Migrants, Minorities and Historical and Contemporary Health Studies Edited by Lara Marks and Michael Worboys. Edited by Marijke Gijswit-Hofstra, Hilary Maarland and Has de Waardt 6. Health Care and Poor Relief in Protestant Europe 1500–1700 Edited by Ole Peter Grell and Andrew Cunningham.
Preface
Acknowledgments
She is also very grateful to Professor John Stewart and Elaine Ryder, who offered helpful advice and insightful comments at an earlier stage of this work. Helen would especially like to thank Professor Anne Digby for her endless contributions of support and encouragement, advice and constructive criticism, perseverance and encouragement.
Glossary and Conventions
QN Queen's Nurse: Fully qualified general nurses who have successfully completed an additional period of training in District Nursing at the Queen's Institute Training Center and have been admitted to the Queen's Institute Nursing Roll. QNI/QIDN Queen's Nursing Institute, Queen's Institute of District Nursing, also QVJIN Queen Victoria's Jubilee Institute for Nurses: Professional organization for Queen's Nurses and UK-wide advisory body.
Introduction
Is it possible to assess changes in both the public image and awareness of community nurses as well as the self-image and perceived status of community nurses during this period. This book provides a look at area nursing of the past, dealing with its nature and experiences of practice as told by area nurses.
The History of District Nursing
1 Historical Trajectories
Mary Scharlieb, herself a pioneering doctor, was appointed as one of the first lecturers of Queen's Trained Nurses. By the end of the nineteenth century there were more than 900 trained QNs on the Institute's roll.

2 What Became of the Lady?
The Interwar Period, 1919–1939
Now it was usually the lady of the manor, and the lady of the manor would have. This increase in the number of patients in the early 1930s changed the working experience of the district nurse.

3 War to Welfare State, 1939–1948
Their lack of commitment to the wider ideals of the QNI led to a return to the QNI in the post-war NHS negotiations discussed later in this chapter. Through the first three years of the war, QNM provides a vivid picture of district nurses living and working in a series of very difficult conditions. On the other hand, there were some foreign visiting staff members at several of the major district nurse training centers who had to be repatriated, some of whom this proved impossible and had to remain in the UK for most of the war. 8.
As a result of the bombing, patients, potential patients, and many of the association's volunteer collectors fled the cities. The QNI records quantify some of the war work on the lists requiring payment for the treatment of air raid victims by the Queen's Nurses.31 These refer not only to care at the time of the air raid, but to subsequent nursing care after the initial trauma. . This rift later influenced negotiations over the role of the QNI within the new NHS.
The common ethos seems to be universal and excludes descriptions of conditions that would be part of the common experience of the time. Nevertheless, in 1947, anticipating the fragmentation of the county nursing service, a warning was expressed regarding the responsibility of local health authorities for the training and supervision of nurses. QNI's failure to win the ministry can be seen as a rejection of the old order that it symbolized in many ways.
4 Changing Places, 1948–1979
As part of a move towards greater integration between hospital and primary health services and the development of the health care team, the organization of district nursing was revised in the 1960s. Hot on the heels of Changing Places from the NHS was the proposed creation of health centers across the country which would include district nurses as part of the team. This shift away from the traditional authority of the association committees represented a potential threat to the quality of district nursing.
It is not surprising to find that these members were Miss Merry, General Superintendent of the QNI; Dr. Struthers, Chairman of the Training Subcommittee of the QNI; and Miss Treleaven, senior supervisor of DNA Ranyard. A holistic approach to health care was part of the language of district nursing and part of its appeal.
According to a chief nursing officer at the time, it was the district nurse who led the primary health care nursing team. Throughout the 1960s and 1970s, changes in the nurse's role resulted from several factors, including the introduction of improved transport and communication and the creation of the GP attachment system. By the end of this period, the discrepancy between the ideals of the NHS and the realities of delivering a comprehensive "cradle to grave" health service was often all too apparent in the profession of district nursing.
Themes and Issues
5 Town Nurse, Country Nurse
District Nursing Landscape
Therefore, the traditional image of the district nurse as native to her community is not always true. Cities each had their own characteristics that affected the experiences of the nurses differently. In the mid-nineteenth century the highlands and islands were relatively well supplied with nurses, but this situation deteriorated by the turn of the century.
The creation of the Highlands and Islands (Medical Services) Board in 1913 tackled this problem. In the 1940s, largely due to the impact of the Highlands and Islands (Medical Services) Board combined with the proliferation of nursing associations affiliated with the QNIS and employing highly trained nurses, access to health services in remote areas improved, particularly in the provision of nurses. As there was no doctor on many of the islands, emergency cases had to be quickly transported to the mainland for hospital treatment.
But they were there most of the day, you see, and they all knew each other, and it was one. Decisions directly affecting the health and welfare of industrial communities were often under the control of local industrial owners. Charity of the kind described in Berry did not always come from the immediate locality.
6 Technology, Treatment, and TLC
Changes in the materials used for dressings, especially in the second half of the century, required regular updating of the nurse's knowledge and understanding of wound care. She commented that improvisation had become "less of a part of the nurse's work than in the past", although the provision of disposables and other nursing equipment was proving more costly. Many of the district nurses interviewed referred to a decline in the tender loving care (TLC) of informal care and, in particular, that provided by neighbors and relatives of patients.
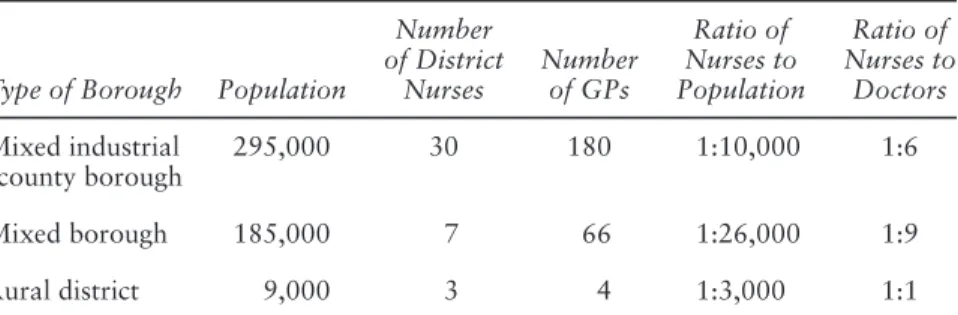
They were very good at cars, in the Southeast they even changed them quite often. In 1938 this was reiterated in the QNI report to the Interdepartmental Committee on Nursing Services,26 in which the QNI stated this. This has resulted in the services of Queen's Nurses being requisitioned by quite small districts with a population of 1,000 or even less.”27.
Technology, Treatment and TLC 145 often extremely severe as described by a nurse who trained in London in the 1930s:. Clearly, this made interprofessional communication even less feasible, especially in the rural setting. Pharmacological developments, particularly the introduction of antibiotics and sulfa drugs in the mid-twentieth century, made a dramatic difference to the work and experience of the entire primary care team, not least that of the district nurse.

7 Generalists and Generals: District Nursing Professionalisation
Taking medicine as an example, this includes ownership of the client, particularly in the public sector, and control of social and economic positions of power in the marketplace. Larson10 referred to this as "exclusive cognitive identity" that is necessary both for the creation and subsequently for the exploitation of the market. Bullough explained that "In the process of emerging as a profession, a professional group tends to delegate many of the more mundane tasks to other groups or individuals."16.
To the part of the nursing community that supports registration, represented by Mrs Breay, selective recruitment of suitable… This represents an overly simplistic view of medical and nursing theorists in the late nineteenth century. As more women were able to aspire to these status symbols, a decline in the social prominence of the community nurse does not seem surprising.
The result of this was that grassroots employment and supervision of district nurses fell largely under the office of the MOH. A further concern was the introduction of home help, assistant nurses and SENs to community nursing (see later) and the title home nurse to cover all grades of nurses working in the community, and was also used to describe care provided by voluntary organisations. such as local branches of the British Red Cross and St. Through changes in administration and the move to GP adherence, a better channel of communication between members of the primary healthcare team has been established.
8 Language of Caring
Care and Nurses’ Lives
Almost all of the older nurses interviewed, most of whom retired in the 1970s or 1980s, spoke of “non-medical care” as a feature of the past rather than the present. An accepted part of the nurse-patient relationship was for the nurse to care for the patient in this holistic way. Carrying out non-caring tasks was something that came up in the interviews.
Although a younger nurse in the 1980s said that she still performed non-nursing duties, there is a perception among older retired community nurses that this is a thing of the past. In the Nightingale Age, this idea of care took on greater significance as a central part of the concept of the ideal woman and the spirit of nursing. Orr continued to work in Greenock until his retirement and was a pioneer in the development of night nursing.
Orr spoke about his relationship with the doctors in the same way as the interviewees. Orr found his relationship with the county's doctors relatively conflict-free. This is echoed in the frequent use of the terms primary nursing or general nursing when referring to a type of care that was often provided but required little or no nursing expertise.