Although the case histories are taken from actual cases, every effort has been made to conceal the identity of the individuals involved. The cerebellum has the most neurons of any part of the brain and interacts with all parts of the brain.
Acknowledgments
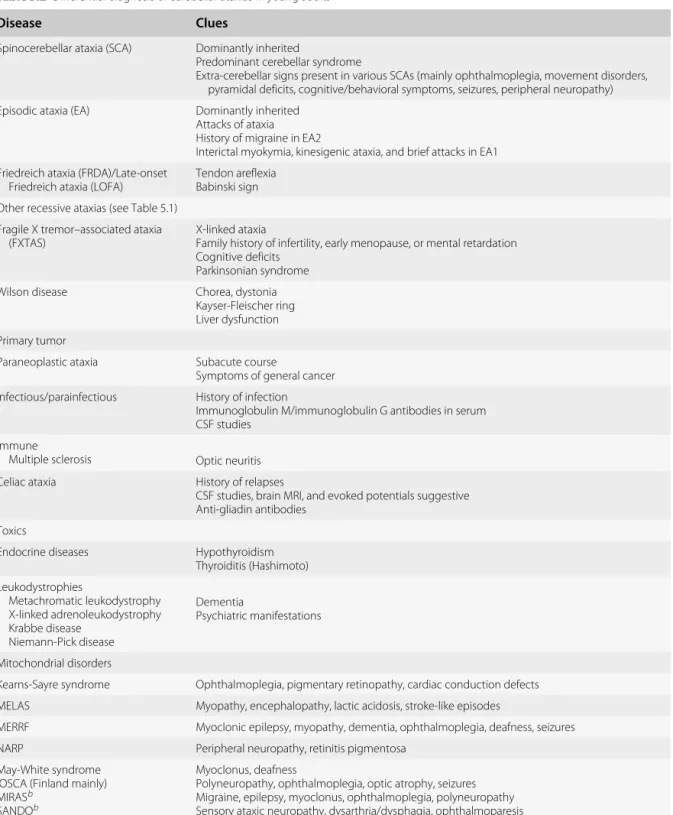
The terminology for cerebellar ataxias encompasses a wide range of disorders. Advances in neuroimaging, advances in translational neuroscience, recent discoveries in molecular biology, and the availability of genetic testing have revolutionized the field of cerebellar disorders. Diagnosis and general treatment of cerebellar ataxias are discussed in chapters 5 and 6 respectively. The following chapters discuss the sporadic forms and hereditary diseases encountered in daily practice.
Embryology
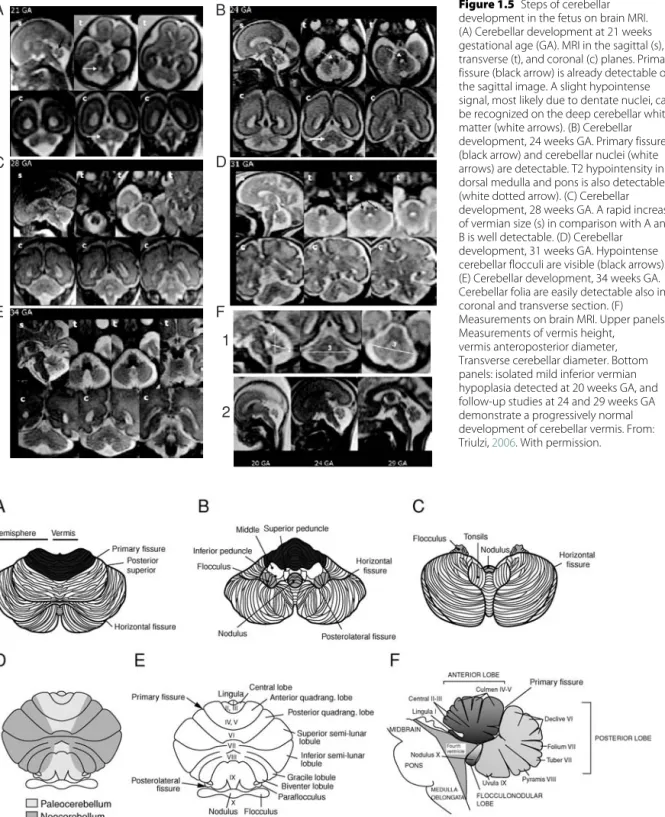
Embryology and anatomy
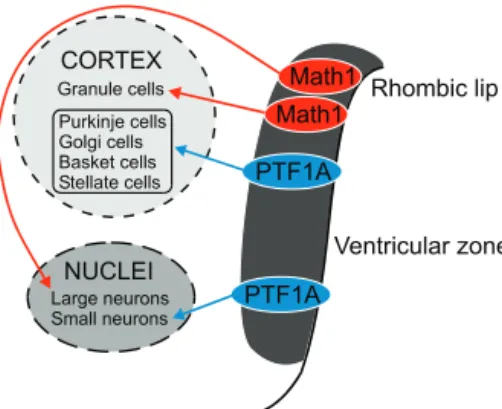
The Math1 gene encodes a transcription factor specifically expressed in the precursors of the EGL and is required for granule cell lineage (Ben-Arie et al., 1997). PTF1A (pancreatic transcription factor 1A) is implicated in the generation of cerebellar GABAergic neurons (Hoshino et al., 2005).
Anatomy Nomenclature
Top panels, crown sections; lower left, parasagittal section; lower right, inferior view of the cerebellum. Purkinje neurons inhibit the cerebellar nuclei, which are the origin of the output from the cerebellum.
Cerebellar nuclei
In other words, a small area in the inferior olive is connected to a certain area of output of the cerebellum. Cerebellar stimulation of the fastigial nucleus triggers responses in the hippocampus and amygdala (Heath & Harper, 1974).
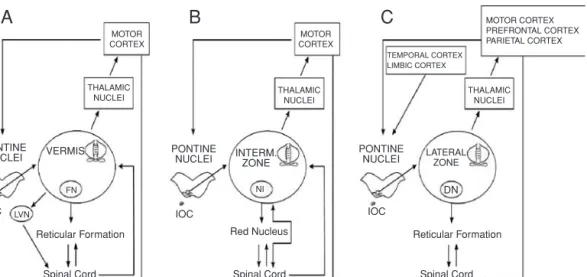
The three functional divisions
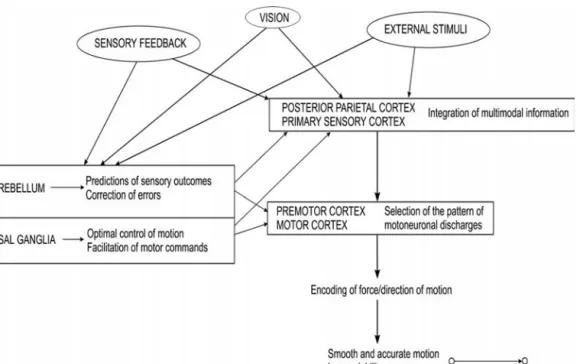
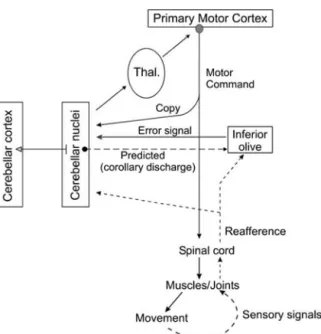
The output of the cerebellum is directed to all components of the motor systems, except the basal ganglia. It regulates the activities of voluntary muscles, coordinating the timing, duration and magnitude of muscle discharges. The cerebellum is involved in planning activities, learning new motor skills, and updating previously acquired motor schemas.
Activities in the cerebellar nuclei
Physiology of the cerebellum
The midline area and intermediate area receive direct information from the spinal cord, unlike the lateral cerebellum.
Activities of Purkinje neurons
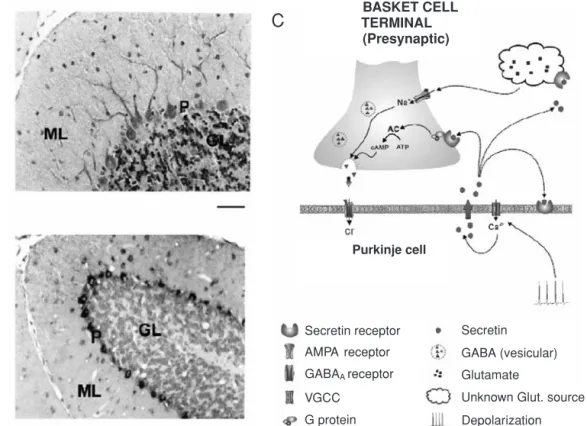
Stimulation of parallel fibers alone can trigger a long-term potentiation of the synapse parallel fiber/Purkinje neuron.
Activities of the inferior olivary complex
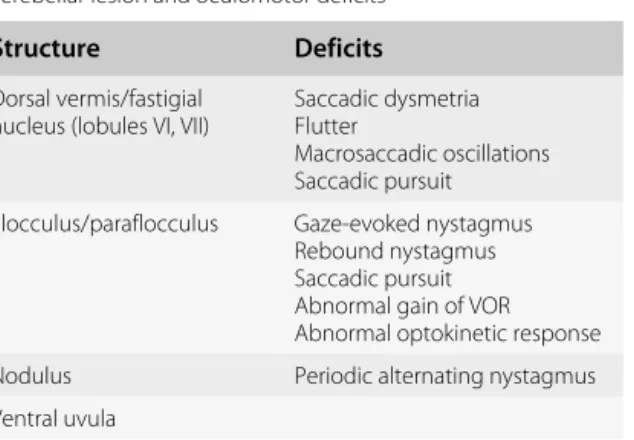
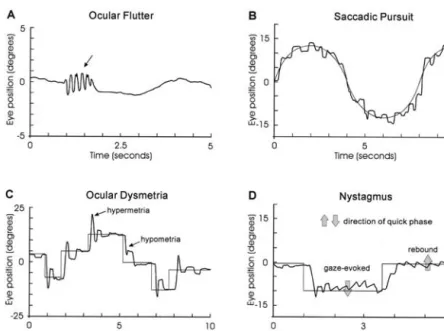
Control of eye movements
Control of speech
A preparatory loop includes the supplementary motor area, the dorsolateral frontal cortex including Broca's area, the anterior insula, and the superior cerebellum. The executive loop includes the sensorimotor cortex, basal ganglia, thalamus, and the inferior cerebellum.
Control of limb movements
Posture and gait
As for the posterior cerebellar vermis, it may control the coordination of bilateral leg movements (Bastian et al., 1998). The LLRs are involved in the stabilization of postural activities in the four limbs and contribute to postural stability. The cerebellum controls the M2/M3 components of LLRs ( Friedemann et al., 1987 ).
Learning
One paradigm used to estimate the adaptation of motor learning in arm movements is the following (Deuschl et al., 1996): the subject stands in front of a screen showing a target that repeatedly moves between two positions. to match a ballistic movement of the elbow (or hand) to the target (or to match the isometric force during a pinch task). Errors typically show exponential learning curves during adaptation. The number of trials required to adapt to the new condition is higher in cerebellar patients.
Sensory” processing
Mossy fibers originating from the pontine nuclei carry CS information, while climbing fibers originating from the inferior olive carry US information in the cerebellum. Excitability changes occur in cerebellar neurons that receive input from the CS mossy fibers and US climbing fibers, both in the cerebellar cortex (for example, long-term depression - LTD - of parallel fiber-Purkinje cell synapses) and in nuclei.
Cerebellum and timing
The net effect of plasticity in these two areas is increased activity in the nucleus interpositus, which may be able to drive activity in brainstem neurons that control eyeblinking.
Computational models of cerebellar function
Sensorimotor latencies vary by modality and context and can range from 50 to 400 msec. The cerebellum has been suggested to contain the neural representations or "internal models" to mimic fundamental natural processes such as body movement (Ramnani, 2006). This theory is supported by fMRI studies, transcranial magnetic stimulation (TMS) experiments and psychophysical studies. Some of the most compelling evidence that the CNS uses internal feedforward models in human motor behavior comes from studies dedicated to the control of grasping forces during object manipulation ( Nowak et al., 2007 ). The rate of grip force development and the balance between grip and load forces when grasping/lifting an object are programmed to meet the demands due to physical object properties, such as weight, surface friction, or shape.
Cerebellum and cognitive operations
Although studies of the changes in Purkinje cell firing that occur when an external force load is changed from resistive to assistive during elbow movements suggest an inverse dynamics model, it should be noted that these experiments did not control limb kinematics or change the magnitude of external loads (Yamamoto et al., 2007). Two of the differences between cerebellar simple spike responses and those of motor cortical cells are the non-uniform distribution of preferred directions and the extensive overlap in the timing of the correlations. These differences suggest that Purkinje cells handle kinematic information differently compared to motor cortical neurons.
Cerebellum, mood, and depression
Liu Y, Pu Y, Gao JH, et al. Human red nucleus and lateral cerebellum supporting roles for sensory information processing. Hum Brain Map. Cerebellar symptoms are influenced more by the location and rate of disease progression than by pathologic features (Gilman et al., 1981; Lechtenberg, 1993).

Ataxia: definition
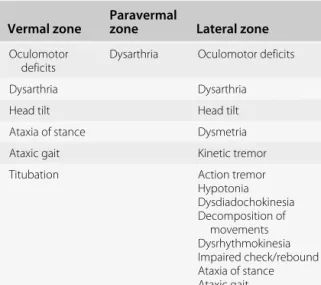
Clinical signs and sagittal zone affected
Classification of clinical signs
Symptoms of cerebellar disorders
In particular, cerebellar ganglioglioma may be associated with paroxysmal facial contractions (Chae et al., 2001). Similar symptoms can be observed in children with hamartoma of the floor of the fourth ventricle (Delande et al., 2001).
Lesion–symptom mapping
Recovery after lesions of the cerebellar nuclei is often less complete (Eckmiller & Westheimer, 1983). Schmahmann JD, Weilburg JB, Sherman JC. The neuropsychiatry of the cerebellum: insights from the clinic. Cerebellum.
ICARS
Clinical scales
Hand rests on the knee before the beginning of the movement. Three movements of each limb are performed under visual guidance. Abnormalities of the eye pursuit: the subject is asked to follow the slow lateral movement performed by the examiner's finger.
BARS (Brief Ataxia Rating Scale)
Dysmetria of saccades: the index fingers of the examiners are placed in each temporal visual field of the patient, whose eyes are in the primary position. The patient is asked to look laterally at the finger on the right and left. The average overshoot or undershoot of the two parties are estimated. The interrater correlation is very high for the total score, and high to very high for each subscore of the component (Storey et al., 2004). The scale is sensitive to a range of forms of ataxia, from mild to severe.
AS20 (Ataxia Scale on 20 points)
The ICARS is a reliable scale that meets accepted criteria for interrater reliability, test-retest reliability, and internal consistency (Schmitz-Hubsch et al., 2006a). The ICARS is also useful in extracting and assessing the severity of cerebellar signs in multiple system atrophy, although it is contaminated by parkinsonian features (Tison et al., 2002).
SARA (Scale for Assessment and Rating of Ataxia)
Support of feet and torso allowed if necessary. The subject is asked to repeatedly point his index finger from his nose to the experimenter's finger, which is located in front of the subject at approximately 90% of the subject's reach. Support of feet and torso allowed if necessary. The subject is asked to perform 10 cycles of repeated alternations of pronations and supinations of the hand on his/her thigh as quickly/accurately as possible.
Comparison between scales
Heel-shin shift: each side is assessed. The subject lies on the examination bed, without a view of his legs. The subject is asked to lift one leg, point the heel towards the opposite knee and slide along the shin bone to the ankle and place the leg back on the examination bed. The task is executed three times. The SARA score is closely correlated with the Barthel Index, which is widely used to estimate activities of daily living. The score correlates poorly with disease duration, and the scale presents some difficulties in detecting the early stages of cerebellar ataxia.
Quantitative tests
If the subject slides and shines without contact in all three attempts, the rating is 4.
FARS (Friedreich Ataxia Rating Scale)
Place markers 25 feet apart for walking. The patient walks a distance, turns around and returns, and the activity is timed. Tandem position (use a stopwatch; three attempts, dominant leg in front; time in seconds. Three attempts are made and the average is recorded.).
Unified Multiple System Atrophy Rating Scale (UMSARS)
Development of a brief ataxia rating scale (BARS) based on a modified form of ICARS.Mov Disord. Reliability and validity of the International Cooperative Ataxia Rating Scale: a study in 156 spinocerebellar ataxia patients. Mov Disord2006a;21:699-704.
The importance of obtaining a detailed genealogy
The role of brain imaging
Diagnosis of cerebellar disorders as a function of age
Blood studies
Which cutoff for age?
Congenital and childhood disorders
Most children show head growth retardation from 4 to 6 months of age, and visual disturbances begin around 3 years of age. Another metabolic disorder that should not be overlooked in early childhood is the Glut1 deficiency syndrome, a potentially treatable disorder.
Ataxias in young adults
Cerebral folate deficiency is associated with low cerebrospinal fluid (CSF) 5-methyltetrahydrofolate (the active metabolite of folate) in the presence of normal folate metabolism outside the nervous system (Ramaekers & Blau, 2004). Clinical features typically include motor and intellectual delay, seizures, head growth retardation, and movement disorders with ataxia, dystonia, and spasticity (Brockmann, 2009).
Ataxia in the elderly
L-2-hydroxyglutaric aciduria presents with cerebellar ataxia associated with pyramidal signs, mental decline, seizures, and macrocephaly. The acronym ILOCA refers to an idiopathic late-onset cerebellar ataxia associated with cerebellar atrophy on MRI. The diagnosis is retained when the other causes of cerebellar atrophy have been ruled out.
Genetic testing
Early-onset ataxia with oculomotor apraxia and hypoalbuminemia is caused by mutations in a novel HIT superfamily gene.Nat Genet. Readers are also referred to the corresponding chapters for more details regarding the specific management of a given disorder.
Medical treatment
Overview of the general management of cerebellar disorders
Surgery
Rehabilitation and assistive therapy
Cerebellar ataxia Amantadine (release of dopamine and modulation of NMDA pathway) 50-300 g/day Buspirone (5-HT1A agonist) 10-60 mg/day. Baclofen (GABA-B receptor agonist) 20–80 mg/day Memantine (uncompetitive NMDA antagonist) 5–20 mg/day Abbreviations: GABA: gamma-aminobutyric acid; NMDA: N-methyl-D-aspartic acid.
Treatments under investigation
Social workers and psychologists should be integrated in the discussion about therapeutic procedures, especially in chronic disorders of the cerebellum.
Classification of cerebellar malformations
Malformations of both midbrain and hindbrain
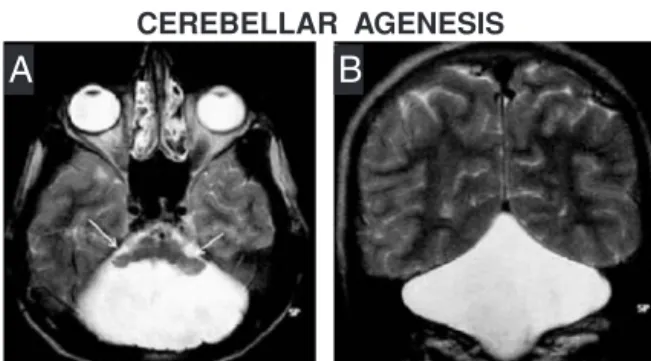
Malformations
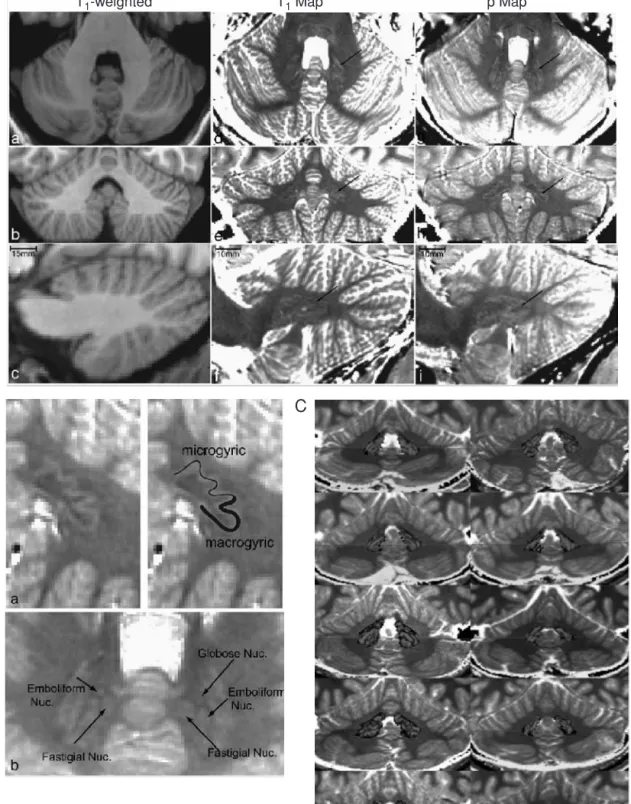
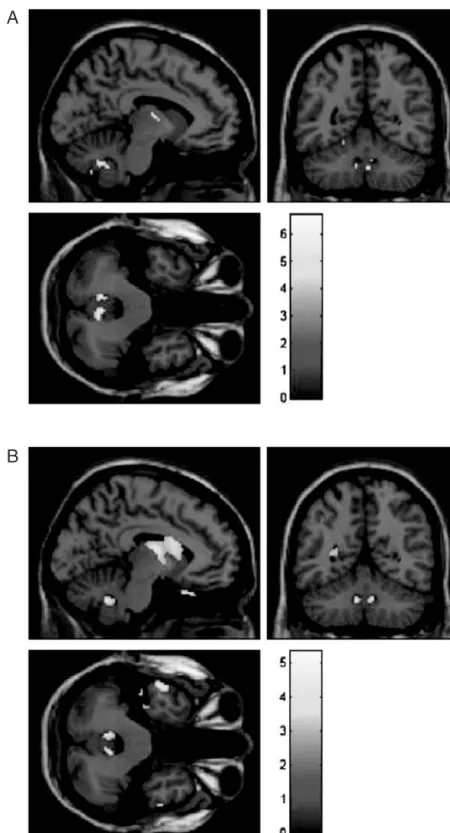
Rhombencephalosynapsis is characterized by the absence of the vermis or severe dysgenesis of the midline structures of the cerebellum. Inferior vermic agenesis, fusion of the inferoposterior parts of the cerebellar hemispheres (arrow in left panel) and dysplasia of the superior vermis (short arrows in right panels).
Malformations predominantly affecting the cerebellum and
Prenatal diagnosis of Dandy-Walker malformation and cerebellar vermis hypoplasia/dysplasia can be problematic. Tectocerebellar dysraphia has features that overlap with those of Dandy-Walker malformation, Chiari II malformation, and posterior fossa ventriculocele.
Malformations predominantly affecting the lower hindbrain
Paradoxically, a mild dilatation may be associated with a worse prognosis than a classic Dandy-Walker malformation associated with a large dilatation. Surgical treatment of Dandy-Walker malformation involves diverting the CSF from the ventricular space or the cystic space to another location, such as the peritoneal cavity.
Developmental abnormalities with fluid collections
Possible associated findings include hydrosyringomyelia, possibly due to the transmission of increased pressure in the spinal cord, and a progressive scoliosis (Oldfield et al., 1994). Aplasias of cranial nerves VI and VII are associated with lateral gaze deficits and facial nerve palsy.
Prenatal–onset degeneration
Isoelectric focusing of serum sialotransferrin shows an abnormal glycosylation of this glycoprotein in type I CDG (Stibler et al., 1998). However, ataxic patients may demonstrate unequivocal cerebellar hypoplasia but a normal or slightly abnormal transferrin isofocusing result (Vermeer et al., 2007).
Other malformations and syndromes Lhermitte-Duclos syndrome
Several mutations have been identified, in particular R141H – the Danish population has a high carrier frequency of this mutation – and F119L of the PMM2 gene located on chromosome 16p13 (Matthijs et al.,1997; Kjaergaard et al.,2001). . Barth PG, Blennow G, Lenard HG, et al. The syndrome of autosomal recessive pontocerebellar hypoplasia, microcephaly, and extrapyramidal dyskinesia.
Anatomy of cerebellar vessels
The venous drainage of the cerebellum is characterized by relatively large zones of venous return and anatomical variations between subjects. Three main groups of arteries are identified: the superior or Galenic group, the anterior or petrosal group, and the posterior or tentorial group. group (Figure 8.3). The superior group drains the upper brainstem and the superior portion of the cerebellum. The superior cerebellar vein reaches the great cerebral vein of Galen. The anterior group drains the anterior parts of the brainstem and cerebellum. The veins of this group mostly empty into the superior petrosal vein near the pons (Braun et al., 1996). The posterior group drains the lower parts of the cerebellar vermis and medial parts of the cerebellar hemispheres.
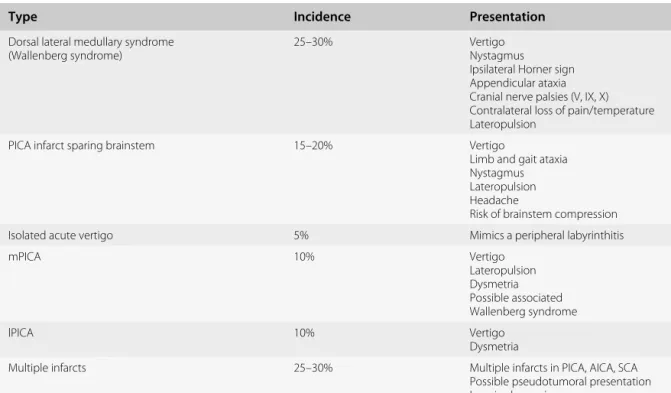
Cerebellar infarctions
Cerebellar stroke
Small deep infarcts are located either in the border zone of the AICA and side branches of PICA territories, or between the vermal branches of the two SCA arteries. Patients often present with sensory deficits and varying degrees of pain depending on the location of the stroke.
Pathogenesis of cerebellar infarcts
Patients with a thalamic infarction in the territory of the posterior choroidal artery involving the posterior thalamic nuclei may develop complex delayed hyperkinetic motor syndromes, combining ataxia, tremors, dystonia, myoclonus and chorea (“dystonic unsteady hand”) (Ghika) al., 1994). Aspergillosis can involve the vessels of the posterior circulation, occluding the distal branches of the cerebellar arteries and leading to infarction or hemorrhage (Walsh et al., 1985).
Cerebellar hemorrhage
Lipohyalinosis affects small penetrating branches in the brainstem, closing the lumen of the vessel as a result of subintimal proliferation. The zebrafish-like pattern of distant cerebellar hemorrhage with a typical striated, curvilinear bleeding pattern is located in the upper cerebellar foramen.
Cerebellar vein thrombosis
Also note the small hemorrhage in the interhemispheric fissure (interpreted as related to acute loss of cerebrospinal fluid). C) CT scan of a patient who underwent resection of a Pancoast tumor with subsequent insertion of a thoracic aspiration drain. Remote cerebellar hemorrhage is a rare complication of supra-tentorial, thoracic, or lumbar spine surgery (Brockmann & Groden, 2006).
Diagnosis of cerebellar stroke
Isolated venous angiomas of the posterior fossa are common and are very often asymptomatic. They are managed conservatively. Monitoring of intracranial pressure Surgical removal of the lesion if necessary Endovascular thrombolysis in selected cases Antibiotics in case of infection.
Treatment of cerebellar stroke
A decision-making algorithm was proposed for vertebral artery aneurysm dissection (Iihara et al., 2002). Multimodal therapy (combinations of radiosurgery, surgery and endovascular techniques) of arteriovenous malformations of the posterior fossa is associated with a better clinical outcome (Kelly et al., 2008).
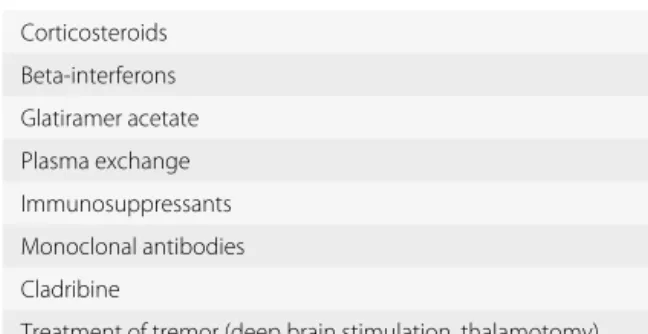
Multiple sclerosis
Immune diseases
T2-weighted images of the optic nerve usually show a hyperintense lesion in optic neuritis, and gadolinium enhancement is seen in an acute attack (Kolappan et al., 2009). An advantage of stimulation of the nucleus of the zona incerta may be to improve the proximal components of tremor (Plaha et al., 2008).
Ataxia with anti-GAD antibodies
Celiac disease and gluten ataxia
Concomitant autoimmune disease is not unusual (especially Hashimoto thyroiditis, type 1 diabetes mellitus and pernicious anemia) (Hadjivassiliou et al., 2008). Post-mortem studies have provided evidence of neuroinflammation in the cerebellum and posterior columns (Hadjivassiliou et al., 2002).
Other immune disorders affecting the cerebellum
Multiple infarcts in the vertebrobasilar region may be the first manifestation (Kwon et al., 1999). Antibodies directed against Purkinje cells have been reported in patients with lupus ataxia (Shimomura et al., 1993).
Thyroid disorders
Endocrine disorders
One difficulty is that these antibodies can be detected in elevated titers in the general healthy population (Mocellin et al., 2007). High-dose methylprednisolone (1 g/day for 5 days) is recommended in cases of encephalopathy (Shaw et al., 1991).
Parathyroid disorders
Cerebellar ataxia and diabetes
Cerebellar ataxia and hypogonadism
Autoimmune thyroiditis and a rapidly progressive dementia: global hypoperfusion on SPECT scan suggests a possible mechanism. Neurology. High prevalence of serum autoantibodies to the amino terminus of alpha-enolase in Hashimoto's encephalopathy.
Bacterial infections
Infectious diseases
Cerebellitis
Autoantibodies against glutamate receptor delta 2 (mainly expressed in the cerebellum) have also been reported (Shimokaze et al., 2007). Cerebellitis can mimic a tumor on brain imaging (pseudotumoral presentation). The lesion can be unilateral (Amador et al., 2007).
Human prion diseases
Dopamine transporter SPECT shows putaminal dopaminergic presynaptic changes in sporadic CJD (Ragno et al., 2009).
Clinical features
Brain imaging
Neurophysiology
Neuropathology
Corticobasal degeneration
Differential diagnosis
Treatment
Both schwannoma and meningioma occur in type 1 (von Recklinghausen's disease) – usually diagnosed in the first decade – or in type 2 neurofibromatosis – usually diagnosed between 18 and 40 years of age. Headaches tend to be localized in the occipital region and are exacerbated by coughing or the Valsalva maneuver.
Medulloblastomas
Tumors and paraneoplastic disorders
Medulloblastoma is associated with a deregulation of the sonic hedgehog pathway (see Chapter 1) (Wetmore, 2003; Ferretti et al., 2008).
Cerebellar astrocytomas
Brainstem gliomas
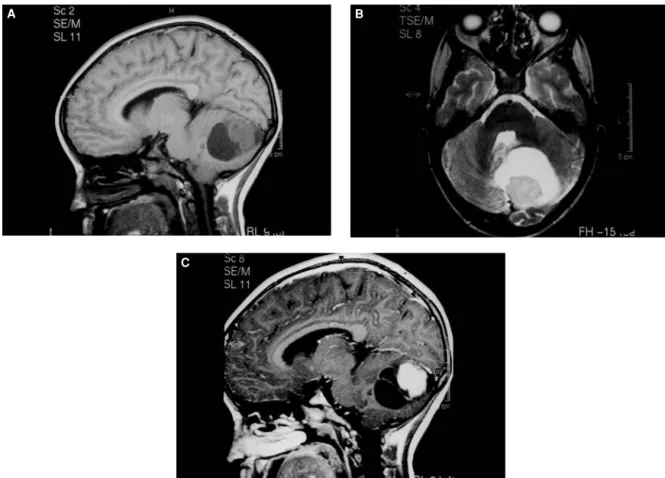
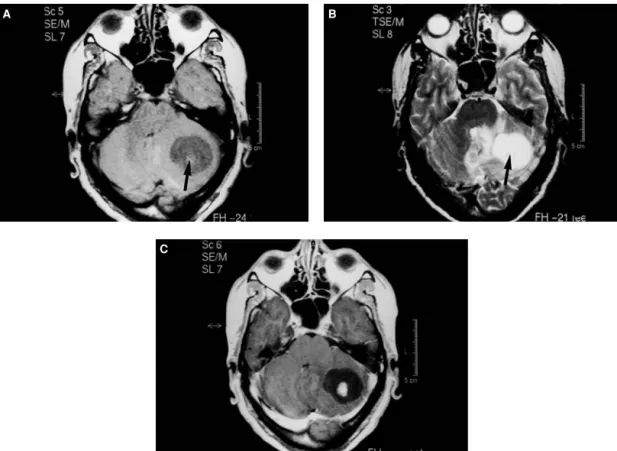
Brainstem involvement, fourth ventricle invasion and radiation dose to the posterior fossa and the spine are prognostic factors. The 10-year overall survival rate is 50% to 55%. Post-contrast T1-weighted image shows enhancement of the solid component, also observed in the cyst wall (C).
Hemangioblastomas
Ependymomas
Meningiomas
Extensive skull base meningiomas should not be misinterpreted as idiopathic hypertrophic pachymeningitis (IHPM) (Rudnik et al., 2007). MRI shows thickening of the skull base pachymeninx compressing the lower brainstem, with the presence of contrast enhancement.
Schwannomas (neurinomas)
However, approximately 5% of patients require surgical resection after radiosurgery, in the presence of increased intracranial pressure or cerebellar ataxia (Iwai et al., 2007). These operations are complicated by fibrosis and adhesions between the tumor and surrounding tissues (Lee et al., 2003).
Epidermoid and dermoid tumors
When surgery is performed during the transient swelling period, surgical outcomes are poor in terms of preservation of cranial nerve function, particularly facial nerve function (Iwai et al., 2007). In patients with tumor enlargement several years after radiosurgery, the possibility of chronic intratumoral bleeding due to delayed radiation injury should be considered (Iwai et al., 2007).
Primary lymphomas of the CNS
Swelling usually peaks about 6 months after radiosurgery, but may persist for up to 2 years and may not respond to steroids. Close follow-up in very elderly patients with slow-growing tumors and mild deficits may be an alternative.
Lhermitte-Duclos disease
Cerebellar metastases
These characteristics help achieve highly conformal dose distributions with minimal damage to surrounding tissues (Wadasadawala et al., 2007). It should be taken into account that death in half of the patients is due to systemic cancer lesions.
Complications of chemotherapy, phenytoin, lithium salts
Open microneurosurgery with resection should be considered when the lesions appear removable and there is an expected survival of 6 months or more (Hildebrand & Bal´eriaux, 2002). Radiation therapy (usually 30 Gy in 10 fractions) is recommended, both in patients undergoing surgery and those in whom the metastases are not removed.
Superficial siderosis
This assumes that the primary cancer is under control. The high rate of postoperative complications is quite typical for metastatic disease of the posterior cranial fossa, especially because a small hematoma in the posterior fossa leads to neurological deterioration requiring a reintervention (Pompili et al. ., 2008). Indeed, small metastases are good targets for stereotaxy. They are often well-defined with distinct contrast-enhancement borders and have a displacement rather than infiltrative effect, unlike gliomas.
Stroke
Infections
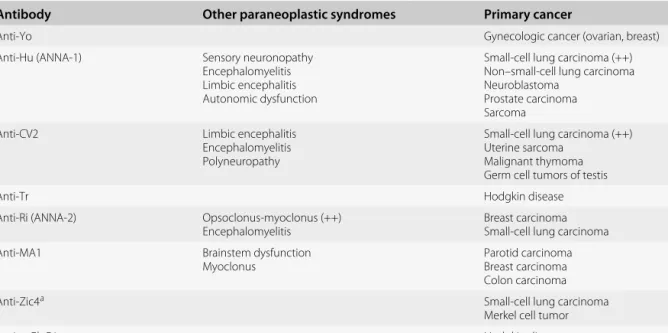
Paraneoplastic cerebellar degeneration
Follow-up brain scans may demonstrate cerebellar atrophy despite stability or even mild improvement in neurological status (Figures 13.10 and 13.11). Prompt treatment of the primary cancer (tumor resection, radiation and/or chemotherapy, depending on the cancer) can in some cases halt the progression of PCD.
Langerhans histiocytosis
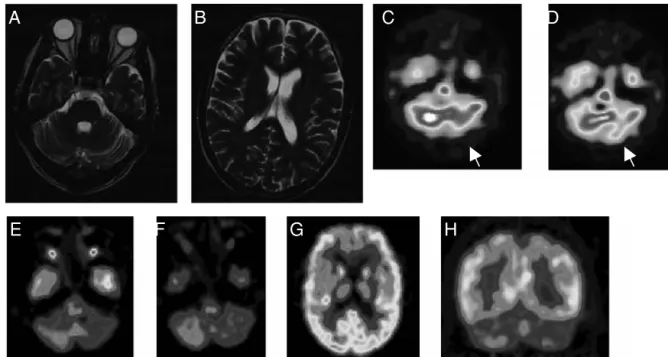
FDG-PET scan and single photon emission CT can reveal cerebellar hypermetabolism and increased regional perfusion in the acute stage of the disease due to the inflammatory response (Choi et al., 2006). An exciting butterfly aspect of the dentate nuclei can be observed on coronal images (Martin-Duverneuil et al., 2006).
Erdheim-Chester disease
In other cases, ataxia is associated with histiocytic infiltration of the pons and middle cerebellar peduncles (Evidente et al., 1998). Healey EA, Barnes PD, Kupsky WJ, et al. The prognostic significance of postoperative residual tumor in ependymoma. Neurosurgery.
Clinical presentation
Penetrating injuries or fractures usually cause liquorrhea in open head injuries (Maschke et al., 2002). The vertebrobasilar system may be involved with dissection of the vessels and secondary infarction (see also Chapter 8). Indeed, trauma to the posterior fossa is a potential cause of death, especially in children, young adults, and the elderly.
Types of trauma
Trauma of the posterior fossa
Occlusion of the blood vessel lumen, arterio-arterial embolism, may result, possibly leading to a cerebellar stroke (Figure 14.5). Traumatic dissection of the vertebral arteries is more common than dissection of the carotid arteries (Reid & Weigelt, 1988).
Investigations
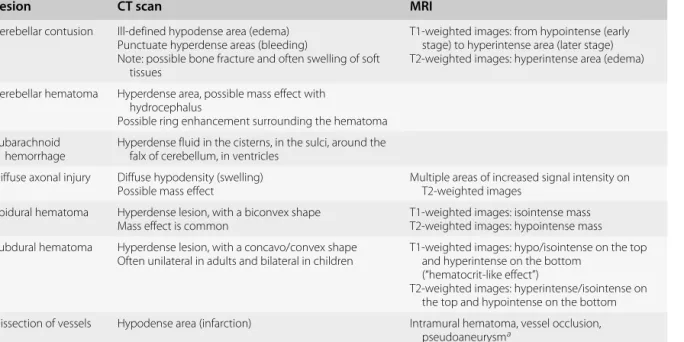
Subdural hematoma in the posterior fossa with collection of blood between the arachnoid and the meningeal layer of the dura is relatively rare in traumatic brain lesions. A clear interval between the trauma and the clinical deficits usually lasts a few hours and occurs in up to half of the patients. The hematoma appears biconvex (figure 14.4).
Management
Late complications
Triangles indicate a fracture of the right temporal bone extending to the sulcus of the sigmoid sinus. Mood disturbances and neuropsychological deficits may occur, developing several months to a year after injury to the posterior fossa.
Cerebellar toxicity of alcohol
Toxic agents
Prenatal exposure (fetal alcohol syndrome) may be associated with atrophy of the anterior region of the vermis (lobules I through V), sparing lobules VI through X (Sowell et al., 1996). Hypometabolism in the superior cerebellar vermis is associated with decreased cellular and synaptic activity due to neuronal loss (Gilman et al., 1990).
Drugs
Other toxic agents may add to cocaine and participate in neurological deficits (Katz et al., 1993). Phencyclidine is a non-competitive antagonist of NMDA receptors with neurostimulatory properties (Deutsch et al., 1998).
Environmental causes of cerebellar ataxia
Experimental studies have shown that carbon monoxide induces impairment of the differentiation of cerebellar GABA-synthesizing neurons (Benagiano et al., 2005). PCBs cross the placenta and are transferred to newborns via breast milk (Nguon et al., 2005).
Animal-related cerebellar toxicity Scorpions
Experimental studies show that perinatal exposure to PCBs is associated with impaired cerebellar development and abnormal motor behavior (Nguon et al., 2005). Cerebellar deficits may be predominant, hence the terminology of ataxic shellfish poisoning (Rhodes et al., 1975).