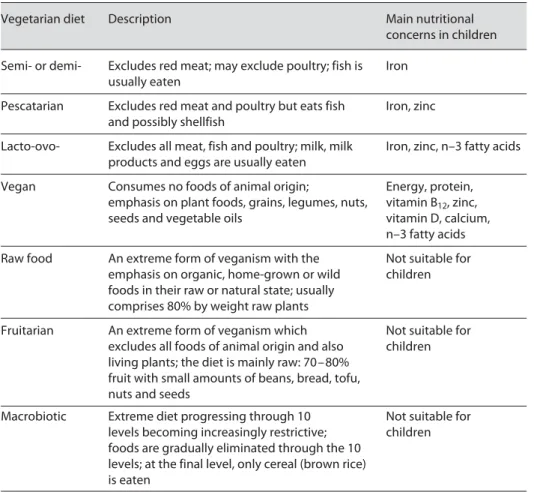
Vegetarian Diets
Carefully planned mixed vegetarian diets (with milk and eggs) can provide sufficient energy, protein and nutrients for all stages of childhood growth and development. Very restrictive or unbalanced vegetarian diets can result in failure to thrive and serious nutrient deficiencies in infants and children. The main sources of zinc in vegetarian diets include whole grains and cereals, which are also high in phytates and reduce the bioavailability of zinc [10].
Primary and Secondary Malnutrition
Water-soluble forms of the usually fat-soluble vitamins (A, D, E and K) should be used when available. Secondary malnutrition is more common in developed countries and is difficult to treat without addressing the underlying causes. • Secondary malnutrition should be managed in. the Life Course and Malnutrition - Area Acute Malnutrition. eds): Pediatric nutrition in practice.

Micronutrient Deficiencies in Children
Zinc supplementation in children aged 1 to 4 years is associated with a reduction in all-cause mortality of approximately 9 to 18%. 14 Imdad A, Herzer K, Mayo-Wilson E, Yakoob MY, Bhutta ZA: Vitamin A supplementation for the prevention of morbidity and mortality in children aged 6 months to 5 years. 18 Imdad A, Bhutta ZA: Effect of preventive zinc supplementation on linear growth in children under 5 years of age in developing countries: a meta-analysis of studies for input into the life-saving tool.
![Table 1. Global deaths attributed to micronutrient deficiencies as well as disability-adjusted life years (DALYs) of children <5 years of age [23]](https://thumb-ap.123doks.com/thumbv2/123dok/10720884.0/164.807.204.734.126.252/table-global-attributed-micronutrient-deficiencies-disability-adjusted-children.webp)
Enteral Nutritional Support
The following should be taken into account when choosing a formula: (a) nutrient and energy requirements adjusted to the patient's age and clinical condition; (b) history of food intolerance or allergy; (c) level of bowel function; (d) the place and route of delivery of the formula; (e) formula characteristics such as osmolality, viscosity and nutrient density; (f) preferred taste; and (g) costs. Placement in the stomach is confirmed by measuring the pH of the aspirate, which in children should be <4 in. Patients receiving PN should be assessed 2 to 3 times per week (eg, clinical examination, weight, anthropometry, laboratory values, and dietary intake as appropriate).

Parenteral Nutritional Support
This should be avoided whenever possible by the use of adequate care, specialized enteral nutrition (EN) and artifi-. In premature infants, the glucose intake should start at 4–8 mg/kg per minute (5.8–11.5 g/kg per day) and gradually increase. In critically ill children, the glucose intake should be ≤ 5 mg/kg per minute (7.2 g/kg per day).
Management of Child and Adolescent Obesity
For preadolescent children, weight outcomes can be improved with a parent-focused intervention without direct involvement of the child [9]. Examples of the former include not buying cookies or reducing TV time to 3 hours a day. Diarrhea remains one of the leading causes of mortality among children under 5 • Risk factors for diarrhea include those related to.
Reducing the Burden of Acute and Prolonged Childhood Diarrhea
Probiotics 14% reduction in duration of diarrhea, 11% reduction in stool frequency on day 2 and 19% reduction in hospital admissions, although not statistically significant. Therapeutic zinc. 66% reduction in diarrhea-specific mortality, 23% reduction in diarrheal hospitalizations, and 19% reduction in diarrheal prevalence Antiemetics for gastroenteritis 54% reduction in the incidence of vomiting and hospitalizations and 60%. reducing the need for intravenous fluid. intervention-based interventions 153% increase in ORS use and manifold increase in zinc use for diarrhea; 76% reduction in antibiotic use for diarrhea.

HIV and AIDS
The focus of nutrition activity has shifted from supporting malnourished HIV-infected infants and children to ensuring that ART-infected children are adequately nourished. There are no evidence-based guidelines for the appropriate prescription of micronutrient supplements for HIV-infected children. A focus on the growth and nutrition of the HIV-infected child at each visit is warranted.
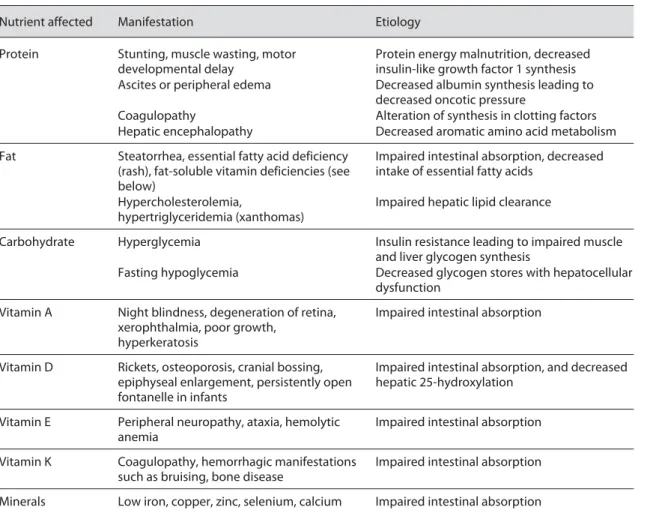
Nutritional Management in Cholestatic Liver Disease
The most common types of cholestatic liver disease in children include extrahepatic biliary atresia, Alagille syndrome, α1-antitrypsin deficiency, cystic fibrosis, and liver disease associated with intestinal failure. On the other hand, decreased glycogen stores and reduced glucose production in all types of end-stage liver disease can result in fasting hypoglycemia. It may also contribute to the prevention of cholestasis and liver disease • Gut microbiota has both positive (short-chain fatty acid production) and deleterious (intraluminal bacterial growth) effects.
Malabsorptive Disorders and Short Bowel Syndrome
Use of the gastrointestinal (GI) tract as early and as often as clinically tolerated should be promoted and feeding aversions prevented. Adaptation—the physical and physiological processes by which the intestine compensates for loss of intestinal length or function—is optimized by providing OF or EF. Utilization of the gastrointestinal (GI) tract is vital for maintaining or restoring normal intestinal structure and function [3].
![Fig. 4. Reference charts (percentiles) for subscapular skinfold (boy) and BMI. Modified after Tanner and Whitehouse [14] and Nysom et al](https://thumb-ap.123doks.com/thumbv2/123dok/10720884.0/19.807.76.712.100.490/reference-charts-percentiles-subscapular-skinfold-modified-tanner-whitehouse.webp)



![Table 3. Energy requirements of girls during the first year of life 2002 Institute of Medicine [15] 2004 FAO/WHO/UNU [1]](https://thumb-ap.123doks.com/thumbv2/123dok/10720884.0/52.807.205.732.445.707/table-energy-requirements-girls-year-life-institute-medicine.webp)
![Table 2. Energy requirements of boys during the first year of life 2002 Institute of Medicine [15] 2004 FAO/WHO/UNU [1]](https://thumb-ap.123doks.com/thumbv2/123dok/10720884.0/52.807.205.732.109.376/table-energy-requirements-boys-year-life-institute-medicine.webp)