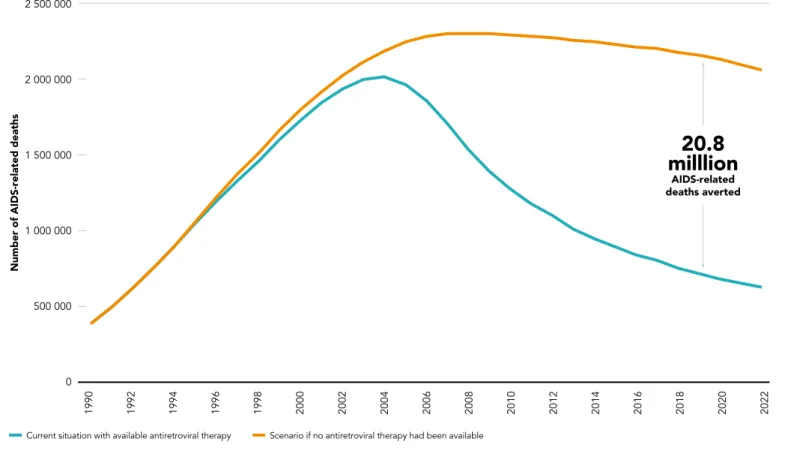
The risk of claims arising from infringement of any part of the work of third parties rests solely with the user. Thanks to freer access to HIV treatment, almost 20.8 million AIDS-related deaths have been prevented over the past thirty years (Figure 0.1).2 Overall, the number of AIDS-related deaths has fallen by 69% since its peak in 2004.
Many countries are doing the right things—and reaping the benefits
There is untapped potential for stronger HIV prevention
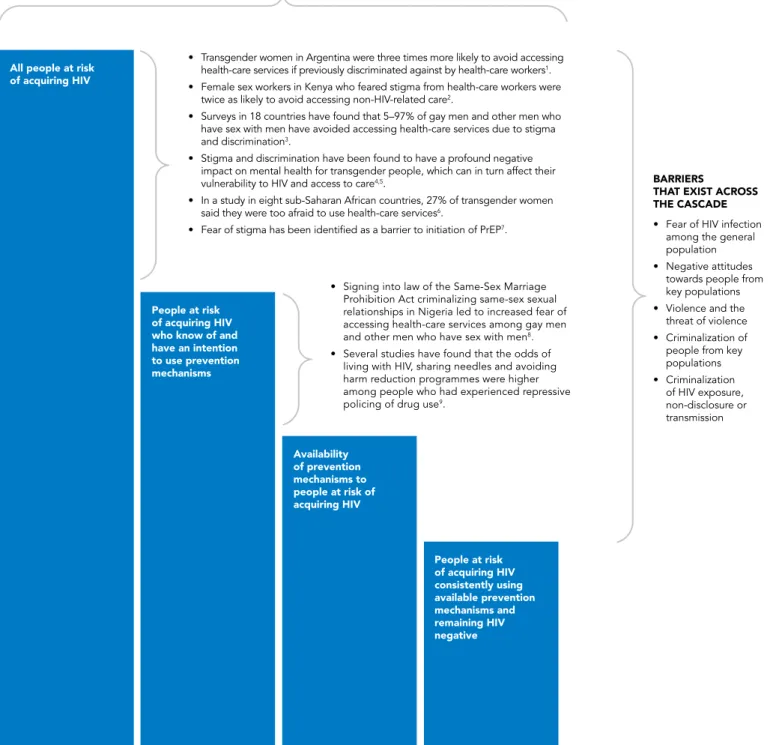
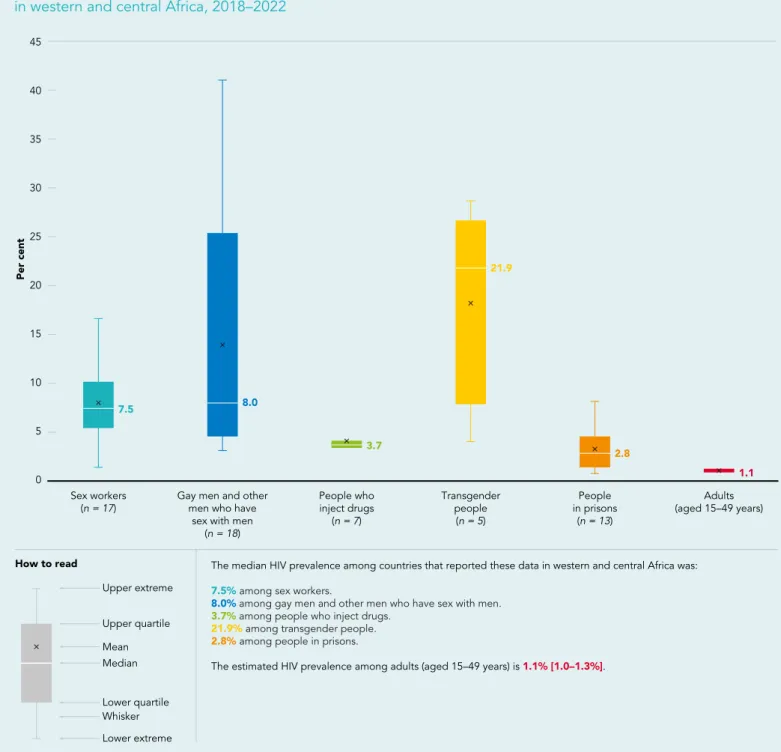
The vast majority of countries (145) still criminalize the use or possession of small amounts of drugs; 168 countries criminalize some aspect of sex work. In 2022, compared to adults in the general population (aged 15–49), HIV prevalence was 11 times higher among gay men and other men who have sex with men, four times higher among sex workers, seven times higher among persons , who inject drugs, and 14 times higher among transgender people.
Millions still miss out on treatment
HIV and other health services for people from key populations are rare, inaccessible or completely absent in many countries. 67 countries criminalize consensual same-sex intercourse; 20 countries criminalize transgender people; and 143 countries criminalize or otherwise prosecute HIV exposure, non-disclosure or transmission.
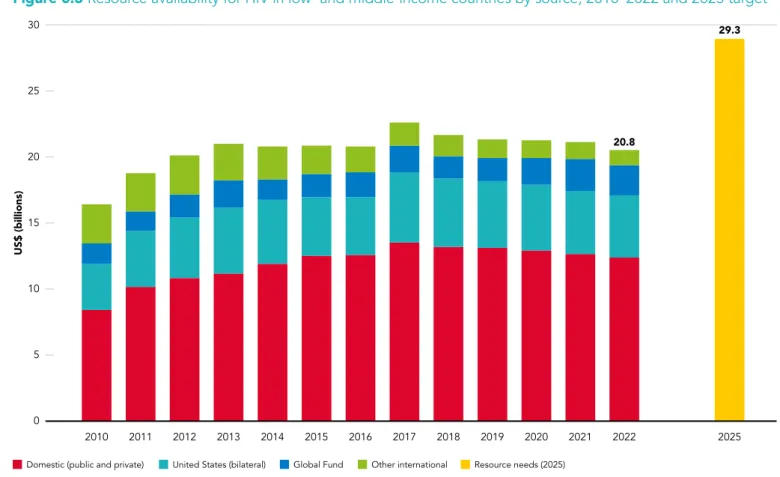
The funding gap is widening
Programmes and policies that put people first have the most impact
Greater equity will unlock new opportunities
PATHWAYS
TO SUCCESS IN THE HIV
RESPONSE
Many countries are
THE PROVISION OF EFFECTIVE TREATMENT
NUMBERS OF
AIDS-RELATED DEATHS GLOBALLY BY 51%
SINCE 2010
Remarkable
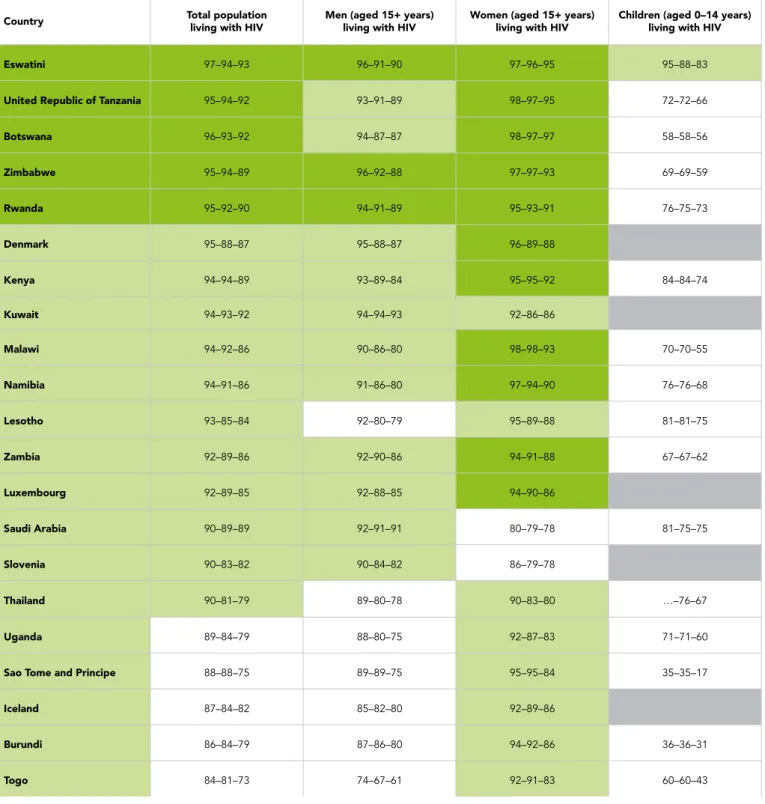
Note: achieving the 95-95-95 targets requires 95% of people living with HIV to know their HIV status (indicator 1); 95% of people who know their status are receiving antiretroviral treatment (indicator 2); and 95% of people on antiretroviral therapy have suppressed viral load (indicator 3). 81% of people living with HIV receive antiretroviral therapy; and 73% of people living with HIV have suppressed viral loads.

The transformative impact of PEPFAR on the global HIV response
Integrated services are boosting both HIV and tuberculosis (TB) outcomes
IN 2021, TB-RELATED DEATHS GLOBALLY
Not everyone is benefiting equally
Fewest new HIV
The biggest declines in new HIV infections
Numbers of new HIV infections among adolescent girls and young women are declining, but not as rapidly as among their male counterparts. Adolescent girls and young women are still at a very high risk of contracting HIV, especially in East and Southern Africa (see Chapter 2).

Prevention progress is slower outside sub-Saharan Africa
Gaps remain in combination prevention programs and in support programs promoting biomedical, behavioral and structural interventions for adolescent girls and young women and for men in general in most high HIV burden countries.
THE COUNTRIES WITH THE LARGEST
Most new HIV infections in these regions are among people from mainstream populations. There has been uneven progress in reducing new HIV infections among people from key populations.
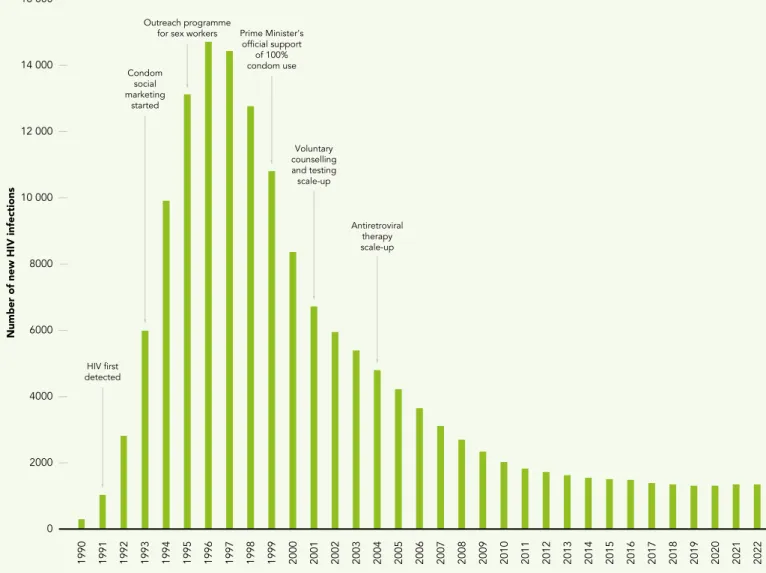
Strong leadership and effective key population programmes led to Cambodia’s steep reductions in HIV infections
Over three million children protected
ABOUT 82% OF PREGNANT OR
2022 saw the lowest number of new
The number of new infections in children fell sharply until early 2010 as coverage of antiretroviral therapies increased among pregnant and lactating women with HIV. Coverage of antiretroviral therapies for pregnant and lactating women and the number of new HIV infections in children have stabilized.

2022 saw progress in the removal of
Positive changes
How HIV
SUCCESSFUL TREATMENT
PROGRAMMES SUPPORT HOUSEHOLDS IMPACTED
IMPROVE THEIR ABILITY TO GENERATE INCOME
Leaving no one behind
The sharpest decline in the number of TB-related deaths was among people living with HIV. AIDS-related deaths TB-related deaths among HIV-negative people TB-related deaths among people living with HIV.

STRONG PREVENTION OF VERTICAL
This was evident, for example, when HIV laboratory systems, health workers and service delivery facilities were among the first to respond to the COVID-19 pandemic in many countries. This central feature of the HIV response illustrates the principle that affordable access to essential health care is a basic human right.
TRANSMISSION AND CHILD TREATMENT
The HIV response has excelled in building innovative partnerships and putting communities at the center (SDG 17). The multisectoral character of the Joint Program – which brings together the expertise and assets of 11 United Nations agencies and organizations – also typifies the partnership-for-development approach of the SDGs.
REDUCED NUMBERS OF AIDS-RELATED DEATHS,
The two largest HIV funders, the Global Fund to Fight AIDS, Tuberculosis and Malaria and the US President's Emergency Plan for AIDS Relief (PEPFAR), invest approximately US$2.5 billion per year in strengthening health systems (25). HIV Justice Network, 12 June 2023 (https://www.hivjustice.net/news-from-other-sources/belize-government-approves- amendment-to-outdated-section-of-the-criminal-code-related - na-transmission-hiv/).
BREAKING DOWN
BARRIERS
REMOVING
THE OBSTACLES THAT HOLD
BACK HIV
RESPONSES
Not everyone is benefiting from progress made towards
If we can identify the barriers that prevent people from protecting their health and well-being, we can act more effectively to remove those barriers. This chapter reviews the latest evidence on the limitations and HIV-related inequalities affecting people from specific populations, including adolescent girls and young women, children exposed to HIV, people from key populations of different ages and aging people living with HIV.
Adolescent
Providing women with an enabling
Intensified prevention where HIV risk is highest
There is wide variation in the incidence of HIV among adolescent girls and young women in sub-Saharan Africa. In 81% of sub-Saharan Africa's sub-national areas, and in most countries of the world, HIV incidence among adolescents and young women (aged 15 to 24 years) is estimated to be less than 0. 3 infections per 100 person-years.
Women and adolescent girls still lack basic information and services to
Gender-based violence
ACCORDING TO A RECENT ESTIMATE,
INFECTIONS BY 2030
More needs to be done to protect people from high levels of sexual and gender-based violence in prisons and other closed settings, and to provide support for survivors and witnesses who need it (36). A growing number of countries provide some HIV-related services in prisons and other closed settings, but much stronger measures are needed to protect against sexual violence in prisons and other closed settings.
An overlooked group in the pandemic
For example, transgender people in prison are estimated to be up to 13 times more likely to be sexually assaulted than cisgender people in prison. Prison authorities are responsible for combating gender-based sexual violence, the exploitation of vulnerable people in prisons, and all forms of victimization in prisons.
TRANSGENDER PEOPLE IN PRISONS ARE
CISGENDER PEOPLE IN PRISONS
Data from three cities in South Africa show low rates of HIV treatment retention and particularly low rates of viral suppression among transgender women living with HIV (Figure 2.2). Antiretroviral treatment retention and viral suppression rates are typically poor among transgender women. Figure 2.2 Testing and treatment cascade for HIV-infected transgender women in three metropolitan areas in South Africa, 2018–2019.
New insights can help unlock HIV prevention in high-burden settings
Analysis of 15 years of HIV surveillance and phylogenetic data from Uganda shows that the gender disparity in HIV transmission is increasing and the increasing male contribution to HIV transmission is associated with lower antiretroviral therapy coverage and lower rate of viral load suppression in men than in women. . Overall, this analysis highlights that achieving and maintaining very high levels of antiretroviral therapy coverage and sustained viral load suppression among people of all genders is an ongoing priority if cycles of HIV transmission are to be broken ( 53).
Mothers and
Targeted efforts are needed to reduce vertical HIV transmission
In West and Central Africa in 2022, almost two-thirds of new infections in children were due to their mothers not receiving antiretroviral therapy, including during pregnancy or breastfeeding periods. In East and Southern Africa, no single factor dominates, although a significant proportion of new infections in children can be attributed to their mothers who cannot avoid acquiring HIV during pregnancy or breastfeeding.

Reaching all women with services
Testing strategies that go beyond early childhood diagnosis are also essential: 62% of children living with HIV but not on treatment are estimated to be between the ages of five and 14. Increasing outpatient and family index testing could connect more undiagnosed children and adolescents with HIV to treatment and care.

New commitments to end AIDS in children
This can be changed with integrated person-centered procedures that track mother-child pairs and ensure that mothers receive test results. Health outcomes for children receiving HIV treatment remain worse than for adults.
Prevention and
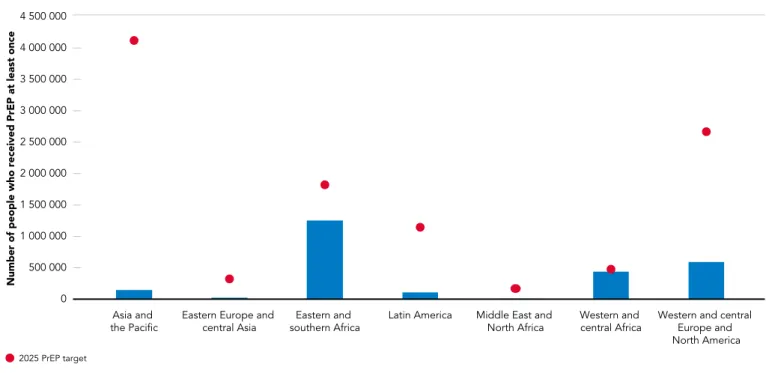
The full potential of PrEP is not being realized
HIV risk and incidence vary
Multi-month handouts, the use of virtual service platforms, the removal of parental consent, and the promotion of greater roles for community-led organizations may further increase the use of this powerful prevention tool. Although high, the current effectiveness of the ring in preventing HIV infection does not yet match the optimal use of oral PrEP (73).
Antiretroviral medicines for HIV prevention
Today, the majority of people living with HIV who are aware of their HIV-positive status and take their treatment as prescribed are not at risk of sexually transmitting HIV. Effectively scaling up the use of antiretroviral drugs for HIV prevention requires differentiated people-centered approaches and systems to be in place to create an enabling environment for people living with HIV.
IN 2022, 21 MILLION PEOPLE WERE TESTED
Barriers that prevent access to affordable HIV services for people from key and vulnerable populations, including migrants and refugees, must be removed. A series of barriers still need to be overcome to make U = U a reality for all people living with HIV, but the message is gaining traction worldwide as a call for greater access to HIV treatment, better services for people living with or be affected. by HIV, and less stigma and discrimination.
WITH ONLY SIX MILLION PEOPLE IN 2015
This means ensuring that medicines can be taken freely and on time without exposure to stigma and discrimination, that treatment literacy is prioritized, and that health systems are robust (no stockpiles of effective medicines) and people-centred, so that viral load can be shared by all. be monitored. Strong community involvement and well-established networks are essential to ensure full access to viral load testing and sharing of results so there is knowledge of viral load status.
Condom programmes are falling off the agenda
Voluntary medical male circumcision (VMMC) can make an even
VMMC programs face two major challenges – a lack of funding and the need to reach more men in their twenties and older (services have so far focused primarily on youth). Data from population-based estimates of the impact of HIV from 2015 to 2019 show that VMMC use is worse among men in lower wealth quintiles.
A road map towards boosted HIV prevention
A few countries, including Malawi, are having some success in targeting their VMMC programs at younger men. Programs may also do better in convincingly addressing men's concerns about potential adverse effects and community stigma, and in highlighting the broad HIV and other health benefits of VMMC (86, 87).
People-centred approaches can close many of the treatment gaps
Services at schools and in workplace settings are not ideal for reaching those men, while services at health facilities may involve high transport costs (85).
Children and adolescents with HIV are losing out
Treatment gaps between men and women are wide
SUB-SAHARAN AFRICA, 78% OF ADULT MEN
OF ADULT WOMEN
They were more likely to remain in care and achieve viral suppression than those who transitioned to inpatient care (106). Community-led monitoring has also been shown to be a valuable source of information for improving HIV services (108).
WHEN CLIENT-CENTRED TRAINING AND
These include increased use of HIV self-testing (99), partner engagement testing methods, workplace-based interventions, social network strategies, provision of convenient HIV services in outpatient clinics, and targeting places frequented by people more likely to be at risk for HIV (100-103). Tailored support at health facilities and from community-led organizations would enable people of all genders, ages and populations to remain in HIV care.
MENTORING WERE INTRODUCED AT 24
Community-led interventions are particularly essential to ensure that people from key populations access and fully benefit from HIV treatment, and they may have the added benefit of reducing the burden on clinics (106). Analysis of data from observational studies and randomized controlled trials found that retention in HIV care was similar when the number of routine clinic visits was reduced (from twice to once a year) and antiretroviral drug refills were spread over periods longer (six and not three months). ) (110).
Advanced HIV disease is posing new challenges
Persons re-engaging in care after discontinuation of treatment and who have advanced HIV disease should be offered a comprehensive clinical evaluation. WHO recommends that a package of screening, prophylaxis, rapid initiation of antiretroviral therapy and intensified adherence interventions should be offered to all people living with HIV who present with advanced disease.
A long tail of new HIV infections
The package includes interventions to prevent, diagnose, and treat common opportunistic infections, including TB, cryptococcal meningitis, and serious bacterial infections, and to ensure rapid initiation of antiretroviral therapy and intensified adherence support (111). There is also a need to improve HIV education at the community level so that people living with HIV are aware of services and supports that can help them adhere to treatment.
As people with HIV grow older, new challenges are emerging
FAILURE TO PROTECT PEOPLE FROM KEY
HIV responses still neglect
There has been little progress in reducing
Higher risk, less protection, more HIV infections
PrEP coverage among people from key populations is very low, typically below 5%, including sex workers and gay men and other men who have sex with men. Studies show a high willingness to use HIV prevention, including PrEP, among gay men and other men who have sex with men (137).
Prevention gains in a challenging context
Programs that prioritize public health priorities over punitive and discriminatory approaches are making progress in various aspects of their HIV response (e.g., in Australia with the introduction of PrEP, in Cambodia with prevention services for sex workers, in Estonia and Portugal with services for people, who inject drugs, and in Thailand and the United Kingdom of Great Britain and Northern Ireland with inclusive policies for gay men and other men who have sex with men) – but these success stories are far from the norm. Gay men and other men who have sex with HIV-positive men who have been diagnosed Gay men and other men who have sex with men living with HIV who are undiagnosed HIV-negative gay men and other men , who have sex with men.
Harm reduction services are too scattered and too small
Very few countries are on track to meet the 2025 needle and opioid agonist maintenance targets.
Funding increases will make a big difference
Source: UNAIDS financial estimates and projections, 2023; UNAIDS Global AIDS Monitoring, 2023; Stover J, Glaubius R, Teng Y, et al. Note: data are from 80 countries that have reported their most recent spending on prevention and community support interventions for key population interventions.
Laws that put people in harm’s way
Laws that criminalize people from key populations or their behavior remain on statute books across most of the world. In Pakistan, a federal court struck down parts of the Transgender Persons (Protection of Rights) Act (151).
Stigma and discrimination still block progress
The vast majority of countries still criminalized the use or possession of small amounts of drugs in 2023, 168 countries criminalized some aspect of sex work, 67 countries criminalized consensual same-sex intercourse, 20 countries. Niger and Zimbabwe have adopted harmful policies that restrict freedom of association, including for LGBTQI+ organizations; anti-transgender legislation was introduced in the United States of America; and efforts are underway in the Russian Federation to expand laws banning so-called “LGBTI propaganda” (152).
THE EVIDENCE IS CLEAR
Some countries have limited the scope or removed laws that criminalize the transmission, exposure or non-disclosure of HIV and drug use. Uganda's new Anti-Homosexuality Act (2023), signed into law in May 2023, provides for severe penalties against LGBTQI+ people and organizations (148), and Indonesia's new penal code contains articles that violate women's and people's rights from sexual minorities (149, 150).
ENDING MISGUIDED AND UNJUST
CRIMINALIZATION IS GOOD FOR PUBLIC
HUMAN RIGHTS OBLIGATION (142)
A systematic review of qualitative findings on factors enabling and hindering HIV testing uptake in sub-Saharan Africa. Social network-based strategies to improve HIV testing uptake and linkage to care among men who have sex with men in sub-Saharan Africa.
OPPORTUNITIES FOR QUICKER
PROGRESS TOWARDS
AIDS
Investing in a sustainable response will render health,
SEIZING THE OPPORTUNITIES
MOMENTUM TOWARDS ACHIEVING A RANGE
The HIV funding gap is widening
The HIV funding gap is widening
Domestic HIV funding is vital but under stress
ALMOST HALF OF THE REPORTING 62
ANNUAL HIV BUDGETS WILL BE AT 2023 LEVELS
This suggests that, at least in the short term, external financing will continue to be key for low- and lower-middle-income countries to end AIDS. The continued reliance on external financing for HIV responses is at odds with health spending patterns generally in low- and middle-income countries.

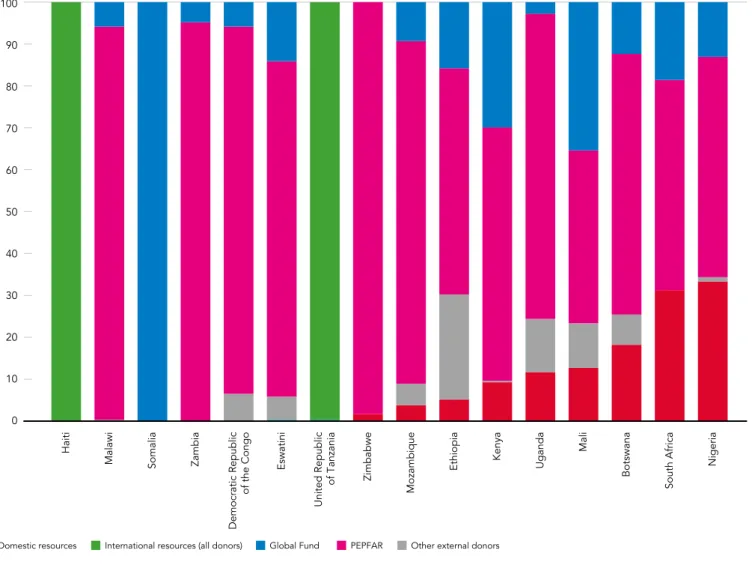
International HIV financing remains crucial in many countries
HIV prevention programs are usually heavily dependent on international resources (mainly the Global Fund and PEPFAR) (Figure 3.5). The Global Fund and PEPFAR are the main sources of funding for HIV prevention programs.
GLOBAL TARGETS CALL FOR SPENDING
Innovations for sustainable financing of the AIDS response
Programmes that put people first
A SYSTEMATIC REVIEW OF STUDIES ACROSS 10
Eliminating stigma, discrimination and punitive approaches would reboot HIV
Harmful laws, stigma and discrimination
AT LEAST ONE IN THREE REPORTING
HEALTH-CARE SERVICES DUE TO CONCERNS
CONFIDENTIALITY OR OTHER ISSUES
Community-led services can make an even bigger difference
Steer more support to
Lack of institutional arrangements linking the activities of these organizations to comprehensive health systems and weak technical and managerial capacities further hinder the current work and future contributions of community-led organizations. Trusted partnerships between public health systems and community-led organizations are important and can contribute to greater effectiveness, cost savings and efficiency in national HIV responses.
Greater equity will unlock new
ON AVERAGE THE UNIT PRICES FOR
REGIMENS ARE ALMOST 2.5 TIMES HIGHER IN
Equitable access to new technologies and other innovations
Inequities and inequalities are
In clinical trials, people who received long-acting cabotegravir were 70-90% less likely to acquire HIV than people who took daily oral PrEP (34, 35). As part of the agreement with the Medicines Patent Pool, three generic manufacturers will be able to produce long-acting cabotegravir, and additional manufacturers may be added at a later stage.

IN CLINICAL TRIALS, PEOPLE RECEIVING
A voluntary licensing agreement signed in 2022 between manufacturer ViiV Healthcare and the Medicines Patent Pool allows about 90 countries to buy cheaper generic versions of the medicine once generic manufacturing begins. The Indian company Cipla announced in May 2023 that it will manufacture a generic version of long-acting cabotegravir at its plants in South Africa.
CABOTEGRAVIR WERE 70–90% LESS LIKELY
This has great potential to offer people, especially women, an additional option and greater autonomy to protect themselves from HIV infection. Countries excluded from the voluntary licensing agreement are estimated to account for approximately 8% of all new HIV infections per year (approximately 120,000 new infections) (39).
Vaccine hopes suffer a blow
Social safety nets should reach everyone in need and reduce
To strengthen the contribution that social protection can make in the AIDS response, programs should aim to "include populations at risk of HIV infection or susceptible to the consequences of HIV infection" (64). A new study of the HIV inclusiveness of social protection programs in 20 low- and middle-income countries and across Latin America and the Caribbean found that none explicitly discriminated against people living with, at risk of or affected by HIV not (65).
THE PROVISION OF FREE HIV TREATMENT
Increased school attendance and several years of youth education are associated with a lower risk of contracting HIV, especially among adolescent girls and young women (57, 58). However, stigma and discrimination – towards people living with HIV and towards excluded and marginalized populations in general – were important barriers to access in all countries, underscoring the need to remove stigma and discrimination from social protection and health services to reap their benefits. full benefits.
Integrated
INTEGRATION OF HIV AND TB
Integration can support the
A large meta-analysis of 114 studies, mostly from sub-Saharan Africa, found that HIV treatment and care outcomes, including viral suppression, were better when integrated services were provided, while. Similarly, a systematic review of 19 studies, mainly from Asia, found that offering integrated HIV and sexual and reproductive health and rights to sex workers was highly cost-effective (71).
Integrated TB and HIV services can save millions more lives
TB treatment success rates are slightly lower for people living with HIV (77%) than for all people with a new episode of TB (86%). The success rate among people living with HIV is highest in sub-Saharan Africa (>80%).

Making greater use of other integration opportunities
It could also address some of the risks of developing non-communicable diseases among people living with or at risk of HIV. A meta-analysis of 26 studies from sub-Saharan Africa found that approximately one in five people living with HIV had hypertension, but that screening and treatment for hypertension was rare in most HIV clinics (88).
A STUDY IN LATIN AMERICA FOUND
Integrating HIV testing and treatment with maternal and child care has been instrumental in massively expanding antiretroviral therapy coverage among women living with HIV and their male partners, and in preventing millions of HIV infections in children. In some regions, these populations include significant numbers of people living with HIV, whose access to HIV treatment and other services is often destabilized.
THE INTEGRATION OF HIV AND RELATED
Geneva: Joint United Nations Program on HIV/AIDS; 2023 (https://www.unaids.org/en/resources/documents/2023/a-triple-dividend, accessed 2 July 2023). Geneva: Joint United Nations Program on HIV/AIDS; 2015 (https://www.unaids.org/en/resources/documents/2015/JC2725_communities_deliver, accessed 2 July 2023).
Asia and the Pacific
2022 DATA
Progress towards the 95-95-95 targets has been uneven across countries and populations in the region, reflecting difficulties in reaching people from key populations and their sexual partners with testing and treatment. All countries in the region, except New Zealand and some states in Australia, criminalize sex work.
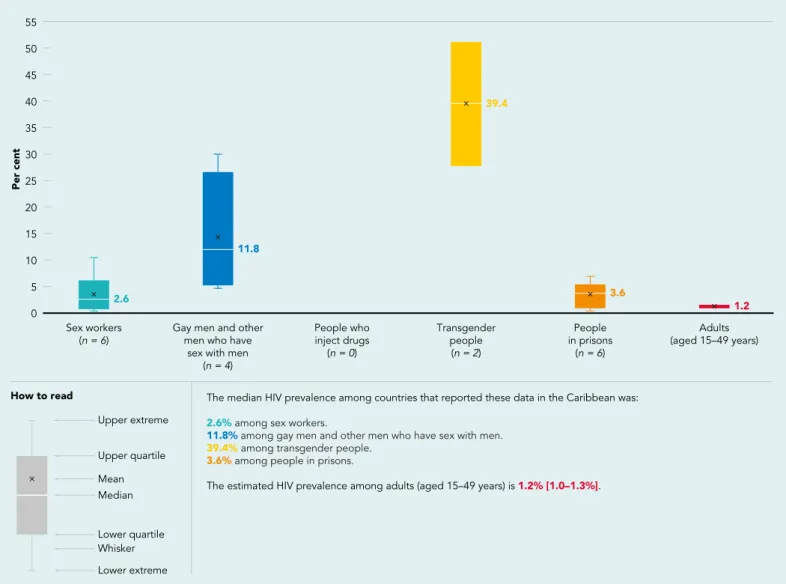
Caribbean
Eight countries and territories in the Caribbean1 have been validated by the World Health Organization (WHO) for the elimination of vertical transmission of HIV and syphilis since 2015 (1). 1 Greater efforts are needed to accelerate the elimination of syphilis and congenital syphilis in America.
Eastern and
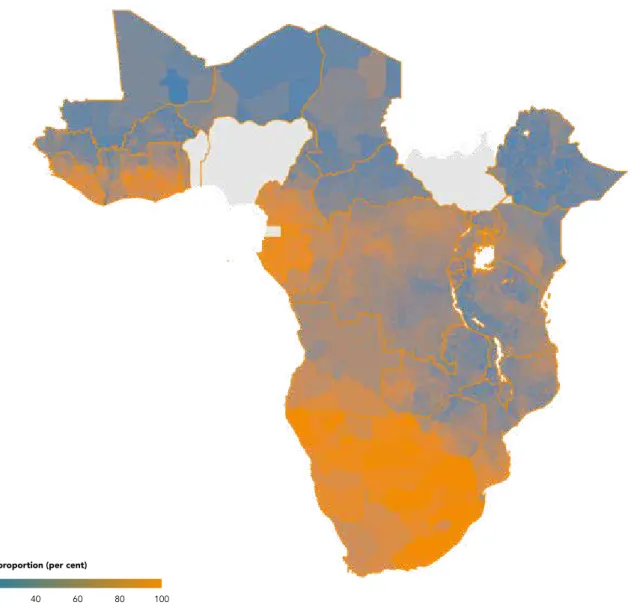
Note: analysis available for 16 countries in eastern and southern Africa with sub-national data required. Countries in the region not included are Comoros, Eritrea, Madagascar, Mauritius, Seychelles and South Sudan.

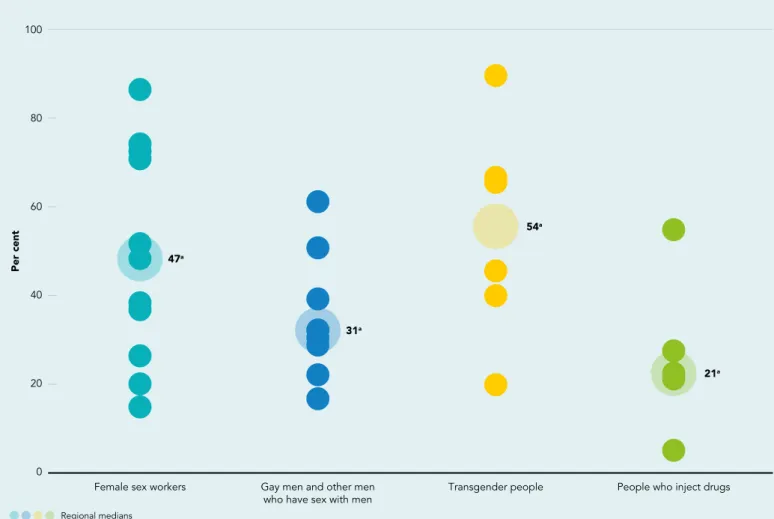
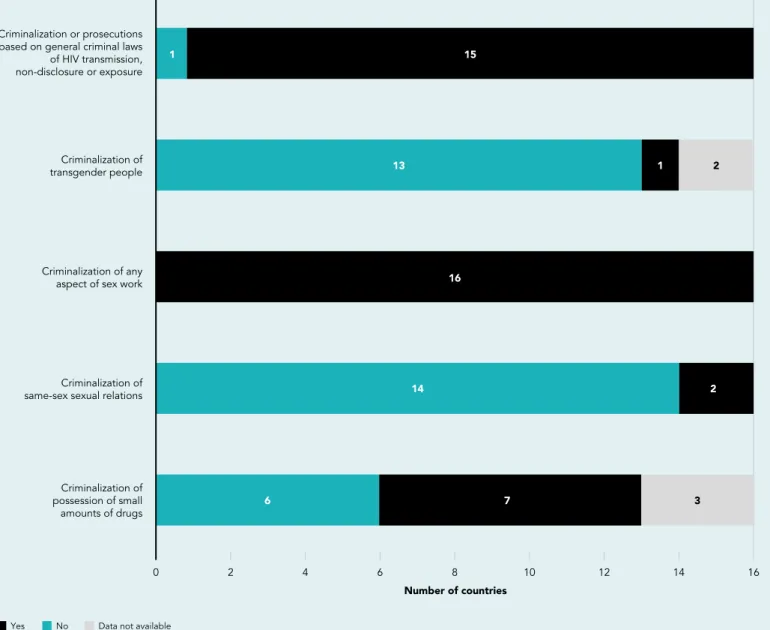
Most countries in the region retain laws that criminalize same-sex sexual relations, sex work or drug use. Removing or reforming these laws, consistent with public health evidence, will strengthen the HIV response and the human rights of people from marginalized populations, particularly key populations that continue to have much higher HIV prevalence than the general population (Figure 6.3) .
Eastern Europe and central Asia
Recent legislative changes, including those in the Russian Federation that restrict human rights and social space (1), have further compromised the delivery of essential HIV services (Figure 7.3). For example, since the beginning of the conflict, approximately 8,500 refugees from Ukraine affected by or living with HIV have had full access to public HIV, tuberculosis and harm reduction services in the Republic of Moldova.1 The sustainability of the HIV response remains a big problem. concern.
Latin America
Only nine countries in Latin America offer oral and on-demand pre-exposure prophylaxis (PrEP) to people from key populations. Thirteen countries in the region include PrEP in national guidelines, but only 10 offer oral and on-demand PrEP to people from key populations, and only five allow community-based delivery (Figure 8.3).

Middle East and North Africa
Status of the HIV epidemic in key populations in the Middle East and North Africa: knowns and unknowns. An evolving HIV epidemic in the Middle East and North Africa (MENA) region: a scoping review.
Western and central Africa
A significant number of pregnant women living with HIV in the region are not receiving antiretroviral treatment. More than one in 10 people from key populations living with HIV report that they avoid accessing health care because of stigma associated with their HIV-positive status (2).
Western and central
Europe and North America
There has been progress in adopting PrEP in Western and Central Europe and North America. Most countries in Western and Central Europe and the North American region have adopted the World Health Organization's recommendations for oral PrEP in national guidelines (Figure 11.3), but disparities in access to services persist, particularly for people of color and Hispanics in United States (4 ).

Combination HIV prevention for all
Progress towards the 2025 targets
Reduce the number of new HIV infections among adolescent girls and young women to less than 50,000 Number of people who received PrEP at least once during the reporting period, globally, 2022 Source: UNAIDS Global AIDS Monitoring, 2023 (https://aidsinfo. unaids .org/).
95–95–95 targets for HIV testing and treatment
Reduce the number of TB-related deaths among people living with HIV by 80% by 2025 (compared to a 2010 baseline). Between 2010 and 2021 there has been a 67% reduction in the number of TB-related deaths globally among people living with HIV.
End paediatric AIDS and eliminate vertical transmission
Between 2005 and the end of 2021, a total of 16 million people living with HIV were initiated on TB preventive treatment. Considering that 38.4 million people were estimated to be living with HIV, this is still much lower than the 90% target set for 2025.
Gender equality and empowerment of women and girls
Community leadership
Realize human rights and eliminate stigma and discrimination
Sub-target of the Global AIDS Strategy: Less than 10% of people living with HIV report internalized stigma by 2025. Sub-target of the Global AIDS Strategy: Less than 10% of people living with HIV experience stigma and discrimination in health care and in the community 2027.

Universal health coverage and integration
In four out of eighteen countries, more than half of people living with HIV surveyed reported internalized stigma. Percentage of people living with HIV who have experienced stigma and discrimination in healthcare and in the community, countries with available data. Source: People Living with HIV Stigma Index Surveys, 2020–2023.
Investments and resources
Introduction
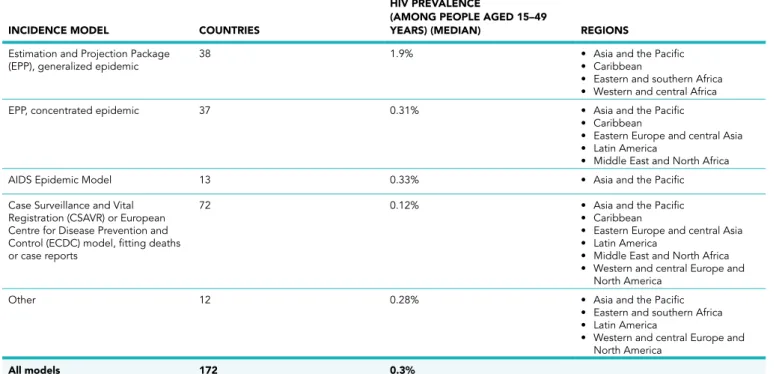
Countries where HIV transmission is maintaining an epidemic in the general population use the Estimation and Projection Package (EPP) module of the Spectrum modeling tool, which reflects a trend in HIV prevalence data from pregnant women attending antenatal clinics and from nationally representative population surveys. Most countries in Western and Central Europe and North America use AIDS-related mortality data from vital registry and HIV case reports and the delay between infection and diagnosis to estimate national HIV prevalence and incidence trends.
Uncertainty bounds around UNAIDS estimates
Selected data in the model - including the number of people on antiretroviral therapy and the number of women using services to prevent vertical transmission of HIV - are reviewed and further validated in partnership with the United Nations Children's Fund (UNICEF), the Organization World Health Organization (WHO), the United States President's Emergency Plan for AIDS Relief (PEPFAR) and its agencies, the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund) and other partners . In the 2023 round of assessments, subnational assessments were created and used by 38 countries (37 in sub-Saharan Africa, one in the Caribbean).
Improvements included in the 2023 UNAIDS estimates model
Demographic projection
Impact of antiretroviral therapy on HIV transmission
Mortality among adults on antiretroviral therapy
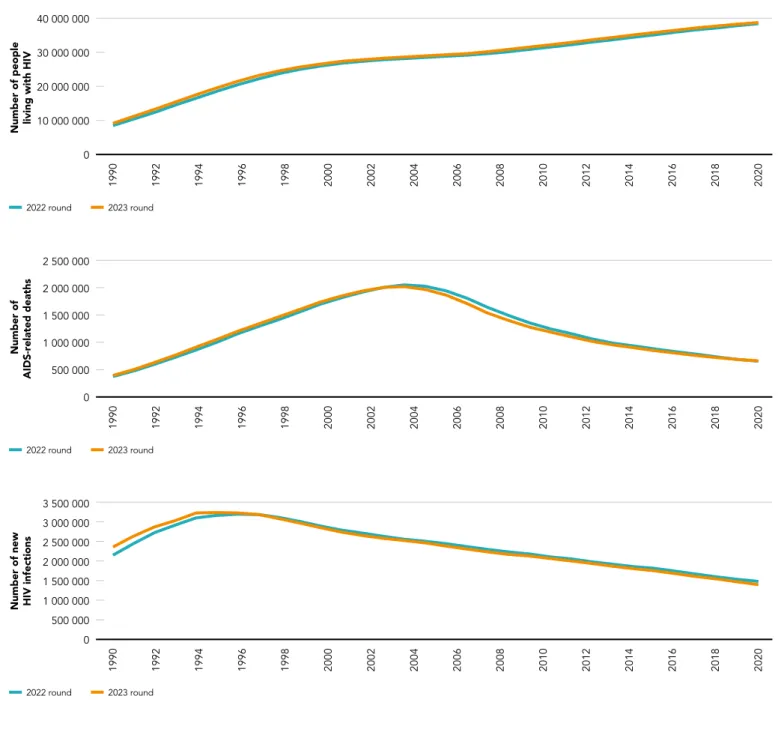
Shifts in the curves are the combined effect of the updated country data and the changes in model structure and assumptions described above. At the global level, trends in the number of new HIV infections, AIDS-related deaths and people living with HIV are similar to those estimated in the previous round, although there are shifts within some regions.
Publication of
The United Nations Political Declaration on HIV and AIDS: Ending Inequality and Getting on Track to End AIDS by 2030 set the testing and treatment targets at 95-95-95. When the numbers or coverage of the treatment target are expressed in relation to the total number of people living with HIV, this is called the HIV testing and treatment cascade.
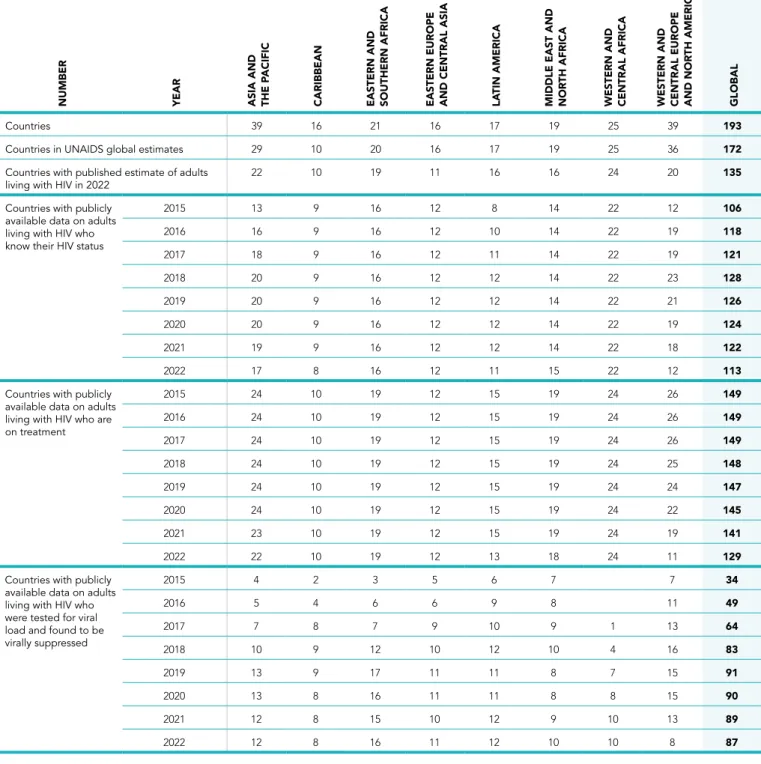
Data sources for constructing country measures
Countries with publicly available data on adults living with HIV who know their HIV status. Countries with publicly available data on adults living with HIV who have been tested for viral load and found to be virally suppressed.
Estimates of people living with HIV
Knowledge of HIV status
Knowledge of HIV status estimates from Shiny90 takes precedence over those derived directly from population surveys or program data. Both Shiny90 and the CSAVR estimate of knowledge of HIV status cover only adults aged 15 years and older.
People accessing antiretroviral therapy
Shiny90 estimates distinguish people living with HIV who have had an HIV test after seroconversion and are thus aware of their HIV status from those who converted after their last HIV-negative test. Shiny90 estimates knowledge status by gender and age, assuming adult male/female test rate ratios have remained relatively constant since 2010.
People who have achieved viral suppression
Some regions (e.g. Asia and the Pacific, Western and Central Europe and North America) have a higher percentage of countries with imputed knowledge of status or viral load suppression in 2022 compared to earlier years, as the latest data are still available has been reviewed. Limited data are available to inform knowledge of status in Asia and the Pacific, Western and Central Europe, and North America and Latin America.
New HIV infections by subpopulation
The ratios of infections in adults estimated by Goals and Optima were also used to estimate new infections among clients of female sex workers and non-client, non-key population male and female sex partners of people from key populations. Compared to previously published estimates of spread, the new estimated numbers of new infections among key populations are lower.
Calculation of pre-exposure
Quality of population size estimates
Cross-sectional estimates for HIV prevalence, antiretroviral therapy coverage, and HIV incidence are derived from the midpoint of the most recent nationally representative household survey. The model allows for the probability that people living with HIV have access to antiretroviral therapy in a contiguous subnational area.