MEGAN ELISE MCLEOD: The District-Level Impact of Telemedicine: A Difference-in-Differences Analysis of the University of Mississippi Medical Center's Telemedicine Initiatives. This study analyzes some of the societal benefits of UMMC's telemedicine initiatives using a difference-in-differences identification strategy.
Introduction
Background
Interest in using telemedicine to provide care for the general public re-emerged in Norway in the early 1990s. The average wait time for an appointment with a primary care physician in the United States is 2.5 weeks (Topol, 2015). Based on these numbers, a doctor can complete 15 virtual visits in the time it would take to complete one in-person consultation.
Topol (2015) attributes much of this attitude to the paternalistic culture found in medicine, noting that "the doctor knows best" is more than just a figure of speech.
Mississippi
According to America's Health Rankings, the state's core health measures placed it collectively in the bottom three states in the nation for overall health since Annual Report - Mississippi"). In 2015, Mississippi had the highest rates of preterm birth, low birth weight and deaths from cardiovascular disease , stroke, diabetes, and septicemia in the state (“Stats of the State of Mississippi,” 2017).Although the state does not have significant differences in health status by education level, the.
In 2017, the counties in the northwestern part of the state that comprise the Mississippi Delta (De Soto, Tate, Tunica, Panola, Coahoma, Quitman, Tallahatchie, Bolivar, Leflore, Grenada, Sonneblom, Carroll, Holmes, Humphreys, Washington, Sharkey, Issaquena, Yazoo and Warren) are all in the bottom quartile of health factors for the state. Given the state's struggles with debilitating chronic diseases, shortage of health care providers, and sizable rural population, Mississippi seems an excellent candidate for implementing telemedicine in an effort to increase access to care and efficiency. Mississippi also has no geographic restrictions on where service can be provided—except that the patient must live within the state—and honors a wide range of specialties, even going so far as to allow a non-Mississippi-based provider (who is licensed) too late. to practice in .. Mississippi) to be reimbursed for storage and shipping services not available in Mississippi (Miss.
In Mississippi, residents of 53 of the state's 82 counties are more than a 40-minute drive from specialty care (Michael Adcock, FACHE, email correspondence, May 2017). The University of Mississippi Medical Center (UMMC) – the only academic medical center in the state – recognized and responded to this geographic disparity in access to care. More than 500,000 patient visits in 69 of the state's 82 counties have been recorded since the center's inception (in 2003) with just three locations, and today it has grown to more than 200 locations, not including patients' homes” ( University of Mississippi Medical Center, 2017).
Data
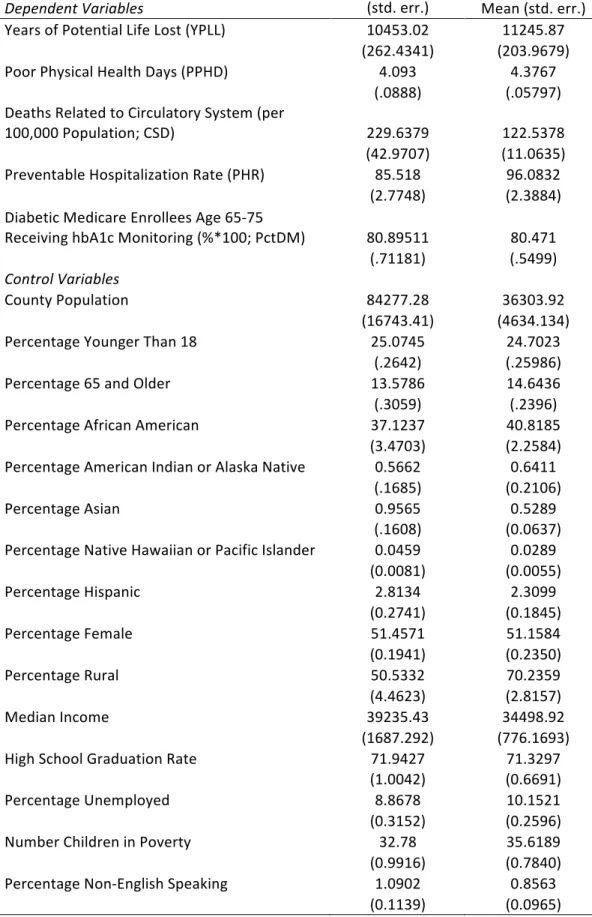
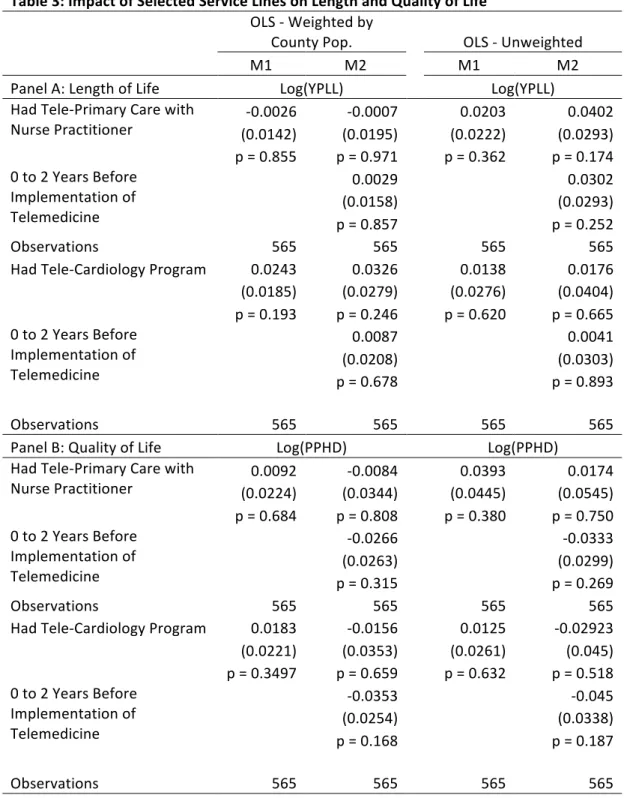
In this data set, PPHD is defined as the average number of physically unhealthy days reported in the past 30 days (age-adjusted) from the Behavioral Risk Factor Surveillance System (BRFSS). These life expectancy and quality of life outcome variables are used to evaluate the effects of the general presence of telemedicine in a country, depending on whether the country had one or more service lines versus no service lines. The impact of tele-cardiology is evaluated based on the number of circulatory system-related deaths (per 100,000 population; . CSD).
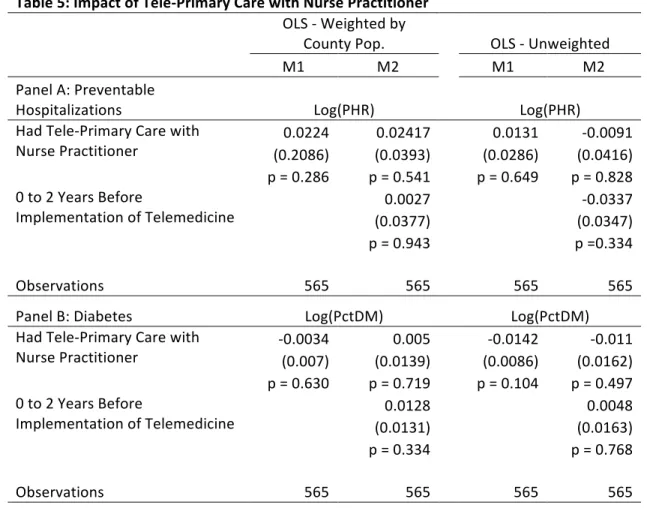
The impact of tele-primary care is assessed based on two outcome measures: preventable hospitalization rate (PHR) and the proportion of diabetic Medicare enrollees aged 65–75 years receiving HbA1c monitoring (PctDM). Monitoring HbA1c is thought to be one of the best ways to see if a person's diabetes is being managed well. Because of the expected non-normality in the distribution of these variables, the log of each outcome variable is used in the regressions.
To account for possible confounding factors from different demographic and socio-economic compositions of provinces, control variables are included in the regressions. These include the percentage of the county that is under age 18, the percentage of the county that is over 65, the racial composition of the county, the percentage considered rural, the median income, the percentage of unemployed, the percentage with only a high school education, the percentage of children in poverty, and the percentage who do not speak English. Both weighted (per provincial population) and unweighted averages are reported for each of the variables.
Identification Strategy
Note that 𝑇𝑟𝑒𝑎𝑡𝑖×𝑃𝑜𝑠𝑡𝑡 = 1 only if unit i is in the control group and period t occurs after the administration of treatments, and = 0 otherwise. Therefore, the 𝛽3 coefficient is the main parameter of interest because it represents the before/after difference for the treatment group minus the before/after difference for the control group. Outcome𝑖t is one of the health outcomes for district i in year t (YPLL, CSD, PHD, PHR or PctDM; . see Table 1 above).
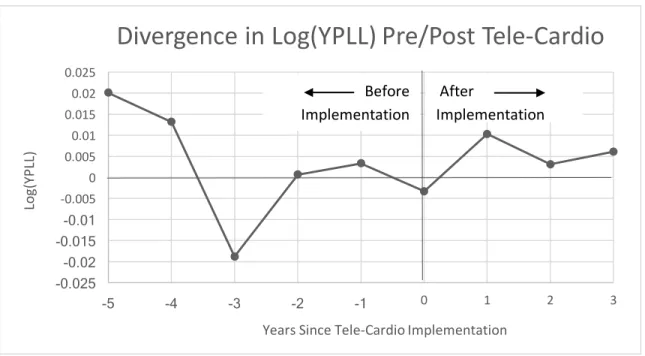
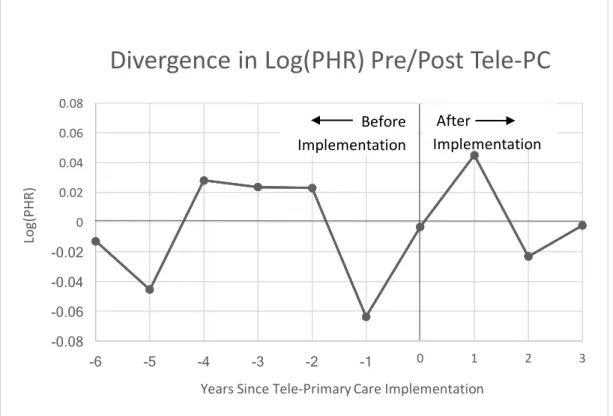
Equation (3) is identical to equation (2) except for the inclusion of variable leadp𝑖t, which is a leading indicator that = 1 if the observation of Outcome𝑖t occurs within p periods before the implementation of a telemedicine program (e.g. .indicates p = 2) a window of 0 to 2 years) for a county in the treatment group and = 0 otherwise. Graphically, evidence of divergence in trends in treatment and control counties prior to implementation indicates a violation of the identifying assumption. Here, YrPrep𝑖t = 1 when observation Outcome𝑖t occurs within p periods before implementation of the telemedicine program (e.g. if p = 1, YrPre1𝑖t = 1 when Yeart = 2013 and if the telemedicine program was implemented in 2014 for the county in question) and = 0 .
A graph of these 𝛽4 and 𝛽5 coefficient estimates provides a visual representation of the difference in health outcome trends between treatment and control counties over time. Furthermore, if the estimates of 𝛽5 from equation (5) trend in one direction or the other after the introduction, this would indicate that the introduction affected the outcome 𝑖t in the treatment group but not in the control group. Estimates of 𝛽5 capture dynamic treatment effects, while 𝛽1 represents the overall average effect.
Results
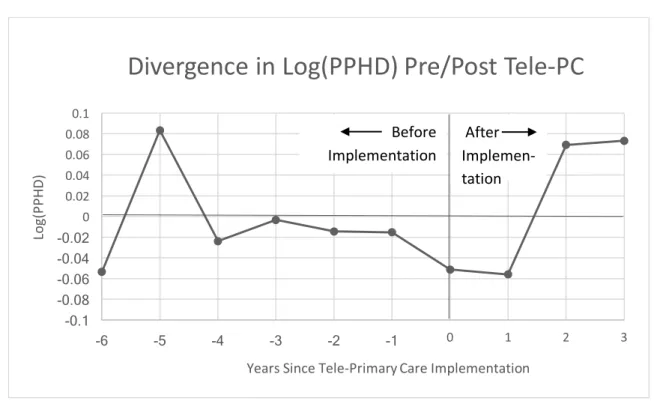
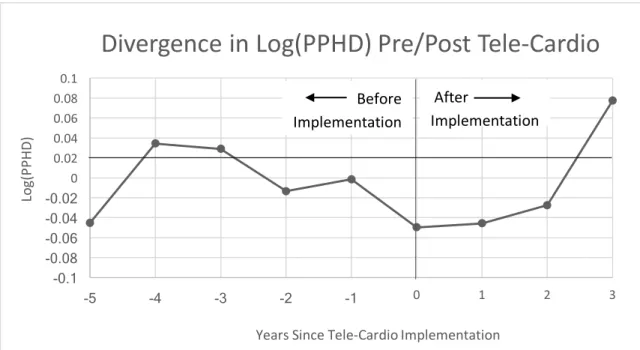
The YPLL and PPHD outcomes are regressed on treatment variables related to whether or not a county had a teleprimary care program (panel A) or a telecardiology program (panel B). In fact, the coefficient estimates for the PPHD regressions performed on the impact of teleprimary care and telecardiology on PPHD both changed from positive to negative with the inclusion of the leading indicator (panel B). These estimated values show the differences in trends for YPLL and PPHD between treatment and control countries before and after the implementation of teleprimary care and telecardiology.
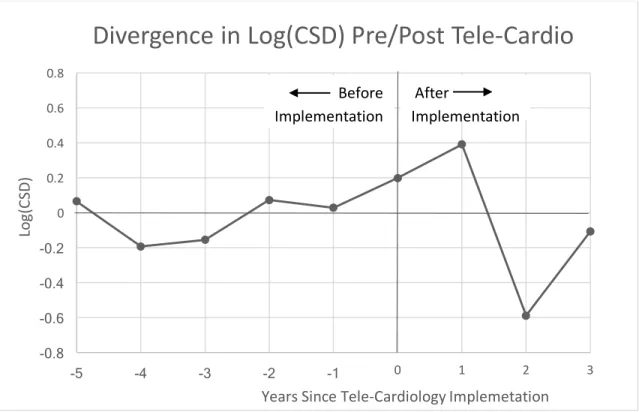
In Figure 1, for example, the difference in trends for YPLL before the introduction (ie, coefficient estimates of 𝛽4) of teleprimary care deviates from zero, especially for p = 4, 5 and and –6 in the figure), indicating that the identification assumption in this case may not be true. Also, there is no significant deviation from zero after implementation (i.e., 𝛽5 . coefficient estimates), which means that the introduction of teleprimary care did not significantly affect YPLL in the treatment districts. Similar conclusions can be drawn from graphs 2–4 regarding the effect of telecardiology on YPLL and the effects of telecardiology and telecardiology on PPHD.
So while it seems encouraging that estimates of the effect of telecardiology implementation are moving in the expected direction with a decrease in heart-related deaths, no solid conclusions can be drawn from the model. The same regression framework was used to find out the effects of implementing a tele-primary care line. Greater access to primary care providers should, in theory, reduce the number of avoidable hospitalizations by providing essential care before a medical problem requires hospital-level treatment.
Therefore, the model was used to estimate the effects of implementing a teleprimary care line on preventable hospitalization rates (PHR) and on the percentage of diabetics enrolled in Medicare receiving blood glucose monitoring (PctDM). Again, the first two columns in Table 5 contain estimates from Ordinary Least Squares (OLS) regressions weighted by county population, and the last two columns contain estimates from the unweighted versions of the same OLS regressions.
Discussion
This may be due to an increased awareness of one's own health with the implementation of tele-primary care. Further analysis of later observation periods may be able to investigate whether the increase in PPHD continues. Finally, there was evidence of a likely violation of the common trend assumption underlying the difference-in-differences method.
UMMC is aware of the potential for growth in data collection and analysis and intends to use some of the resources from the grant that came with being named a National Telehealth Center of Excellence for this purpose. Director of the Center for Telehealth Michael Adcock says, "While our center has been able to show some impressive results, we haven't had the staff to focus on researching telehealth delivery models and outcome comparisons. The hope here is that telemedicine continues to grow in state of Mississippi, and that the collection and analysis of related data will add to the knowledge of the subject.
Perhaps as adoption of telemedicine continues to spread and more and better data become available for investigation, studies of similar design may be able to elicit causal relationships between telemedicine programs and public health outcomes at the county or even state level. Amendments to the HIPAA Privacy, Security, Enforcement, and Breach Notification Rules Under the Health Information Technology for Economic and Clinical Health Act and the Genetic Information Nondiscrimination Act; Other Amendments to the HIPAA Rules. Department of Veterans Affairs, Veterans Health Administration, Deputy Under Secretary for Operations and Management, Veterans Integrated Services Network 16, Houston VA Medical Center.