MILLER RICHMOND: Psychosocial Care in the Syrian Refugee Crisis (led by Dr. Katherine Centellas). These results led to the conclusions that the implementation of psychosocial care is likely to require a change in the cultural perception of mental illness and that a major commitment must be made by host countries and the international community. New innovations in medical technology and a better understanding of mental illness will facilitate and improve the implementation of a psychosocial care infrastructure that reduces suffering from mental illness.
INTRODUCTION
When reporting mental health symptoms that were 'always' present over the past two weeks, 15.1% of respondents were so scared that nothing could calm them down; 28.4% felt so angry that nothing could calm them down; 25.6% felt so uninterested in things they used to enjoy; 26.3% felt so hopeless that they did not want to continue living; 38.1% felt so deeply upset by the conflict that they tried to avoid places, people, conversations or activities that reminded them of such events; and 18.8%. Older studies separate treatment of trauma and daily stressors, arguing that they cannot be treated through the same process. More recently, research shows that an integrated approach to specialist mental health care is integrated with a.
METHODOLOGY
Except when permission is given, NGOs will not be mentioned as a condition of the interview. Mental health statistics, especially in a crisis situation, are estimates of the true mental health burden on a population. This study will therefore be primarily from a qualitative perspective; however, some mental health data will be used to understand the scale of the crisis.
GLOBAL MENTAL HEALTH AND PSYCHOSOCIAL CARE
Therefore, this study will apply fundamental concepts of global mental health to analyze psychosocial care in the Syrian conflict. As we discuss later, many mental health programs working with Syrian refugees are struggling to keep up with the demand for care. It also depends on governments, non-governmental organizations and policies to instill an understanding of mental health that would reduce the stigma around mental illness.
THE SYRIAN CONFLICT AND VIOLENCE
The regime's crackdown on protests in the city of Daraa is the “spark that lit the Syrian flame” of the civil war (Sterling, 2012). The Assad regime is a minority Alawite sect that rules over a majority Sunni population, and Daraa, a city that is predominantly Sunni but historically close to the regime, is a case study in the tensions that have been building for years against the Assad regime across Syria in Sunni-majority areas. He will do whatever it takes to maintain his power as evidenced by the atrocities described below.
The sustained, violent tactics of actors in the Syrian Civil War over the past six years have been brutal on the general population, with comparisons commonly drawn to the Rwandan genocide and the Holocaust (Landler, 2014). All these groups contribute to the flow of refugees to surrounding countries and the traumatic experiences they bring with them through physical and emotional scars in the form of lost limbs, PTSD and depression. Although trauma and violence come from all groups in the Syrian conflict, the regime has contributed much of the terror.
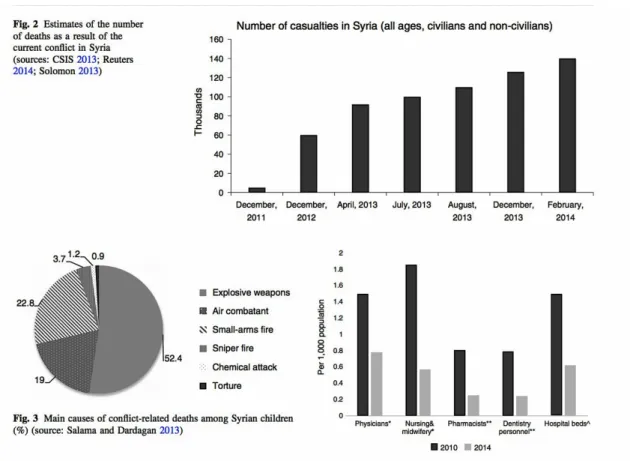
This usually took place during mass hangings in the middle of the night, after a “military process of one to two minutes” (Amnesty, 2017). Chemical attacks have “psychological, social and political consequences,” and after an attack “general levels of malaise, fear and anxiety can remain high for years, exacerbating pre-existing psychiatric disorders and beyond.” The UN and other organizations conservatively estimated in April 2016 that 400,000 people died in the conflict, the majority as a result of bombs (UNHCR, 2017).
All statistics detailed in the graphic are traumatic, against the Geneva Convention, and constitute war crimes, but I want to draw particular attention to the loss of health care workers for this study.
SYRIAN REFUGEE CRISIS IN JORDAN
Many Syrians had family in Jordan and the borders had been quite fluid in previous years due to Bedouin groups living in the area long before the border was established in 1921. As ISIS began to expand into northern Syria and the Assad regime began and allies more bombings in the conflict, there was a large increase in Syrian refugees crossing into Jordan in 2013. News media, celebrities and advocacy organizations often travel to refugee camps to advocate on behalf of Syrian refugees, as they can seen below in the photo of Ben Stiller and Angelia Jolie in Zaatari camp with UNHCR.
Most refugees have settled in urban or suburban areas in northern Jordan and Amman (UNHCR, 2015). It registered 9.5 million people in the country, including 2.9 million “guests” (Jordan Population Statistics Department, 2015). Jordan raises a number of unique issues in the context of refugee law: the country has not ratified the 1951 UN Convention Relating to the Status of Refugees and the 1967 Protocol.
Furthermore, the role of the state, UNHCR and (I)NGOs in providing protection and assistance. In fact, a group of unregistered refugees in the area taught the younger children what they could, but many of the women were also uneducated. If the estimate of unregistered refugees is correct, 1.4 million Syrian refugees are in Jordan, or about 1 in 6 people in the country are Syrian refugees and have arrived in the last 6 years.
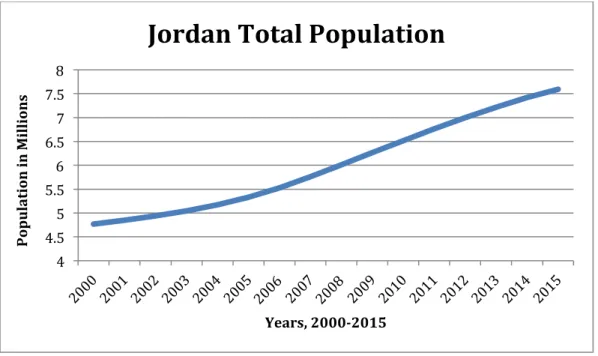
In Figure 3 below, a conservative estimate from the World Bank shows a population increase of nearly 50% in the last 15 years.
PUBLIC HEALTH IN THE SYRIAN CONFLICT
The NCD, and more specifically, chronic disease burden is relevant for two reasons when analyzing mental health and psychosocial care capacity in the conflict. Although this article focuses on mental health and psychosocial care, Syrian refugees' bodies undergo changes from. Second and perhaps most importantly, primary health care workers did not treat mental health because it was believed to be a fundamentally different kind of illness than they were equipped to treat.
Mental health services are often the last health services to be developed and integrated into primary health care (Saraceno et al., 2007). The destruction of health services in Syria as a method of waging war and as collateral damage has already been discussed at length, but it should be independently noted that the current infrastructure for mental health in Syria is non-existent. A strong mental health system was long overdue in Syria, and destroying the entire system will likely set back the development of the mental health infrastructure by decades.
Since 2007 in Jordan, mental health and psychosocial care have dealt with similar issues related to the centralization of services in cities and the shortage of health workers. The number of psychiatrists, psychologists and social workers per 100,000 was almost double or four times that of Syria in some professions, but there were still few mental health providers in absolute terms (Okasha et al., 2012). Interestingly, Jordan had more mental health professionals before the crisis, which probably didn't matter to the Syrian refugees.
It is possible that more mental health clinics were established in Jordan due to the influence of Western governments and development agencies, or in response to the large number of refugees the country was already hosting.
RESULTS
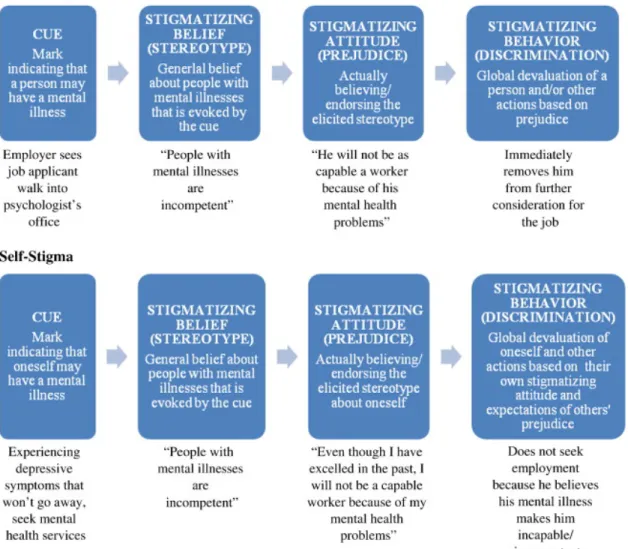
Mental health stigma can be divided, across cultures, into two dimensions: public stigma and self-stigma, which are explained below in Figure 4 (Corrigan & Kleinlein, 2005). Sleiman, informed me that feelings of helplessness regarding mental health care among PCPs were quite common. The separation of traditional MH services and mental health services exacerbates the divide between physical illness and mental illness.
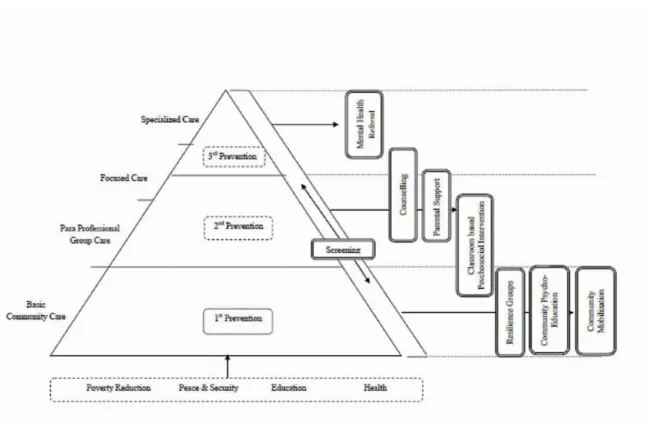
Doctors were not fully aware of non-traditional forms of mental health treatment, such as psychosocial care. Although not ideal, this fits the pyramid models of the MHPSS discussed in Global Mental Health and. NGOs and UNHCR have scaled up their deployment of mental health professionals, but the current number of professionals is not enough.
Mental health care as a crisis response needs to be implemented at the population level with the amount of traumatic events that have been and are still happening in the Syrian civil war. Legal issues were another problem affecting the delivery of mental health and psychosocial care. NGOs should commit to training and building capacity for more Jordanian mental health professionals in the country.
While Jordan is undoubtedly one of the most hospitable host countries for Syrian refugees, there are several regulations that could be removed to increase access to mental health and psychosocial care. If this trend continues, mental health and psychosocial care could be seen as the first response for populations such as Syrian refugees in the future. Although telepsychiatry has been criticized for being impersonal, it has proven to be an effective means of providing mental health care (Perle et al., 2011).
CONCLUSION
An interview-based investigation of issues surrounding access to dedicated mental health facilities should also be conducted. I discuss the traditional separation of mental illness and physical illness at length, and it would be quite meaningful to better understand how the Syrian refugee community views a stand-alone mental clinic versus one. The mental health of children affected by armed conflict: protective processes and pathways to resilience.
Culture, context and the mental health and psychosocial well-being of Syrians: a review for mental health and psychosocial support professionals working with Syrians affected by armed conflict. 34; Surveillance and Control of Communicable Diseases in the Context of Conflict and Mass Displacement in Syria." International Journal of Infectious Diseases. Implementation of a Mental Health Care Package for Children in Areas of Armed Conflict: A Case Study from Burundi, Indonesia, Nepal, Sri Lanka and Sudan .
War exposure, daily stressors and mental health in conflict and post-conflict settings: bridging the gap between trauma-focused and psychosocial frameworks. Predisplacement and postdisplacement factors associated with mental health of refugees and internally displaced persons: a meta-analysis. An investigation into the integration of education and mental health treatment in the care of diabetes in Syrian refugee women.
Psychiatric interventions for traumatized asylum seekers and refugees: What do we know about their effect?.

