The present publication aims to provide an up-to-date overview of the epidemiology of chronic liver disease worldwide. We hope that this review will provide the reader with an updated worldwide perspective of the clinical epidemiology of chronic liver disease.
Defining a Population for Clinical Epidemiology Studies It is not feasible to study the entire population to evaluate an exposure-outcome
Defining Exposure
Defining Outcome
Descriptive Epidemiology
Analytic Epidemiology
The risk or speed of developing the result is estimated from that point forward, similar to a prospective study. However, if the investigators could obtain this information about cases and controls from another source, such as the medical record, before the outcome occurred, then the potential for recall bias is reduced.
Measures of Association
Information on aspirin use in NHANES III was limited to the month before study entry. This is especially important because any potential protection against liver fibrosis is likely to require long-term aspirin use.
Some Notes About Statistical Inference (p-Values and Confidence Intervals)
Bias
Confounding
For example, in the cross-sectional study of aspirin use and liver fibrosis described earlier [5], unadjusted results showed a modest inverse association in patients with chronic liver disease that was not statistically significant at the alpha = 0.05 level. (CI coefficient - 0.41 to 0.07; p-value 0.2; see Table 1.1). Interestingly, in this study, age was the most important confounder, and after adjusting for age, the inverse association between aspirin use and liver fibrosis was strengthened (Coefficient CI -0.47 to -0.07; p-value 0.008).

Selection Bias
Misclassification
Relatively cheap, easy and fast; often generalizable: provides valid estimates of the prevalence of risk factors and outcomes. Measure risk factors in an outcome-free cohort and observe them until they develop the outcome.
Generalizability
Understanding Study Design for Clinical Epidemiology Studies
- Overview of Chapter
- Case Control Study
- Overview
- Randomized Controlled Trial
- Overview
- Cohort Study
- Overview
A confounder is a factor associated with the exposure of interest and possibly also a cause of the outcome of interest. You are aware that angiosarcomas are associated with vinyl chloride, but are unsure of the association between vinyl chloride and HCC.
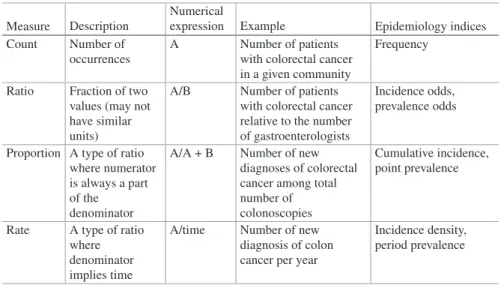
Understanding the Interpretation of Disease Incidence and Prevalence
- Frequency Data
- Incidence
- Cumulative Incidence (Incidence Proportion)
- Incidence Density (Incidence Rate)
- Incidence Odds
- Prevalence
- Point Prevalence
- Period Prevalence
- Prevalence Odds
- The Relationship Between Incidence and Prevalence
- Reporting Incidence and Prevalence
Incidence” describes the number of new individuals meeting the case definition (e.g. the disease in question) among the total population at risk within a certain period. The numerator for this measure is the number of cases at a given point in time (both existing and new), while the denominator is the total population at that same point in time.
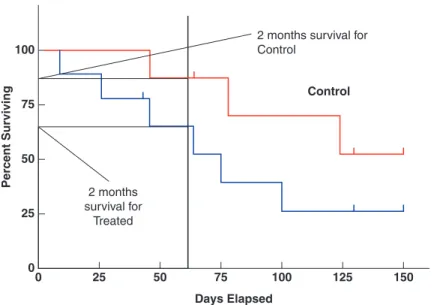
Understanding Survival Analyses
Introduction
- What is Survival Analysis?
- Why Measure Survival Analysis?
Survival analysis is widely used in epidemiological studies to measure the effect of a particular intervention on the long-term outcomes of the study population. Survival analysis is used in almost all phase III and most phase II clinical trials to provide information about the effectiveness of the drug, device, or procedure being studied.
Basics and Definitions .1 Censoring
- Distribution of Survival Data
- Survival Probability and Hazard Function
- Univariate Vs. Multivariate Models
- Collecting the Data
The hazard function is a related probability that quantifies the probability of the event of interest occurring at a given time. If the relevant event has not occurred, the date of the last observation (e.g. the last appointment) is used.
Methods
- Kaplan–Meier Estimator
- Log-Rank Test
- Life Tables
- Cox Model
- Cox Model Assumptions
The limitation of the log-rank test or any other test that compares survival curves is the fact that it can only be applied to compare a fairly small number of survival curves. An important feature of the model is the basic hazard function, which is the hazard when all variances are equal to zero.
Global Epidemiology of Chronic Liver Disease
- Introduction
- Chronic Liver Disease in Africa
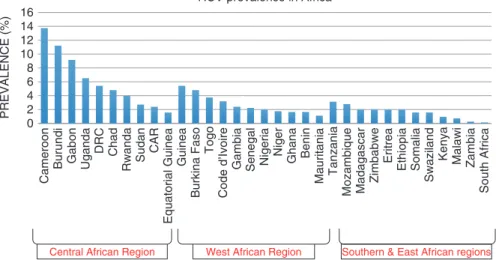
- Epidemiology of Chronic HCV Infection in Africa
- Epidemiology of Chronic HBV Infection in Africa
- Epidemiology of Alcoholic Liver Disease in Africa
- Epidemiology of Chronic Liver Disease in Asia .1 Epidemiology of Chronic HBV and HCV in Asia
- Epidemiology of NAFLD in Asia
- Epidemiology of Chronic Liver Disease in Europe .1 Epidemiology of Alcoholic Liver Disease in Europe
- Epidemiology of Chronic Hepatitis C in Europe
- Epidemiology of Chronic Hepatitis B in Europe
- Epidemiology of Hepatitis D Infection in Europe
- Epidemiology of Hepatitis E Infection in Europe
- Epidemiology of Non-Alcoholic Fatty Liver Disease in Europe
- Genetic Disorders (Haemochromatosis, Alpha-1- Antitrypsin Deficiency & Wilson’s Disease)
- Autoimmune Hepatitis
- Chronic Liver Disease in Latin America
- Epidemiology of Chronic HBV Infection in Latin America It is estimated that 7–12 million Latin Americans are chronically infected with
- Epidemiology of HCV Infection in Latin America
- Epidemiology of Non-Alcoholic Fatty Liver Disease in Latin America
Nonalcoholic fatty liver disease is increasingly cited as a cause of chronic liver disease in all regions of the world. NAFLD is increasingly cited as a cause of chronic liver disease in all regions of the world.
Epidemiology of Chronic Liver Disease in the United States
- Introduction
- General Epidemiology and Burden of Disease
- Non-alcoholic Fatty Liver Disease (NAFLD)
- Hepatitis C
- Hepatitis B
- Alcohol-Related Liver Disease
- Hepatocellular Carcinoma
In 2014, chronic liver disease and cirrhosis were the 12th leading cause of death in the United States [8]. Changes in the prevalence of the most common causes of chronic liver disease in the United States from 1988 to 2008. Prevalence of nonalcoholic fatty liver disease in the United States: the Third National Health and Nutrition Examination Survey, 1988-1994.

Epidemiology of Alcoholic Liver Disease
Taylor Richardson and Ashwani K. Singal
- Introduction
- Natural History of Alcoholic Liver Disease
- Historical Perspective of Alcohol Use
- Alcohol Consumption
- How Alcohol Causes Liver Disease?
- Factors Associated with the Development of Alcoholic Liver Disease (Fig. 7.3)
- Type of Alcohol
- Pattern of Drinking
- Gender
- Ethnicity
- Obesity
- Viral Hepatitis
- Genetic Factors
- Smoking
- Coffee
- Iron
- Magnitude and Burden of Alcoholic Liver Disease
- Worldwide Trends in Alcoholic Liver Disease
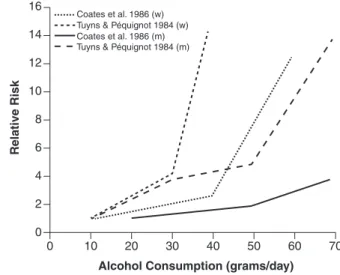
Multiple studies have shown a dose-dependent relationship between alcohol and the development of alcoholic liver disease. Meta-analysis of the effects of alcohol dehydrogenase genotype on alcohol dependence and alcoholic liver disease. Alcoholic liver disease—the extent of the problem and what you can do about it.

Hepatitis B Virus: Asian Perspective
- Introduction
- Natural History
- Epidemiology: HBsAg Seroprevalence
- Mainland China and Hong Kong
- Taiwan
- Korea
- Japan
- Mongolia
- South East Asia
- South Asia
- Central Asia
- Epidemiology: Anti-HBc Seroprevalence
- Molecular Epidemiology
- Nucleoside Analogue Prescription Coverage
- Concluding Remarks
A territory-wide survey of hepatitis B virus seroprevalence in the general population after the era of universal hepatitis B immunization in Hong Kong, China (abstract). Prevalence of hepatitis B in southeast China: a population-based study with a large sample size. A study on the seroprevalence of basic antibodies to hepatitis B and other transfused infections in blood donors.

Viral Hepatitis: The African Experience
- Introduction
- The Devastating Burden of Viral Hepatitis in Africa
- Preventative Strategies .1 Vaccination
- Prevention of Transmission
- Screening
- Population-Based Approaches: The Gambian Experience
- Future Strategies
Gambia is the smallest country on the African continent with a population of 1.8 million people. The third phase of the study consists of identifying cases of HCC and chronic liver disease in the study groups and linking them to their vaccination status. Population-based interventions to reduce the public health burden of hepatitis B virus infection in The Gambia, West Africa.
Hepatitis B: The Western Perspective
- Introduction
- Prevalence: The Americas
- Prevalence: Europe
- Vaccination and Pregnancy
- Transmission
- Special Populations at Risk: Injection Drug Users
- Special Populations at Risk: Incarcerated Individuals Due to a combination of factors including criminalization of drug use, criminal-
Prevalence of chronic hepatitis B among foreign-born persons living in the United States, by country of origin. Data supporting the updated estimates of the prevalence of chronic hepatitis B and C in the United States. Eliminating the public health problem of hepatitis B and C in the United States: phase one report.
Hepatitis D Virus
- Introduction
- The Unique Biology of HDV
- The Complex Epidemiology of HDV
- Problems in the Clinical–Epidemiological Analysis
- The Clinical–Epidemiological Scenarios
- The Current Clinical Epidemiology in the Developing World
- Current Clinical–Epidemiological Pattern in the Developed World
- Clinical Changes
- HDV and Hepatocellular Carcinoma
- Concluding Remarks
HDV infection remains endemic in the eastern Mediterranean [ 29 , 30 ] and throughout Asia [ 31 ]; high prevalence rates have been reported in Russia east of the Urals [32, 33], Pakistan [34], Iran [35] and Tajikistan [16, 35], and in specific populations in Vietnam [36, 37], as in Mongolia in general [38], with correspondingly high rates of cirrhosis and hepatocellular carcinoma (HCC). A comprehensive summary of knowledge about HDV and the prevalence and health impact of hepatitis D in the 1980s, when the HDV epidemic was raging throughout southern Europe. Noticing the initial decline of HDV in Europe in the 1990s; analysis of factors affecting decline.
Clinical Epidemiology of Hepatitis C Virus
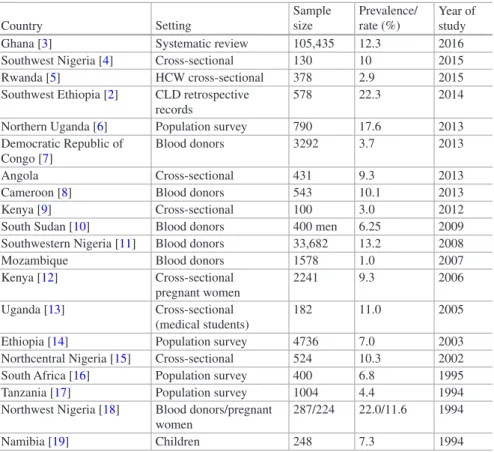
Global Prevalence
In Nigeria, initial estimates reported 7.5 million chronically infected persons, but this was revised to 2.8 million in 2016 [4–6]. This is particularly true in LMICs where transmission of HCV occurred in the health care setting in the 1960s and 1970s.
Genotypes and Genotype Distribution
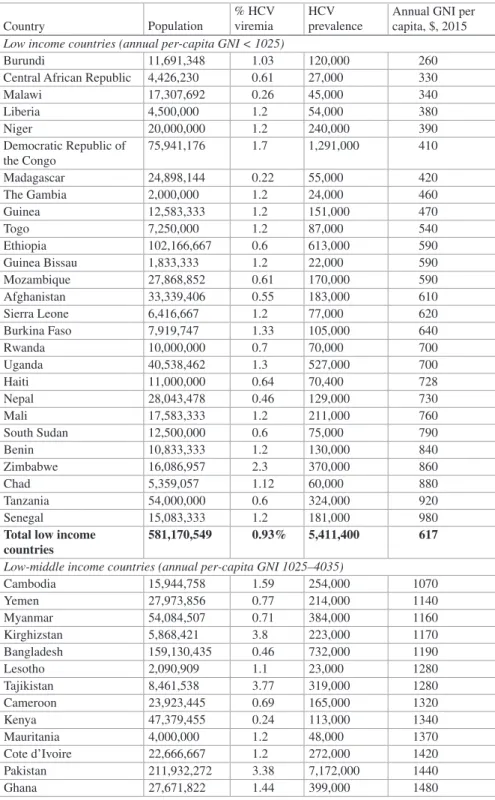
Variability of HCV by gross national income (GNI): Low-income countries, defined as annual per capita GNI of less than $1025, have an estimated 5.4 million chronically infected persons [ 20 , 21 ]. Upper-middle-income countries, defined as annual GNI per capita 4035 to <$12,475, are home to approximately 23.3 million persons with CHC. High-income countries, defined as annual GNI per capita, account for 16.7 million cases of CHD globally.
Incidence
The Q80K variant is present in more than 30% of patients with genotype 1a infection but only in 0.5%. Additionally, NS5A resistance-associated variants (RAVs) at positions M28, Q30, L31, and Y93 are found in 5–10% of genotype 1a treatment-naive patients and decrease response to NS5A-containing regimens [ 17 ]. Lower-middle-income countries, with annual GNI per capita between $1025 and <$4035, account for an estimated 32.4 million chronically infected persons.
Acute HCV Infection
In addition, genotype 3 infection was difficult to treat with the first generation of highly effective DAAs, but now has equal cure rates with subsequent generations of DAAs [ 19 ]. Unfortunately, many of these countries have limited capacity to diagnose and treat their large burden of chronically infected patients. This requires a global effort to improve access to HCV treatment where it is most needed (Table 12.1).
HCV Transmission
The age-related HCV seroprevalence rates in a community are related to the common method of transmission. In LMICs where unsafe healthcare injections play an important role in transmission (such as in Egypt [43], Pakistan [44], Turkey [45], Mongolia [46], and parts of China [47]), HCV seroprevalence rates are steadily increasing with age (Fig. 12.2). Although an increased risk of HCV infection has been reported in individuals with multiple sex partners, there is no evidence of transmission in monogamous relationships.
Clinical Manifestations
Prognosis of HCV
Factors Affecting Rate of Progression of Fibrosis
Complications from HCV Cirrhosis
Death from liver disease occurred in 19%, mainly due to HCC, indicating that in this population HCC was the most frequent and life-threatening complication. In a community-based long-term prospective cohort study involving 23,800 adults over a 16.2-year follow-up (REVEAL-HCV study), mortality during the study period due to liver disease was 12.8% for patients who had chronic HCV infection, 1.6% for those who were HCV seropositive but with undetectable HCV RNA, and 0.7% for seronegative individuals. Mortality rates from extrahepatic causes were 19.8% for patients who had CHC, 12.2% for HCV-seropositive individuals, and 11.0% for seronegative individuals [73].
Effect of Treatment Outcome
This is higher than the 5-year cumulative rates for other causes of cirrhosis, including HBV-related cirrhosis and alcoholic cirrhosis [71]. The most common complication was HCC, occurring in 21% of cases, followed by ascites (19%), gastrointestinal bleeding (4.5%), and encephalopathy (2%).
Future Trends and Prospects
Simeprevir plus sofosbuvir in patients with chronic hepatitis C virus genotype 1 infection and cirrhosis: a phase 3 study (OPTIMIST-2). Prevalence, incidence and risk factors of hepatitis C virus infection among drug users in Amsterdam. Recommendations for the prevention and control of hepatitis C virus (HCV) infection and HCV-related chronic diseases.
![Fig. 12.3 Dynamic course of HCV infection in the US. As the cohort born between 1945 and 1965 ages, a greater fraction will have HCV infection for sufficient time at old-enough ages to develop liver failure and HCC [3]](https://thumb-ap.123doks.com/thumbv2/azdoknet/10578329.0/166.659.115.544.88.342/dynamic-infection-greater-fraction-infection-sufficient-develop-failure.webp)
Enteric Hepatitis Viruses: Hepatitis A Virus and Hepatitis E Virus
Introduction
Viral hepatitis was the seventh leading cause of death in 2013, up from tenth in 1990. The 2014 World Health Assembly requested the World Health Organization (WHO) to investigate the feasibility of eliminating viral hepatitis by 2030. It was proposed that the viral hepatitis The hepatitis response should achieve five prevention and treatment service coverage targets by 2030.
Hepatitis A Virus
- Historical Background
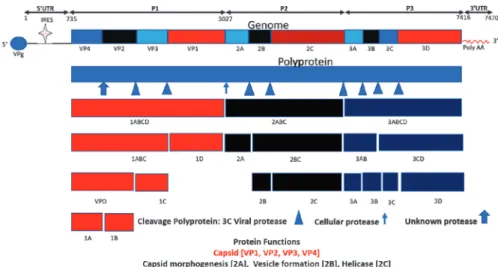
- Morphology
- Replication
- Global Epidemiology
- Mode of Transmission
- Clinical Manifestations
- Laboratory Features and Diagnosis
- Treatment
- Global Control
There is exposure to HAV infection in older children and adolescents and most of these infections are symptomatic. Countries with improved socioeconomic status and high to moderate endemicity have high rates of HAV infection in adults. However, the majority of the adult population does not have anti-HAV and is susceptible to HAV infection.
Hepatitis E Virus
- Historical Background
- Morphology
- Replication
- Global Epidemiology
- Mode of Transmission
- Clinical Manifestations
- Laboratory Manifestations and Diagnosis
- Treatment
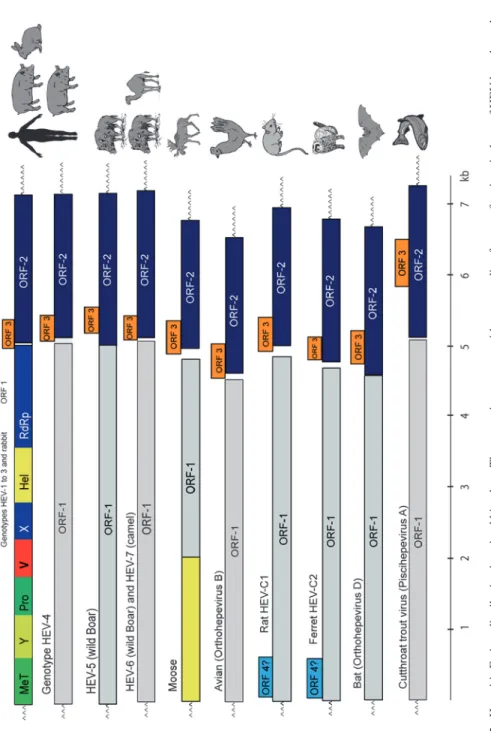
See text for detailed classification of hepatitis E viruses (Khuroo MS, Khuroo MS, Khuroo NS. Epidemics of hepatitis E do not occur, and a small percentage of endemic hepatitis in adults is etiologically related to HEV infection. Transmission of hepatitis E from one person to person transmission has been documented during an epidemic of hepatitis E [121].
![Fig. 4.1 Survival curve evaluating overall survival in patients treated with sorafenib [5]](https://thumb-ap.123doks.com/thumbv2/azdoknet/10578329.0/42.659.86.569.570.871/survival-curve-evaluating-overall-survival-patients-treated-sorafenib.webp)