Alzheimer's disease wreaks havoc on the patient, and its degenerative nature can cause a prolonged period of anguish and anxiety for the patient's family. Marc Agronin has used his years of experience as a geriatric psychiatrist to create an extremely useful resource for psychiatrists and others treating patients with Alzheimer's disease or other dementias. Now in its third edition, Alzheimer's Disease and Other Dementias uses concise and clear language to outline the symptoms, effects, and treatments used to combat the progression of Alzheimer's disease and other dementias that older patients are likely to develop.
Agronin creates a volume full of humanity, knowledge, and insight that is sure to inform and improve the habits and methods of any clinician dealing with Alzheimer's disease and other forms of dementia. He is the author of numerous articles and books in the field of psychiatry and a nationally recognized speaker and expert on Alzheimer's disease and other late-life psychiatric disorders. From psychiatrist Alois Alzheimer's description of Alzheimer's disease to current methods of diagnosis and treatment, clinicians have much to learn and much to contribute to the assessment and management of both patients with this group of diseases and their everyday caregivers.
All new developments in Alzheimer's disease are detailed in the text, including amyloid-targeted neuroimaging, biomarkers, and anti-amyloid therapies. The diagnostic schedules for Alzheimer's disease and other forms of dementia have been updated to comply with the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5).
Part I
Another challenge is that the informant, if present, can demonstrate something of the same relationship as the patient. This introduction should always include your name, title, specialty and the purpose of the interview. The very appearance of the patient (grooming and dressing, walking, motor activity and facial expressions) together with his attitude towards the interviewer and the content of the interview give clues to the current condition and diagnosis.
In the MSE of the dementia patient, it is important to distinguish between real delusions or hallucinations and confused thoughts, as the following vignette illustrates. An important benefit of functional testing is that it helps to involve both the patient and carers in a discussion of the patient's remaining strengths and weaknesses in the face of dementia. Such information can pit family members or caregivers against the disabled individual or against each other - the last situation any clinician wants to create.
One of the most popular functional tests is the Instrumental Activities of Daily Living (IADL) scale. If there is a discrepancy (ie, the neuropsychologist suggests a diagnosis of AD, but the clinician is convinced that it is dementia with Lewy bodies), a discussion with the examiner is warranted.
Part II
Other similar terms that have appeared in the scientific literature include age-related cognitive decline (Levy, 1994) and cognitive impairment without dementia or CIND (Lyketsos et al., 2006). Other research has linked anticholinergic body load with an increased risk of delirium (Flacker et al., 1998). Physical exercise can also increase the release of nerve growth factors such as BDNF (Swardfager et al., 2011).
A Mediterranean diet includes many of these factors and has been found to reduce the risk of AD (Scarmeas et al., 2006). Imaging of AD patients using positron emission tomography (PET) has demonstrated consistent patterns of symmetric hypometabolism in posterior cingulate and parietotemporal brain regions ( Small et al., 2008 ). A schematic of the pathological process of AD involving biomarkers is illustrated in Figure 4.3 (based on Sperling et al., 2011).
Clioquinol has been shown to reduce Aβ deposits in transgenic mice but also induce myelinopathies in the central nervous system ( Zhang et al., 2013 ). Long-term follow-up of AN1792 antibodies showed reduced functional decline (Vellas et al., 2009). These occurrences are visualized on MRI scans and are usually not associated with clinical symptoms (Tayeb et al., 2013).
In one study, lithium reduced both tau hyperphosphorylation and insoluble tau aggregation in the brains of transgenic mice (Noble et al., 2005). One study found that curcumin could inhibit the accumulation of beta-amyloid in the brains of transgenic mice (Yang et al., 2005). However, there is no direct evidence suggesting a therapeutic role in AD in humans (Begum et al., 2008).
Dementia with Lewy bodies 99 locus coeruleus and nucleus basalis according to Meynert (Zaccai et al., 2008). Cognitive-enhancing drugs such as acetylcholinesterase (AChE) inhibitors are recommended for the treatment of cognitive impairment (Neurobehavioral Guidelines Task Force et al., 2006). Recent guidelines suggest describing the diagnosis as probable, possible, or unlikely NPH based on the range of symptoms (Marmarou et al., 2005).
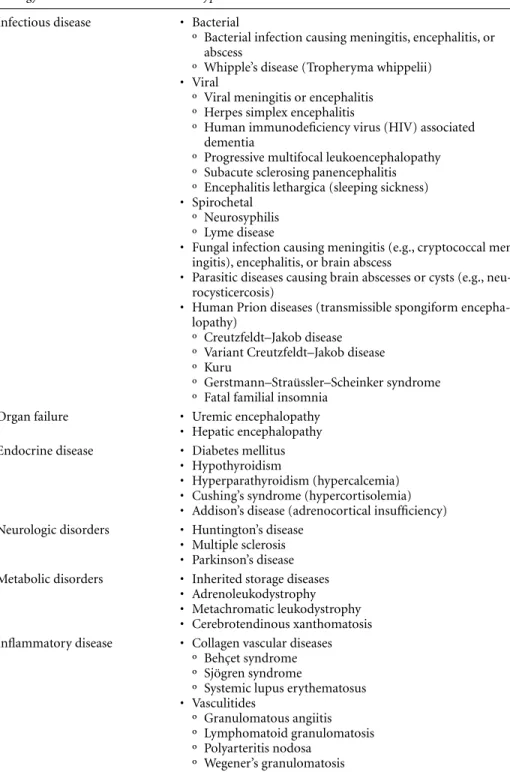
Cumulative lead exposure has also been associated with increased cognitive impairment in Parkinson's disease (Weuve et al., 2013). Dementia Associated with Medical Conditions 131 disorders, ataxia, peripheral neuropathy, and parkinsonism (Chuang et al., 2007; Liu et al., 2012). MRI scans of the brain may show basal ganglia hyperintensity on T2-weighted images (Cambier et al., 2003).
Hepatic encephalopathy is characterized by confusion, asterixis, ataxia, hyperreflexia, mood disturbances and psychosis (Cash et al., 2010).
Part III
Various forms of agitation are seen in 80% to 90% of dementia patients during the course of the underlying disease, with higher rates in more severe dementia and in nursing homes (Ballard et al., 2001; International Psychogeriatric Association, 2000). Although these symptoms may be present early in the course of dementia, their frequency and intensity usually peak in the moderate stages of dementia and then begin to decline as the individual enters the more severe stages. A better description might be something like "the patient is an 80-year-old man with Alzheimer's who slaps the nurses with his hands when they try to give him a bath in the morning," or "the patient is a 75-year-old woman with dementia from a stroke who after a meal he screams incoherently.” These examples enable the second goal of treatment, which is to identify possible causes of agitation.
For example, when a patient insists that he or she has seen a deceased loved one, this may reflect an actual visual hallucination, a delusion of mistaken identification (i.e., the false, fixed belief that another person is the deceased loved one ), or simply agnosia (impaired recognition) related to the dementia itself (eg, an unknown person is mistaken for a familiar one, perhaps because of similar physical characteristics or because the misidentified person's death is forgotten). The precise description of the problematic behavior - the operational definition described earlier - obtained during the assessment allows treatment to be directed at the source of the problem. Individual psychotherapy as part of the behavior plan may be helpful, depending on the degree of dementia.
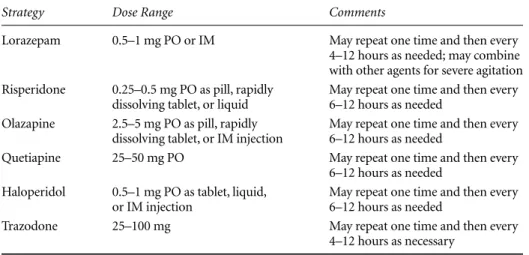
Think about the patient and the situation and ask yourself some of the following basic questions: What does the patient need. Nevertheless, the FDA required that the warning be added to the package insert of the corresponding drugs. Risperidone is one of the atypical drugs with the least sedative effect, but poses a risk of EPS.
The behavioral emergency approach represents an accelerated, more intensive version of the normal assessment and treatment of agitation and psychosis. The combination of two or more antipsychotics or more benzodiazepines should be avoided because of the increased risk of adverse effects. Presented at the 16th Annual Meeting of the American Geriatric Psychiatric Association, Honolulu, Hawaii.
Are cholinesterase inhibitors effective in managing the behavioral and psychological symptoms of dementia in Alzheimer's disease. Depression, anxiety and apathy are some of the main psychiatric problems associated with dementia. In vascular dementia, depression is more common after damage to left frontal and right parietal regions of the brain (Robinson et al., 1983).