I understand that any violation of the above will be a reason for disciplinary action by the Institute and may also attract criminal action from the sources who are therefore not properly cited, or from whom proper consent has not been taken when required . This dissertation would not have been possible without the guidance and help of several individuals who contributed in one way or another and provided their valuable assistance in the preparation and completion of this study. It was his encouragement, cooperation and support that helped in the successful completion of this thesis.
Cardiovascular diseases are one of the main causes of human physicality and mobility in society. Advances in wireless technology and data monitoring can be used to make state-of-the-art (Sot A) facilities accessible to patients in remote and rural areas. Although cardiologists are accustomed to the standard 12-lead (S12) system due to its decades of use and wide acceptance, in general such remote health care environments lead reduced (RL) ECG is appropriate for the above reasons, but may not be clinically acceptable for diagnosis.
The whole cardiovascular disease detection system can be described by 6 different parts, namely data acquisition, pre-processing, data transmission, coefficient generation, signal reconstruction and display on the monitor. The thesis includes a low-complexity and high-speed architecture design (for the pre-processing department) and its implementation on an FPGA and ASIC platform, which can be used for accurate 3-lead to 12-lead ECG signal reconstruction. The application of this architecture has been focused on remote monitoring of the cardiovascular system, where continuous sensing and processing takes place in low-power devices that are computationally limited, ie.
The thesis utilizes research for a reduced 3-lead to 12-lead reconstruction methodology and highlights the associated technical challenges in implementing the architecture and proposes a low-complexity and high-speed architecture for computationally intensive wavelet analysis.
Introduction .......................................................... Error! Bookmark not defined
Vision
An apparently possible solution to the highlighted problems is to obtain an S12 system of the RL system, which can be performed using lead reconstruction. Lead reconstruction methodologies have been primarily inspected to address the issues faced by patients and healthcare providers in hospital settings [6]–[13]. However, they have also been evaluated in the context of remote health monitoring applications. One of the best among the various lead reconstruction algorithms is the reduction from 3 leads (consisting of leads I, II and one of the six precordial leads) to SotA 12 lead signal reconstruction with the artifact preprocessing module [14].
A patient must be registered at a nearby health center which maintains a database to keep track of each patient's health. After using personal reconstruction methodology, the S12 system is reconstructed from the RL system, which is sent to the health center when the patient needs to be monitored. After reconstruction, signals can be displayed on the cardiologist's mobile phone/tablet for further analysis and diagnosis.
Contribution of Thesis
Proposed Architecture
- Material
- Mother Wavelet-Symmlet with DWT
- Optimised Number of inputs
- Low complexity
- Robust
- Architecture Details
Of the 290 patients, 101 were used to verify the proposed architecture, and the rest were excluded from the study regarding their extreme artifacts and rhythm tempo. The algorithm for the already proposed and verified preprocessing module consists of baseline wander (BW) removal based on discrete wavelet transform (DWT) [17]. In this project, due to the hardware perspective of the wavelet transform, only DWT is considered. The number of input samples is equal to the power of 2 for both DWT and TIWT implementations.
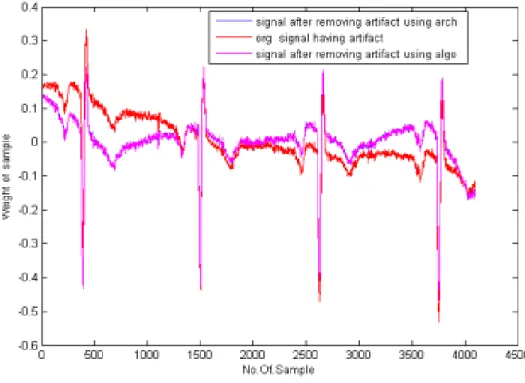
However, we took 4096 samples in our architecture, the reason was discussed in Section 2.4. To describe the implementation of the algorithm, we split the embedded Matlab code into easy-to-implement spreadsheet code using DWT for both baseline wandering (< 1Hz) and denoising (50–60 Hz) and checked the performance statistics. In this proposed architecture, we do not deal with the denoising part (50–60 Hz) during wavelet transform analysis because its values are less important compared to the baseline wander values (< 1 Hz).
Therefore, to obtain a trade-off between accuracy and hardware complexity along with memory requirement, we have performed the comparison shown in Fig. This is neither the simple replacement of the multiplier with the adder nor the implementation of distributed arithmetic where. However, in this architecture, only by exploiting the value of the coefficient, we can implement a multiplier-less architecture, which will again lead to the most desirable complex architecture for the rural health care environment.
Together with the low complexity and low power, the robustness of the architecture is a major problem when implementing an architecture. Therefore, we analyzed the algorithm from an architectural point of view and came up with a robust architecture. We analyzed and tested our architecture for a set of 101 patients with our already proposed algorithm, the details of which are shown in Table I, Table II and Table III in terms of R2, where correlation (rx) and regression (bx) are respectively described in section -IV.
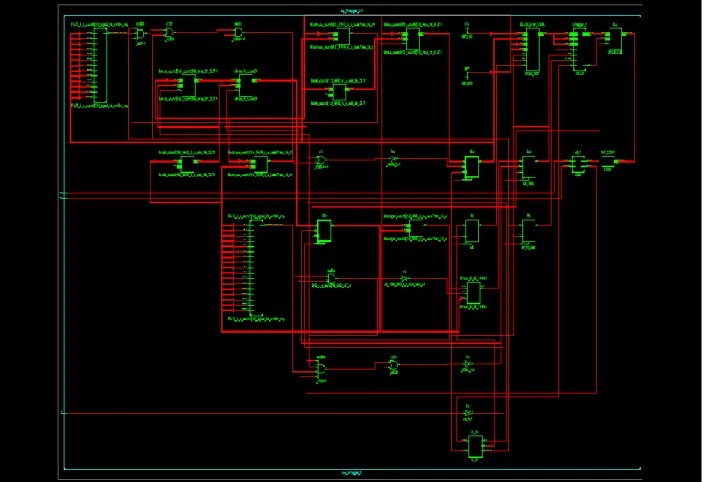
Here we propose a robust, low-complexity architecture of the preprocessing module (which is the most computationally intensive part) for the CVD detection system. The entire architecture is divided into 3 subblocks (controlled by a controller logic), consisting of decomposition, reconstruction and then subtraction. In our architecture, i ranges from 1 to 16 , because the wavelet considered in our architecture is Symmlet-8, which has 16 samples.
While doing the wavelet analysis in conventional approach, we need to do intermediate down-sampling after each decomposition and up-sampling after each reconstruction step. But in our architecture we have achieved output without doing downsampling and upsampling, thereby reducing the delay factor.
Results and Discussion
FPGA prototype of proposed architecture
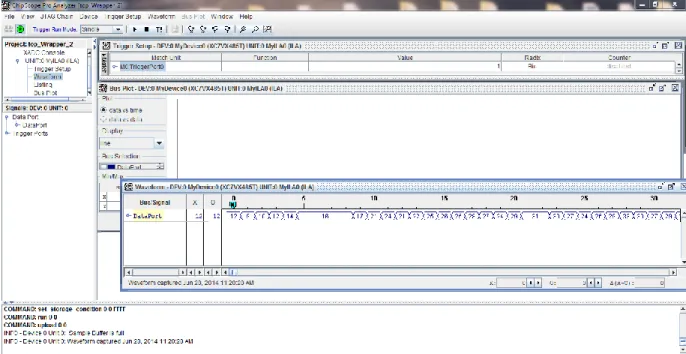
The proposed architecture was prototyped on an FPGA board with a Virtex-7 version with a clock frequency of 229.929 MHz, which clearly determines the speed of the proposed work. The result was analyzed and verified using Chipscope Pro analyzer. A snapshot of the FPGA prototype is shown in Figure 7, and Figure 8 shows the noise-free data resulting from the architecture using the Chipscope-pro analyzer.
ASIC Implimentation of proposed architecture
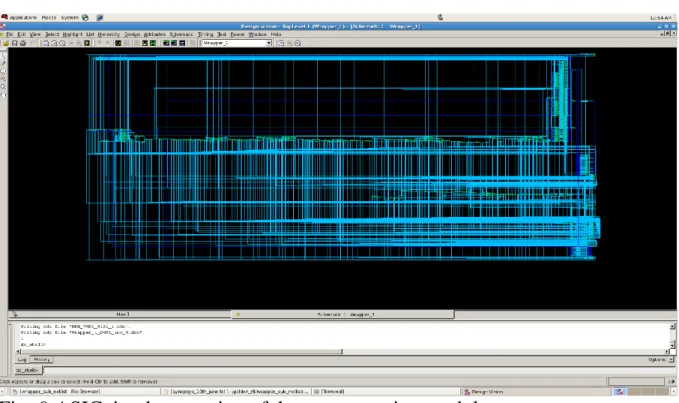
The ASIC implementation of the proposed architecture has been performed using the 130nm technology UMC library and the output has been verified in each and every step of the ASIC flow. The area result from ASIC implementation is 20.54mm square and a power consumption of 66.29mW without doing anything. any optimization. The concept of personal lead reconstruction has drawn a milestone towards the progress of the comprehensive health management system both in rural and urban areas. This intern will provide a reliable solution to the patient suffering from CVD by taking care of all the requirements arising from it.
As mentioned earlier, we proposed an algorithm in our previous work. A step towards personalized healthcare is coded in mat lab. To realize the proposed mat lab code, in this paper we propose a low-complexity, robust architecture to follow the step towards hardware implementation for the most computationally intensive part of the algorithm. Table I, Table II and Table III clearly provide comparison statistics between the already proposed algorithm and the proposed architecture. On the other hand, the hardware complexity of the architecture is drastically reduced by a number of transistors with an input of 2^12 samples and a word length of 16 bit, which reduces the power consumption of the overall architecture internally. a major benefit to the rural healthcare system.
Future work includes, a complete personalized health care system, which can be visualized as shown in Fig. 1 in both scenario-1 and scenario-2. Scenario-1, describes the case where doctors do not need to carry the heavy ECG SotA machine, but can carry a 3-lead ECG machine like a stethoscope and receive the signal in the physical presence of the patients and do all the pre-processing of necessary signal using our architecture (as a small hardware module) for removing the artifact from the signals and reconstructing the 12-lead ECG. Scenario-2 describes the offline mode of the personalized healthcare system, where patients can stay at their premises, do the necessary signal pre-processing and send the signal wirelessly to the healthcare center, where the SotA signal will be reconstructed with 12 plugs. for further diagnosis.
Paper Publication
2004Brechet, L.; Lucas, M.-F.; Doncarli, C.; Farina, D.; ,Compression of Biomedical Signals Using Mother Wavelet Optimization and Best-Basis Wavelet Packet Selection, Biomedical Engineering, IEEE Transactions on, vol.54, no.12, pp Dec. 4] Alesanco, A.; Garcia, J.; ,Automated Real-Time ECG Coding Methodology Guarantees Signal Interpretation Quality, Biomedical Engineering,. Linear affine transformations between 3-lead (Frank XYZ lead) vectorcardiogram and 12-lead electrocardiogram signals, J Electrocardiol, vol., 42, pp.