The work of this thesis would not have been possible without the support of many people. Without the coordination and advice of the Chemical and Physical Biology program leaders at Vanderbilt, namely Professors Al Beth, Hassane Mchaourab, and Bruce Damon, my continuation of this work would not have been possible. No one has been more important to my mental health and the completion of this work than my wife, Christina.
This work could never have been completed without her, and for that I will always be grateful.
INTRODUCTION
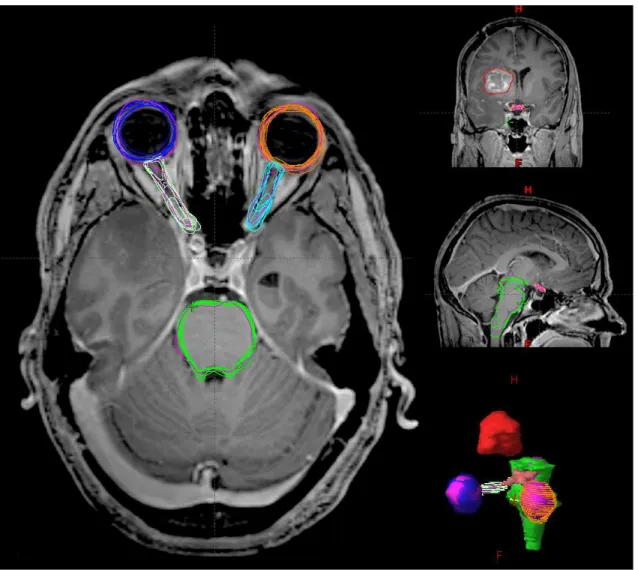
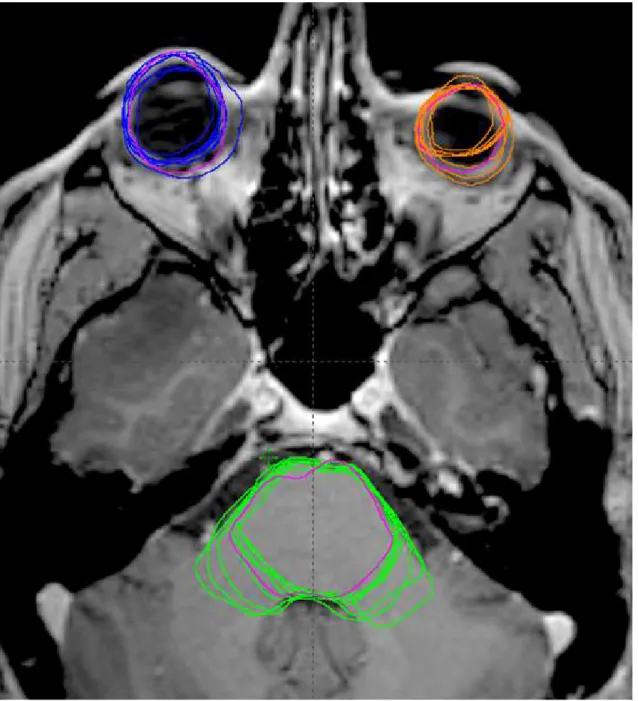
An even more obvious example is at the border between the brainstem and the spinal cord. We apply the combined transformations to the atlas delineations to create a segmentation of the structure of interest. In radiotherapy, we mostly deal with damage to the retina and the lens of the eye.
Also note that this reviewer appears to have segmented the optic nerve at the level of the pituitary gland (we leave the other expert's chiasm in place for reference).
CHARACTERIZATION OF SEGMENTATION VARIANCE
COMPARISON OF MANUAL AND AUTOMATIC SEGMENTATION METHODS FOR BRAIN STRUCTURES IN THE PRESENCE OF
SPACE-OCCUPYING LESIONS: A MULTI-EXPERT STUDY
Finally, local non-rigid registration is performed between the local affine registration results and the atlas image. The STAPLE algorithm uses expectation maximization to provide a probabilistic estimate of the ground truth. This means that the distribution of automatic volumes falls within the variation of individual doctors.
Furthermore, the coefficient of variation of the automatic structures, 11–16%, was consistent across all organ structures. Maurer et al.,2003) and then evaluated on the contour points of the automatic segmentation and the doctor segmentation. Figure II.8 shows the proportion of contour points that fall within 2 mm of the simulated ground truth as a function of rater and structure.
This value can be considered the true positive rate, whereby any contour point drawn within a 2 mm shell of the simulated ground truth scores positive. Each of the geometric measures showed that the automatic segmentations fall within the variation of the expert group, which is shown visually in box plots (figures II.4–II.7). Bondiau and colleagues (Bondiau et al., 2005) investigated atlas-based segmentation of the brainstem using MR images from 6 patients and 7 experts.
This is evident from the variance of the distribution of the Dice index (Figure II.6) of the automatic compared to the simulated ground truths, which is smaller than that of the doctors. The automated system was also near the top of the expert group for the 2 mm true positive rate shown in Figure II.8.

IMPACT OF EDITING ON SEGMENTATION VARIANCE AND ACCURACY
SEGMENTATION MODIFICATION IMPROVES EFFICIENCY WHILE REDUCING INTER-EXPERT VARIATION AND
THE PRESENCE OF SPACE-OCCUPYING LESIONS
Much of the methodology in terms of ground truth estimation and metrics was covered in depth in our previous work. A non-rigid local registration is performed between the affine local registration results and the atlas. Each voxel in the distance map contains the Euclidean distance between that voxel and the nearest ground truth edge voxel.
Contour points that were within the boundary of the ground truth were labeled negative, and those outside were labeled positive. Others have achieved normality by transforming data, such as by using the logit function (Zou et al., 2004). Each distribution consists of the pairwise comparisons between the de novo and the edited segmentations for each of the eight raters.
In Figure III.5, it is clear that across all structures and raters, the median DSC increased with editing of the automatic contours. To this end, we compared low-quality regions (slice DSC < 0.5) in the de novo study with the same regions after editing the automatic contours. So far, the results have focused on the performance of the automatic system in the context of editing compared to the experts' de novo segmentations and the unedited automatic segmentations.
The density of outliers within the bands is proportional to the number of outliers outside the plot range. The dotted line is drawn at the median for the raw machine (A1). However, the best results came from editing the automatic segmentations, which were consistent across structures.
This is likely a result of the reduced variance of the A1 edited class compared to the other edited classes.
DOSIMETRIC IMPACT OF AUTOMATIC SEGMENTATION
The sources of the segmentations were 1) the automatic segmentations (A1), 2) their own segmentations (self) and 3) their peers' segmentations (peer) from the first (de novo) study. Then, for each of the remaining 7 judges and A1, the trial was copied and rerun with the only change being that of the normal tissue input. Dose-to-ground truth segmentations were used to evaluate the impact of segmentation differences to our best estimate of the true organs at risk (the ground truth estimates).
Here we evaluate the plans as a function of the difference in dose between the evaluator segmentation (for which the plan was optimized) and the ground-truth segmentations (IV.4). Each black dot represents a difference in maximum dose compared to the average of the assessor's peers. The unit [%] of the y-axis in the Vxx graphs is the absolute difference in percentage volume, not a percentage error.
The minimum and maximum doses for the targets varied slightly more, but their range of variation across all plans, including A1, was less than 2% of the prescription dose. However, there were individual cases that may have been clinically important, with differences in maximum dose as high as 10 Gy more to the brainstem and chiasm than delivered by the rest of the group. The automated system resulted in plans that worked quite well within the variation of the physician-derived plans.
The variation in this analysis was muted compared to that of the dose reporting differences. Maximum dose, although the most commonly used figure of merit for the normal tissues of the brain, is more susceptible to these variations than volume doses.

DISCUSSION AND FUTURE DIRECTIONS OF RESEARCH
Other body sites require much more expert time (more than an hour) for segmentation, especially in the head and neck. In Chapter III, we presented results of a study to test the interaction between the automatic segmenters and the human experts. Even given the results of the de novo study, it is likely that automatic segmentations will be reviewed by the end user.
With this in mind, we tested the interaction of humans and an automated editing system. We were also interested in the effect of editing outside the context of an automatic system. Rather than being limited to traditional anatomical atlases, users can invoke an automated system to incorporate the knowledge base into the atlases of the target patient as a starting point.
Again, we found that the automated system performed well within the context of the experts. This may have important implications for clinical trials and toxicity studies and may explain some of the differences noted between current studies. We propose similar studies to those presented in the present work, but with a different method for data acquisition.
In the previous studies, we collected data through the clinical treatment planning systems in a laborious process that requires a lot of manual intervention to input and output the necessary data structures. This would be an important contribution, especially if an editorial review could be conducted, as previous evaluation work in the head and neck region has been exploratory, using only a few raters and patients (Chao et al.,2007;Stapleford et al .,2010). ).
BIBLIOGRAPHY
2007), 'Reduce variation and improve performance of computer-aided target volume delineation using a deformable image registration approach', Int J Radiat Oncol Biol Phys Combining registration and active shape models for automatic segmentation of lymph node regions in head and neck CT images', Med Phys Evaluation of multi-atlas based strategies for thyroid segmentation on head and neck CT images for IMRT', Phys Med Biol Commissioning and clinical implementation of a sliding gantry CT scanner installed in an existing treatment room and early clinical experience for precise tumor localization', Am J Clin Oncol Analysis of treatment planning time between systems and planners for intensity modulated radiotherapy', JACR Bootstrap methods and their applications., Cambridge University Press. 2008), "Evaluation of an atlas-based automatic segmentation software for the delineation of brain organs at risk in the clinical context of radiation", Radiother Oncol Nouvelles recherches sur la distribution florale, Bulletin de la Societe Vaudoise des Sciences Naturelles Lessons from QUANTEC: reporting and collection recommendations of dose-response data, Int J Radiat Oncol Biol Phys 76(3 Suppl), S155–160. 1999), "A radiographic and tomographic imaging system integrated into a medical linear accelerator for localization of bone and soft tissue targets", Int J Radiat Oncol Biol Phys.
2005), "Effects of non-normal distributions on confidence intervals around the standardized mean difference: Bootstrap and parametric confidence intervals", Educat Psychol Meas Systematic evaluation of three different commercial automatic segmentation software solutions for adaptive therapy in head and neck disorders. , prostate cancer and pleural cancer', Radiat Oncol Statistical techniques for comparing gauges and measurement methods: a critical review', Clin Exp Pharmacol Physiol. Effects of radiation dose on optic nerve volume and chiasma', Int J Radiat Oncol Biol Phys 76(3 Suppl Radiation associated brainstem injury', Int. 1996), 'Forming inferences about some intraclass correlation coefficients', Psychological Methods Intensity-modulated use of radiotherapy in USA 2011), 'Quality assurance of US-guided external beam radiation therapy for prostate cancer:. 2009), Automatic segmentation of optic nerves and chiasm in ct and mr using optimal atlas-guided medial axis and deformable model algorithm, v. Automatic segmentation of pelvic structures from magnetic resonance images for radiotherapy of prostate cancer', Int J Radiat Oncol Biol Phys.
2012), 'Online automatic and virtualCT segmentation in adaptive radiation therapy of the head and neck', Int J Radiat Oncol Biol Phys84(3), e427-433. metrics for accuracy assessment in medical image segmentation', IJCARS2, 169-181. 2008), "Automatic whole-breath segmentation using atlas approach and deformable image registration", Int J Radiat Oncol Biol Phys. 2011), "Adaptive radiation therapy for head and neck cancer - can an old goal evolve into a new standard?", J Oncol2011.
Adaptive radiotherapy for head and neck cancer - dosimetric results of a prospective clinical trial, Radiother Oncol Near simultaneous computed tomography-guided stereotactic spinal radiotherapy: an emerging paradigm for achieving true stereotaxy, Int J Radiat Oncol Biol Phys. Clinical validation of atlas-based autosegmentation of multiple target volumes and normal tissue structures (swallowing/chewing) in the head and neck, Int J Radiat Oncol Biol Phys Commissioning and quality assurance of an optically guided three-dimensional ultrasound target localization system for radiotherapy', Med Phys Phase I three-dimensional conformal study of radiation dose escalation in newly diagnosed glioblastoma: Radio Therapy Oncology Group Trial 98-03', Int J Radiat Oncol Biol Phys Dosimetric evaluation of automatic segmentation for adaptive IMRT for head and neck cancer, Int J.
![Figure I.2: Brainstem: medulla. MR imaging sections [top row], CT [middle row], and fused image with several expert (green) and the automatic (purple) segmentations [bottom row]](https://thumb-ap.123doks.com/thumbv2/123dok/10731262.0/20.918.138.810.105.606/figure-brainstem-medulla-imaging-sections-middle-automatic-segmentations.webp)
![Figure I.3: Brainstem: pons. MR [top row], CT [middle row] and fusion [bottom row] images showing the pons](https://thumb-ap.123doks.com/thumbv2/123dok/10731262.0/21.918.136.810.104.617/figure-brainstem-pons-middle-fusion-images-showing-pons.webp)
![Figure I.4: Brainstem: midbrain. MR [top row], CT [middle row] and fusion [bottom row]](https://thumb-ap.123doks.com/thumbv2/123dok/10731262.0/22.918.134.811.292.799/figure-brainstem-midbrain-mr-row-ct-middle-fusion.webp)
![Figure I.5: Eye and recti muscles. MR [top row], CT [middle row] and fusion [bottom row]](https://thumb-ap.123doks.com/thumbv2/123dok/10731262.0/25.918.136.809.201.891/figure-eye-recti-muscles-mr-row-middle-fusion.webp)
![Figure I.6: Optic nerve. The right intraorbital optic nerve is shown in MR [top row], CT [middle row], and fused [bottom row] images](https://thumb-ap.123doks.com/thumbv2/123dok/10731262.0/27.918.136.814.215.895/figure-optic-nerve-right-intraorbital-optic-middle-images.webp)
![Figure I.7: Optic chiasm. The optic chiasm is shown in MR [top row], CT [middle row] and fused [bottom row] images](https://thumb-ap.123doks.com/thumbv2/123dok/10731262.0/28.918.135.812.215.896/figure-optic-chiasm-optic-chiasm-shown-middle-images.webp)