While blood pressure control reduces morbidity and mortality in hypertensive patients, in a subset of patients, conventional antihypertensive therapy does not adequately control blood pressure. An estimated 69% of patients with hypertension have uncontrolled blood pressure despite the use of antihypertensive drugs, according to the National Health and Nutrition Examination Survey 1999 to 2000.4 Some of these patients with uncontrolled blood pressure have resistant hypertension (RH), defined as persistently elevated blood pressure blood pressure despite simultaneous use of three antihypertensive drugs, including a thiazide diuretic. 5.
Racial Differences in Hypertension
In general, AA carries an increased risk of mortality and studies of racial differences in mortality rates suggest that much of the difference can be explained by hypertension.33 In a follow-up study of EA and AA hypertensive patients, the population-attributable 30-year risk of mortality due to hypertension was 23.8% and 18.3% in EA men and women compared to 45.2% and 39.5% in AAs, respectively.34 Furthermore, AA hypertensives ' an increased risk of stroke, congestive heart failure, and CKD compared to EA hypertensives.35-41. While AA has an increased risk of developing many hypertension-related diseases, there are some conditions that occur at lower rates in AA than EA.
Antihypertensive Therapies for Blood Pressure Control
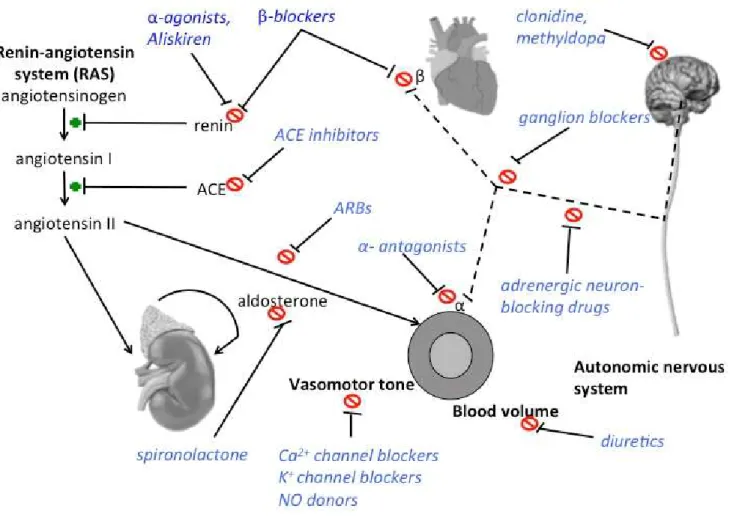
Disproportionate levels of hypertension in AA may explain some of the racial disparities in mortality and hypertension-related disease risk. The first step of the RAAS, the conversion of angiotensinogen to angiotensin I, can be blocked by renin inhibition.
The Cytochrome P450 Hydroxylase Pathway and Blood Pressure Regulation
In the thick ascending limb of the loop of Henle (Henle's Loop), 20-HETE inhibits the Na+-K+-2Cl- co-transporter as well as the Na+-K+ ATPase. In the distal convoluted tubule, 20-HETE inhibits Na+-K+ ATPase, and thiazide diuretics inhibit the Na+-Cl- cotransporter (NCC).

Genetic Variants of CYP4A11 are associated with hypertension and an attenuated
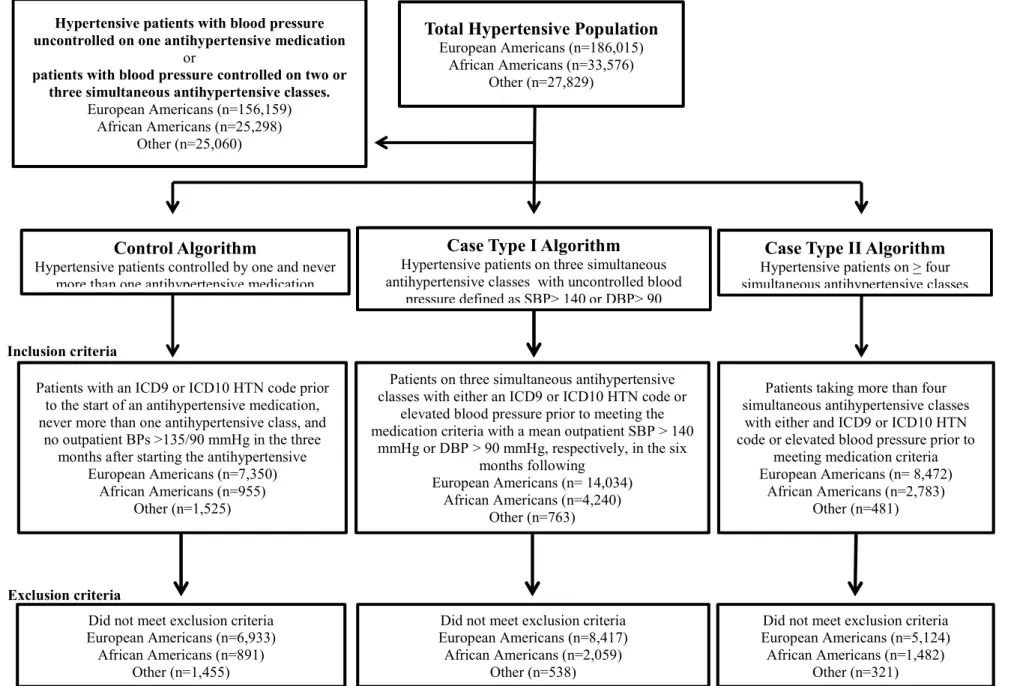
We will discuss this process in terms of identifying patients with resistant hypertension in Chapter 2. To identify patients with resistant hypertension (cases) and patients with controlled hypertension (controls) at VUMC SD, we developed the following, updated algorithms and modified from a previously published algorithm to define resistant hypertension within the Electronic Medical Records & GEnomics (eMERGE) network. 105, 120. Blood pressure and medication use in patients with resistant hypertension with uncontrolled blood pressure describes three medications antihypertensives (case I) and patients with resistant hypertension are prescribed four or more antihypertensive medications (case type II).
Characteristics of European American and African American patients with resistant hypertension (cases) or easily controlled hypertension (controls). Medication use in European-American and African-American patients with resistant hypertension (cases) and easily controlled hypertension (controls). Demographics of European American and African American patients with resistant hypertension stratified by case type.
Using electronic algorithms, patients with resistant hypertension (cases) and patients with controlled hypertension (controls) were identified from 510,167 veterans enrolled in the VA MVP using electronic health records (EHR).117 These algorithms were modified by a.

The Identification of a Clinical Resistant Hypertension Patient Population Using
Vanderbilt University Medical Center’s Electronic Medical Records and DNA
These differences may reflect recent changes in clinical practice that are largely absent in the larger EMR, e.g. We discuss some of these clinical differences in patients identified in VUMC BioVU compared to the larger EMR associated with the RH phenotype in more detail in Chapter 4.
Dissertation Overview
Medication use in European and African American patients with resistant hypertension by case type definition. Urinary sodium excretion predicts blood pressure response to spironolactone in patients with resistant hypertension independent of aldosterone status.
CHARACTERISTICS AND TREATMENT OF AFRICAN AMERICAN AND
Introduction
In the development of the method we observed differences in the prescription patterns of antihypertensive drugs between AA and EA patients with resistant hypertension. We describe here the characteristics and drug treatment of AA versus EA patients with resistant hypertension at VUMC.
Methods
Case type I identified patients with elevated blood pressure despite concurrent treatment with at least three different classes of antihypertensive medications, including a thiazide diuretic, amlodipine, or another DHP CCB (Figure 6). Concomitant treatment with three different classes of antihypertensive drugs was confirmed twice by documentation in the EHR more than a month apart.
Results
DBP and SBP were significantly higher in Case Type I patients than Case Type II patients (Table 6) in both racial groups. 37.4% of EA and 41.2% of AA Case Type II patients were eventually prescribed an aldosterone antagonist.
Discussion
This unexpected finding may be due to the exclusion of a higher proportion of AA with resistant hypertension for fourth and fifth stage KLB compared to EA. Importantly, we found that prescribing trends differ between EA and AA patients with resistant hypertension. Whether differences in drug treatment patterns in AA and EA patients with resistant hypertension reflect adjusted prescribing or prescribing bias requires further study.
Conclusions
Nevertheless, in summary, we demonstrate the feasibility of identifying a large number of patients with resistant hypertension and controlled hypertension using an EHR. Using the methodology, we replicated findings previously reported in population studies and identified distinct patterns of antihypertensive drug use in AA and EA with resistant hypertension.
Figures
Patients on three concurrent antihypertensive classes with either an ICD9 or ICD10 HTN code or. Antihypertensive drug groups are as follows: ACEi, angiotensin-converting enzyme inhibitors; ARB, angiotensin receptor blockers; BB, beta blockers; CCB, calcium channel blockers, including both the dihydropyridine and nondihydropyridine classes; Diuretics, includes non-thiazide class diuretics such as K-sparing and loop diuretics; HCTZ, includes thiazide diuretics, such as hydrochlorothiazide, and thiazide-like diuretics. The percentage of Case Type II patients prescribed four, five, or six simultaneous antihypertensive drug classes at diagnosis based on race.
Tables
Both CYP4A11 variants, rs1126742 and rs3890011, were significantly associated with resistant hypertension in the meta-analyzed total population (Table 10). Low-dose spironolactone reduces blood pressure in patients with resistant hypertension and diabetes mellitus type 2: a double-blind, randomized clinical trial. Ambulatory blood pressure monitoring and clinical features of true and white coat resistant hypertension.

ASSOCIATION OF CYP4A11 LOSS-OF-FUNCTION VARIANTS AND RESISTANT
Introduction
Inhibitors of 20-HETE formation cause salt sensitivity in normotensive rats, while administration of clofibrate to induce CYP4A expression in Dahl salt-sensitive/JR rats can prevent salt-sensitive increases in BP.170-172 Furthermore, the CYP4A2 genotypes segregate together with salt-sensitive hypertension in the F2 cross of Dahl salt-sensitive rats and normotensive Lewis rats.173. Depending on the location of expression in the renal nephron, 20-HETE may increase or decrease blood pressure. In humans, 20-HETE is formed primarily by CYP450 enzymes encoded by the CYP4A11 and CYP4F2 genes.
Methods
Resistant hypertensive cases were defined as patients with blood pressure equal to or greater than 140/90 mmHg despite concomitant use of three antihypertensive agents, including a thiazide diuretic, or if the patient was prescribed four or more concomitant antihypertensive agents, including a thiazide, regardless of blood pressure. The controlled hypertension comparison group included patients with blood pressure controlled to a systolic level of less than 135 mmHg or a diastolic level of less than 90 mmHg, who were prescribed one or two antihypertensive medications. All subjects were genotyped using a modified version of the Affymetrix Axiom Biobank Array and genotypes rs1126742 and rs3890011 were attributed to the 1000 Genomes reference panel.
Results
These strata were then meta-analysed using METAL.182 All regression-based analyzes were performed in SNPTEST v2.5.4-beta.183. In cases and controls combined, the minor allele frequency for the loss-of-function C allele of rs1126742 was 14% in EA and 31% in AA, consistent with previously published frequencies in hypertensive populations.79, 82 Consistent with previously reported frequencies , the frequency of the C allele of rs3890011 was 22% in EA and 57% in AA.86, 184. The increased frequency of the CYP4A11 variants in AA, as well as an association between black race and resistant hypertension make race a genetic analysis stratified by race significant.
Discussion
We detected an association between the loss-of-function C allele of rs1126742 and resistant hypertension in the general population and in AA, but not in EA. In conclusion, our work supports a relationship between CYP4A11 loss-of-function variants and resistant hypertension. It also suggests that future work to better understand the role of salt-sensitive BPs in patients with resistant hypertension and to evaluate the relationship between 20-HETE and salt sensitivity in patients with resistant hypertension is warranted.
Conclusions
Another limitation of this study is the use of control subjects who required more than one antihypertensive drug to achieve adequate BP control. Without long-term follow-up of the identified controls to rule out more advanced hypertension later in life, including the possibility that a subset of the controls may eventually become cases, we cannot ensure a completely homogeneous control population. Finally, our CYP4A11 variants were not directly genotyped using the Affymetrix Array platform and the imputation results were not independently validated.
Tables
Spironolactone is not the only MR antagonist available to lower BP in patients with resistant hypertension. Systematic review and meta-analysis of the prevalence of resistant hypertension in treated hypertensive populations. Abstract p147: Differences in the treatment of resistant hypertension in African Americans and European Americans in a clinical setting.

DETERMINING THE BLOOD PRESSURE RESPONSE TO SPIRONOLACTONE IN
Introduction
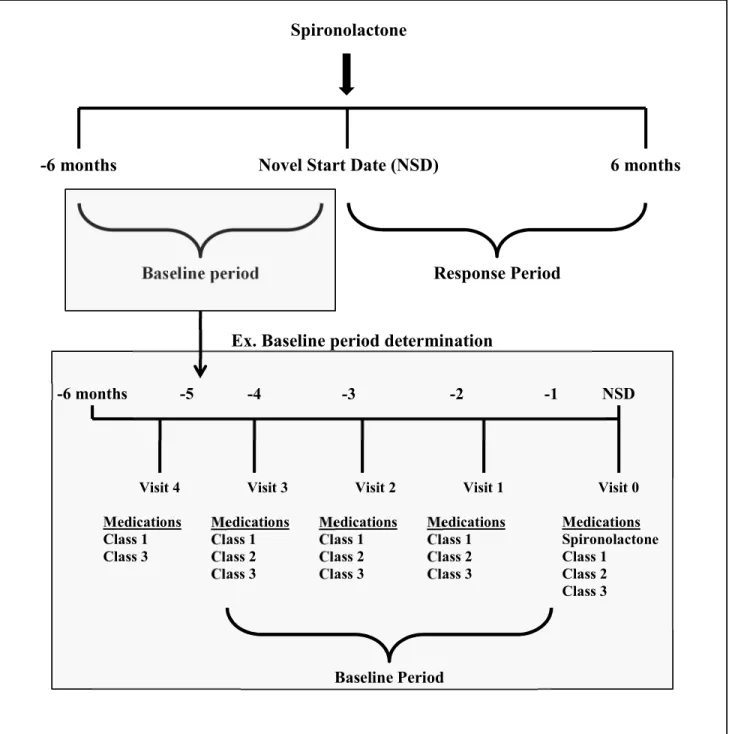
We hypothesized that we could use the electronic medical record (EMR) to assess the blood pressure response to the addition of spironolactone in resistant hypertensive patients who were on a stable antihypertensive regimen with at least three medications, including a thiazide diuretic or CCB. To evaluate blood pressure response to spironolactone, we developed an algorithm to identify patients prescribed spironolactone during a period of stable medication use, from six months before the start of spironolactone treatment to six months afterward. We assessed blood pressure response as a continuous variable and as a dichotomized variable (responders versus non-responders) and built a predictive model that included electrolyte measurements relevant to the mechanism of action of MR antagonism with spironolactone.
Methods
All drug exposures to antihypertensive medications, including spironolactone, were identified from BioVU through electronic prescribing tools and MedEx,125 and at least one of the following identifiers, dose, route, frequency or duration, was required for a medication exposure to be considered valid. In addition, spironolactone, aldactone, or aldactazide prescriptions must be listed at least twice, at least one month apart, during the subsequent six-month period. Any patient without at least one BP measurement during the baseline period and at least two BPs measurements during the response period was excluded.
Results
The decrease in DBP correlated significantly with baseline potassium, decrease in serum sodium, increase in serum potassium, increase in creatinine, and higher baseline sodium (Table 18). The decrease in DBP correlated significantly with the decrease in serum sodium and increase in serum potassium and creatinine (Table 18). The decrease in DBP correlated significantly with baseline HDL and potassium, higher baseline sodium, and increases in creatinine and serum potassium (Table 18).
Discussion
In AA, there was a significant positive correlation between the decrease in SBP and the decrease in DBP, decrease in serum sodium, increase in creatinine and increase in glucose. We found that spironolactone responders had a greater increase in serum sodium and a decrease in serum potassium after MR antagonism and that. Second, non-responders also had an increase in their serum potassium and a decrease in serum sodium after starting spironolactone.
Conclusions
Taken together, these findings suggest that nonadherence is not the dominant cause of the lack of BP response in nonresponders. These levels could be used in the BP response prediction model or to indicate the efficacy of MR antagonism. However, previous studies have reported limited value of adding aldosterone levels or ARR in predictive models of BP response to MR antagonism in resistant hypertension.229, 230.
Figures
Schematic of the spironolactone response algorithm and identification of the baseline and response periods for patients. If the visit date for the start of the baseline period occurs before six months before NSD, the baseline period begins at the six-month mark. 85.5% of the original Subjects not on three medication classes. at the start of spironolactone or. incomplete data for stable window n=999.
Tables
Managing High Blood Pressure in Blacks: An Update of the International Society on Hypertension in Blacks. Incidence of optimal treatment regimens in patients with apparently treatment-resistant hypertension based on office blood pressure in a community-based practice network. Systolic blood pressure and biochemical assessment of adherence: A cross-sectional analysis in the emergency department.
A single nucleotide polymorphism in the cyp4f2 but not cyp4a11 gene is associated with increased 20-HETE secretion and blood pressure. Association of a functional polymorphism in the cyp4a11 gene with systolic blood pressure in survivors of myocardial infarction.
Antihypertensive medication classes and pathways for blood pressure control
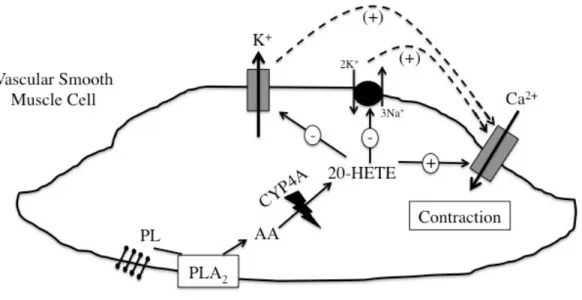
Metabolism of Arachidonic Acid to 20-hydroxyeicosatetraenoic acid
Function of 20-hydroxyeicosatetraenoic acid in vascular smooth muscle cells
Targets of 20-HETE and diuretic drugs in the renal tubule
Diagram of Vanderbilt University Medical Center’s electronic medical record linked
Diagram of the algorithms for the identification of patients with resistant (cases) and
The percentage of Case Type I patients prescribed a specific combination of
The percentage of Case Type II patients prescribed four, five, or six simultaneous
Schematic of the spironolactone response algorithm and identification of the baseline
Diagram of the algorithm for the identification of patients with resistant hypertension