We hope this book will help healthcare providers recognize the role of medications in increasing the risk of falls. Whatever your preference, Louise and I hope this book will help you understand and appreciate the subject of medication-related falls in older people.
Third, policymakers can use this book and the knowledge and data embedded in its chapters to develop systems (environmental, social, health, education) that can help address this global problem. Although this book is destined to be available primarily in electronic format, we hope that it also finds a place on your bookshelf.
The Aging Population and Falls
Falls are a major concern for many older adults, as approximately one-third of older adults in this community fall each year. Falls are not only costly, but can also have a significant impact on the lives of older adults.
Falls are a common health concern among older adults and have a significant impact on both the individual and the health care system. Stubbs B, Binnekade T, Eggermont L, Sepehry AA, Patchay S, Schofield P (2014) Pain and the risk of falls in community-dwelling older adults: systematic review and meta-analysis.
Falls Count and Counting Falls: Making Sense of Data About Falls
Falls Are an Important Health Concern
Going beyond patients' perspective, falls also represent a financial burden for the healthcare system [6. According to the Public Health Agency of Canada [1], more than $2 billion is spent each year on fall-related expenses in the senior population.
Statistical Methods Depend on the Type of Data Collected
Falls Are Not Measured, They Are Counted: Hence, Falls Count
Another important determinant of the choice of statistical methods is whether the investigator wants to estimate a parameter, usually about the magnitude of risk across different groups, or simply wants to find out whether any observed differences could have occurred by chance. CI is interpreted in the context of repeated samples such that if the study was repeated again and again, e.g.
What Kinds of Questions Can Be Asked About Falls?
- How Many People Fall?
- Are Falls Getting More Common or Rarer?
- What Are the Risk Factors for Falls?
- Did Intervention Reduce Falls?
Experiment Direct or indirect manipulation of the risk factor changes the rate of population decline. Instead of the pattern being as above [score (falls) = risk factor level], the pattern is reversed [risk factor level = falls].
The Case of the Pre-/Post-implementation Study
The regression parameter for time yields the incidence rate ratio and can be calculated directly from the data presented in the study. The authors report that the interaction term was 'significant', meaning that the effect of institution depended on time, so that the fall rates in the institutions grew apart over time as expected due to the implementation of the FallSafe program.
The Case of the Simple Randomised Controlled Trial
What cannot be directly calculated is the 95% CI, because each unit represents a cluster, such that individuals in the cluster are more similar to each other than individuals in other clusters. Of the 169 people in the intervention group, 67% had one or more falls compared to 41% in the control group, which was the opposite of what was desired.
The Case of the Complex Clustered Randomised Trial
First, to compare the proportion of people with one or more falls, Poisson regression was used with the number of falls and the natural logarithm of the group-specific population as denominator. In this study, the fall was analyzed using negative binomial regression and generalized estimating equations (GEE), a form of regression that adjusts for clustering, using department as the cluster variable and group as the variable under investigation.
The Case of the Observational or Non-randomised Trial
This study would today be classified as a cluster randomized trial, although in that era, considering the effect of clustering in the analysis would have been rare [41. In reporting HR or relative risks, it is important to place the effect in the context of the effect size (absolute risk).
The Case of the Stepped Wedge
This was borne out by the raw data which showed a control period drop rate of 13.78% and an intervention period drop rate of 7.80. As there is much evidence for the effectiveness of fall prevention programs, the next challenge will be to apply this information so that existing knowledge can be translated into routine clinical practice.
Lessons Learned
The outcome is the number of falls; similar to the Poisson model for overdispersed data (variance greater than the mean) [55. A report from the Kellogg International Work Group on the Prevention of Falls by the Elderly.
Drugs and Falls: Why Are Older People at Risk?
Introduction
The World Health Organization defines polypharmacy as "the administration of several drugs at the same time" or "the administration of too many drugs" [ 10. Although the use of multiple drugs may be appropriate for the management of a chronic disease in some situations, polypharmacy is associated with many iatrogenic consequences.
Medication Use in Older Patients
Finally, the use of ineffective drugs, agents without clinical indication and therapeutic duplication appears to be common. Polypharmacy results from the use of prescription drugs, over-the-counter (OTC) medications, and supplements.
Contributing Factors
A study of elderly outpatients found that 55% were taking at least one medication that lacked an indication, 30% were taking agents that were considered ineffective, and 16% had a therapeutic duplication. In a group of outpatient US veterans, 57% took at least one medication that was ineffective, not indicated, or a therapeutic duplication [22.
Consequences of Polypharmacy
- Exposure to Potentially Inappropriate Medications
- Adverse Drug Events
- Geriatric Syndromes
- Functional Decline
- Nutritional Status
- Lower Urinary Tract Symptoms and Urinary Incontinence
- Cognitive Impairment
- Falls
A study using data from 975 women participating in the Women's Health and Aging Study found that the use of five or more medications was associated with reduced ability to perform IADLs [ 59. A survey of 1,000 community-dwelling subjects. 65 years and older found that polypharmacy (defined as five or more drugs) was associated with reduced intake of B vitamins, fat-soluble vitamins, fiber, and minerals such as iron [66.
Strategies to Reduce Polypharmacy
By American Geriatrics Society 2015 Beers Criteria Update Expert Panel (2015) American Geriatrics Society 2015 updated the Beers Criteria for potential inappropriate medication use in older adults. Petrovic M, van der Cammen T, Onder G (2012) Adverse events in the elderly: detection and prevention.
Background
- Age-Related Changes in Pharmacokinetics
- Absorption
- Distribution
- Metabolism
- Elimination
- Potentially Inappropriate Medications
- Prescribing Cascade
- Geriatric Syndromes
For frail elderly patients with low muscle mass and low creatinine levels, a "normal" value for serum creatinine concentration should be substituted for the actual measured value when used in the formula to estimate creatinine clearance. Prescription cascades are commonly seen in elderly patients but are rarely detected and reported in the literature.
Optimizing Drug Prescribing in the Elderly
Considering the presence of a geriatric syndrome as an atypical presentation of an ADE should be included in the differential diagnosis of a clinical scenario. In the community pharmacy setting, problems identified are processing multiple patient prescriptions at the same time, errors related to verbal orders, and dispensing errors.
Strategies to Reduce Fall Risk-Increasing Drugs
Absence or failure to reconcile medications during admission or discharge led to medication errors. Simplify the drug regimen if appropriate; consider prescribing with a stepwise approach reducing a medication at the same time with adequate follow-up.
Conclusions
American Geriatrics Society 2012 Beers Criteria Update Expert Panel (2012) American Geriatrics Society updated the Beers Criteria for potential inappropriate medication use in older adults. American Geriatrics Society 2015 Beers Criteria Update Expert Panel (2015) American Geriatrics Society 2015 updated the Beers Criteria for potential inappropriate medication use in older adults.
Age-Related Physical and Physiologic Changes and Comorbidities in Older People
Introduction
Unlike normal and age-related physical and physiological changes, which are irreversible, optimal medical management of comorbidities are crucial and effective interventions that can reduce fall risk in the elderly. In addition, the impact of comorbidities will be examined from an intervention perspective, intended to reduce their role in fall risk.
- Postural and Mobility Changes
- Musculoskeletal Changes
- Changes in the Brain and Nervous System
- Changes in Heart and Blood Vessels
- Changes in Kidney Function and Urinary Tract
Finally, in terms of the cartilage, age-related changes in the joints are associated with pain and stiffness, which can affect mobility and predispose to falls. In theory, age-related changes in renal and urinary tract function should not be associated with falls [6.
Comorbidities and Falls in Older Persons
- Endocrine System
- Central Nervous System
- Cardiovascular System
- Kidney and Urinary Tract
- Sensory Systems
- Nutritional Defi cits
- Musculoskeletal Diseases
Vitamin D deficiency, even in the absence of kidney disease, has been associated with a high risk of falls. Iron deficiency is also associated with falls due to anemia [10], which is closely related to sarcopenia.
Conclusion
Secondly, it is associated with high levels of homocysteine, which is associated with the accelerated development of peripheral vascular disease. Sanders KM, Scott D, Ebeling PR (2014) Vitamin D deficiency and its role in muscle-bone interactions in the elderly.
Introduction
Falls: A Preventable Public Health Crisis
The total cost of falls in the UK population aged 60 and over was £981 million, and the highest overall cost component was attributed to inpatient admission, followed by long-term care [7. The fall-related costs were estimated at 1.5. % of total health care expenditures in the US, which corresponds to 0.2 % of gross domestic product [12.
Adverse Events in the General Population
This section will provide a brief overview of what is known about adverse reactions in the general population. It is clear that side effects are relatively common in the general population and can be prevented up to 50% of the time.
Adverse Events in the Elderly
- Adverse Events in the Home Care Setting
- Adverse Events in Long-Term Care
Most AEs and preventable AEs occurred in the physician's office and emergency department [17. Half of the AEs in the home care population studied resulted in moderate (recovery expected in 1 or more months to permanent impairment with disability ≤50%) to serious impairment (permanent impairment with disability >50% or death) [21.
Falls: A Potentially Preventable Adverse Event
- Rate of Falls as an AE in the Elderly
- Vulnerability to In-Hospital Fall-Related Injuries and Poor Outcomes
- Falls in Home Care and Long-Term Care Settings
- Fall Prevention in Healthcare Setting
In the nursing home setting, Gurwitz and colleagues [23] found that the most common AEs in their study in nursing home residents were falls, but the majority of falls did not result in any injury. These findings further highlight the importance of falls in the healthcare setting as a significant patient safety issue for geriatric patients and the healthcare system.
Adverse Drug Events and Falls
- Epidemiology of Adverse Drug Events
- ADEs and the Falling Elderly Patient
- ADEs and the Elderly in Ambulatory Care
- ADEs and the Elderly in Long-Term Care
Gurwitz and colleagues later published another study that looked at all long-term care residents in Massachusetts, which included 18 nursing homes, and the incidence of adverse drug events in a cohort study [44. They found that the rate of adverse drug events was 1.89 per 100 resident months, and the rate of preventable adverse drug events was 0.96 per 100 resident months.
Conclusion
Bates DW, Spell N, Cullen DJ et al (1997) Costs of adverse drug reactions in hospitalized patients. Gurwitz JH, Field TS, Avorn J et al (2000) Incidence and preventability of adverse drug reactions in nursing homes.
Introduction
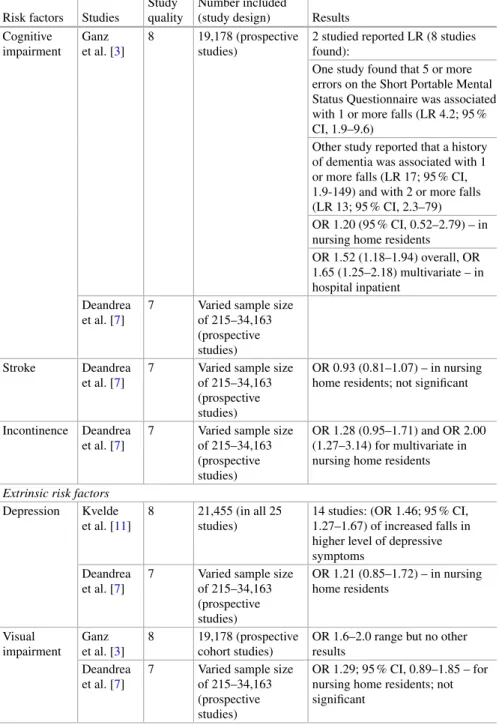
One method of classifying fall risk factors is to view them as intrinsic or extrinsic. However, this chapter will focus on evidence-based risk factors identified in high-quality systematic reviews (defined as ≥7 on A Measurement Tool to Assess Systematic Reviews (AMSTAR)) [6.
Search Strategy
In general, this can lead to conflicting results because there are so many ways to measure and examine risk factors for falls [ 3. Another method for classifying risk factors for falls includes the following categories: sociodemographic, balance/mobility, sensory/neuromuscular, psychological, medical factors, drug factors and environmental factors [ 5.
Risk Factors of Falls
- History of Falls
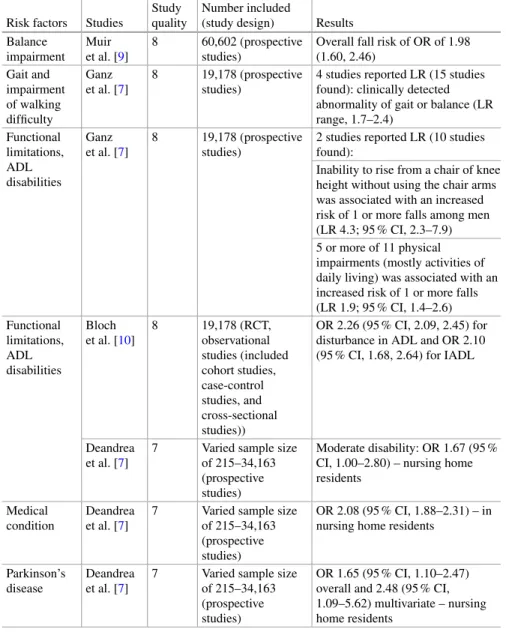
- Functional Impairment
- Medical Conditions
- Cognitive Impairment
- Depression
- Visual Impairment
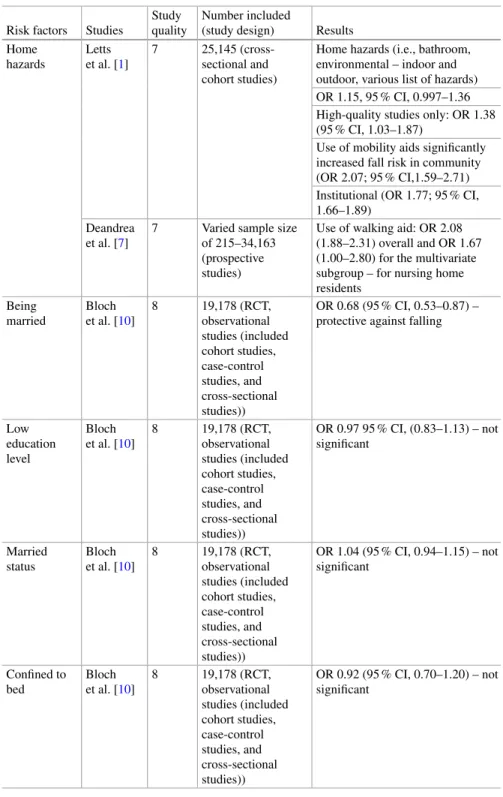
- Home Hazards
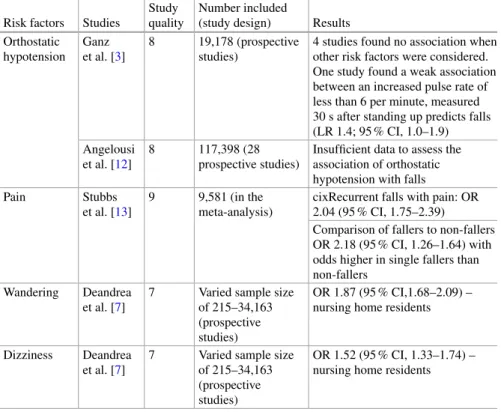
- Orthostatic Hypotension
- Pain
- Medications
Intrinsic risk factors look at specific causes within an individual person, while extrinsic risk factors are those factors that are extrinsic to the individual [4. Patients with a greater number of depressive symptoms (different measures used with different cutoffs for the highest level of depressive symptomatology including the Center for Epidemiological Studies Depression Scale, the Minimum Home Care Data Set, the Mental Health Inventory, the Montgomery-Asberg Depression Rating Scale, the outcome and Assessment Information Set, the Symptom Checklist, the Cornell Scale and the Geriatric Depression Scale) have an increased fall risk (OR CI or relative risk (RR CI) compared to those with fewer symptoms [11.
Chapter Summary
Deandrea S, Lucenteforte E, Bravi F, Foschi R, La Vecchia C, Negri E (2010) Risk factors for falls in community-dwelling elderly: a systematic review and meta-analysis. Muir SW, Berg K, Chesworth B, Klar N, Speechley M (2010) Quantifying the magnitude of risk for fall balance impairment in community-dwelling older adults: a systematic review and meta-analysis.
Medications Associated with Falls in the Elderly
Introduction
The underlying mental health conditions for which psychotropic medications are prescribed can themselves pose a fall risk. This chapter discusses the extent and nature of the fall risk associated with the use of psychotropic medications and discusses ways to moderate this risk.
Antidepressants
- Epidemiology of Antidepressant-Related Falls
- Potential Mechanisms of Antidepressant-Related Falls and Fractures
- Prevention of Antidepressant-Related Falls
In this study, mirtazapine was associated with a small increased risk of falls, although less so than SSRIs [17. In a prospective study over an 8-year period, increases in depressive symptoms were associated with an increased rate of falls [2.
Antipsychotics
- Epidemiology of Antipsychotic-Related Falls
- Potential Mechanisms of Antipsychotic-Related Falls
- Prevention of Antipsychotic-Related Falls
In older persons, medication should be dosed lower and increased more slowly, especially during the first weeks of treatment. There is limited information on the effect of antipsychotics on bone health in older adults.
- Antiepileptic Drugs
AEDs are also commonly used in older adults to treat bipolar disorder, pain disorders, and off-label for the behavioral symptoms of dementia. Steps should be taken to prevent bone density loss in older adults prescribed AEDs, such as ensuring adequate vitamin D levels.
Summary and Conclusions
Iaboni A, Flint AJ (2013) The complex interplay of depression and falls in older adults: a clinical review. Whooley MA, Kip KE, Cauley JA, Ensrud KE, Nevitt MC, Browner WS (1999) Depression, falls and risk of fracture in older women.
Introduction
Benzodiazepines
The concentration in the cerebrospinal fluid is almost equal to the concentration of the free drug in the plasma. BZDs are primarily metabolized in the liver; most of these compounds can be classified as low clearance drugs [27.
Benzodiazepines: Effects and Adverse Effects
Susceptibility of Older Patients to Benzodiazepines
Elderly patients are more sensitive to the influence of BZDs on cognitive function, especially at higher doses. When looking at the clinical effects of BZD use in elderly patients, a high risk of side effects has been reported.
Benzodiazepine-Related Falls
In this study, the incidence of harmful falls in subjects aged 80 years or older exposed to BZDs was 2.8 per 100 person-years. According to the results of this study and recent population estimates, BZD use in France could be responsible for almost 20,000 falls involving injuries in persons aged 80 years or older and for almost 1800 deaths.
Risk Factors for Benzodiazepine Use
Benzodiazepine use was significantly associated with the occurrence of harmful falls, increasing with age, in a nested case-control study using data from a community cohort collected over ten years (the personnes âgées QUID-PAQUID or 'elderly as subject'). 'cohort) [12.
Approach and Interventions
However, general practitioners should be involved in the decision to stop the BZD treatment, in addition to the follow-up after discharge from the hospital. National quality programs should include awareness campaigns to avoid long-term use of BZD in all citizens, with special focus on older patients.
Conclusion
Petrovic M, Mariman A, Warie H, Afschrift M, Pevernagie D (2003) Is there a rationale for prescribing benzodiazepines in the elderly. Softić A, Beganlič A, Pranjić N, Sulejmanović S (2013) The effect of benzodiazepine use on the frequency of falls in the elderly.
Drugs for Degenerative Neurologic
Conditions: Antiparkinson Medications, Cholinesterase Inhibitors, and Memantine
Introduction
These medications are often used in a population with a higher baseline risk of falls secondary to their underlying neurological and medical conditions. First is a review on cognitive enhancers: cholinesterase inhibitors (which include the currently approved medications galantamine, donepezil, and rivastigmine) and memantine.
Cognitive Enhancers
- Cholinesterase Inhibitors
- Effects on Gait/Balance
- Association with Falls in Patients with Dementia
- Association with Falls in Patients with Parkinson’s Disease (PD)
- Summary
- Memantine
- Summary
Finally, Kim [30] performed a meta-analysis of 22 studies (RCTs and extension studies) to assess the effect of CIs on the risk of falls, syncope, and related events. None of these results suggest an increased risk of falls with memantine use.
Antiparkinson Medications
- Effect on Gait and Balance
- Antiparkinson Medication Association with Falls
- Summary
Hiorth YH, Larsen JP, Lode K, Pedersen KF (2014) Natural history of falls in a population-based cohort of patients with Parkinson's disease: an 8-year prospective study. Wood BH, Bilclough JA, Bowron A, Walker RW (2002) Incidence and prediction of falls in Parkinson's disease: a prospective multidisciplinary study.
Antihypertensives and Cardiovascular Medications
Introduction
Due to the use of antihypertensive drugs in the elderly population, patients are exposed to an increased risk of adverse drug effects in both hospital and outpatient settings [1, 2]. These side effects, including balance and gait disturbances, dizziness, and autonomic dysregulation, contribute to orthostatic hypotension. are among the most common and increase the patient's risk of falling and breaking [3, 4.
Hypertension Treatment Goals in Older Adults
In general, these societies often recommend higher blood pressure goals in the older population compared to younger healthy adults. Blood pressure targets in older patients have been recommended by a number of other professional medical societies.
Associations Between Cardiovascular Medications and Falls: The Evidence
- Randomized Controlled Trials
- Observational Studies
- Systematic Reviews
Well-known, notable randomized controlled trials have described the risks of falls and fall-related injuries in older adults taking antihypertensive medications. The associations between antihypertensive and cardiovascular medications and falls and fall-related injuries have been examined by a number of observational studies.
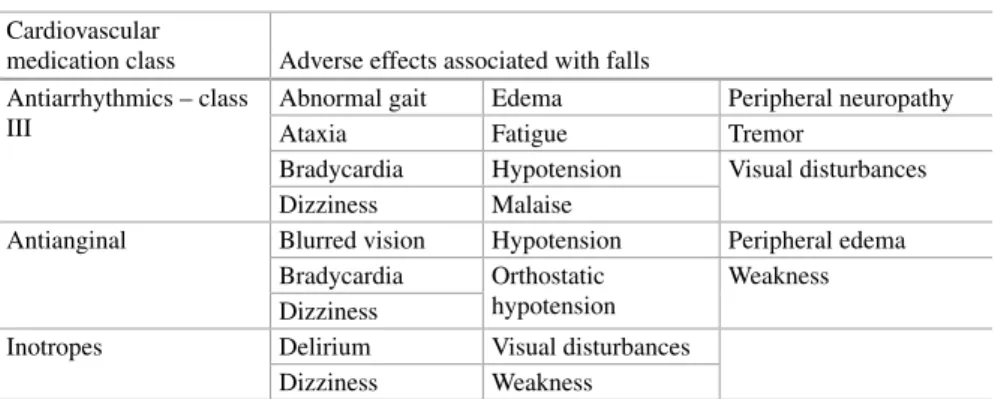
Other Common Adverse Effects of Cardiovascular Medications
Conclusions
Cushman WC, Ford CE, Cutler JA et al (2002) Success and predictors of blood pressure control in diverse North American settings: the antihypertensive and lipid-lowering treatment to prevent heart attack (ALLHAT). Gribbin J, Hubbard R, Gladman JR et al (2010) Risk of falls associated with antihypertensive medications: population-based case-control study.
Introduction
- Retinopathy and Visual Impairments
- Nephropathy and Oral Hypoglycemic Agents
- Bone Fragility
Doses of oral hypoglycemic agents and insulin should be carefully selected to avoid hypoglycemia, which can lead to an increased risk of falls and fall-related morbidity in the elderly. The A Diabetes Outcome Progression Trial (ADOPT) reported an increased risk of peripheral fractures in women taking rosiglitazone but no increased risk of falls [23.
- Metformin
- Other Agents
Thiazolidinediones have been found to double the risk of distal upper and lower limb fractures in women compared with other oral hypoglycemic agents. There is limited data on the increased risk of falls or fractures with other types of diabetes medications.
Conclusion
Berlie HD, Garwood CL (2010) Diabetes medications related to an increased risk of falls and fall-related morbidity in the elderly. Lapane KL, Yang S, Brown MJ, Jawahar R, Pagliasotti C, Rajpathak S (2013) Sulphonylureas and risk of falls and fractures: a systematic review.
Management of Medication-Related Falls
Inappropriate Medications and Risk of Falls in Older Adults
- Introduction
- Skeletal Muscle Relaxants
- Multiple Central Nervous System Medications
- Antiepileptic Drugs
- Opioids
- Conclusion
SMR, AED, and opioids have been shown to increase the risk of falls and hip fractures in older adults. Buckeridge D, Huang A, Hanley J et al (2010) Risk of injury associated with opioid use in older adults.
Identifying Explicit Criteria for the Prevention of Falls
- Introduction
- Development of Explicit Criteria
- Explicit PIP Criteria and Fall Prevention
- Beers Criteria
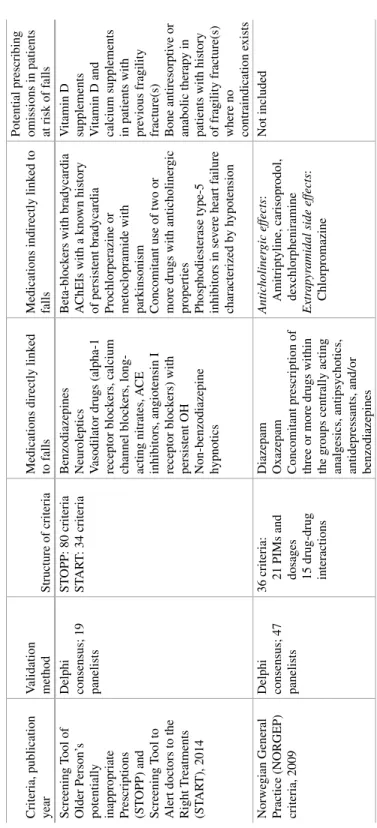
- STOPP/START Criteria
- NORGEP Criteria
- PRISCUS Criteria
- Conclusion
PIMs to avoid in adults with specific conditions (including those with a history of falls and syncope) 3. Unlike the Beers and STOPP/START criteria, the NORFEP criteria are not structured in ways that highlight PIMs that should be avoided in older adults at risk of falls.
Approach to Medication Reviews in Older Adults
- Medication Review vs. Medication Reconciliation
- Rationale for Conducting Medication Reviews
- Principles of Medication Review
- Structure
- Process
- Outcome
- Medication History
- Analyzing Medication History
- Conclusion
- Introduction
- Effects and Effectiveness of Interventions Aimed at Withdrawal of Fall Risk-Increasing Drugs
- Randomized Controlled Trials of Withdrawal of Fall Risk-Increasing Drugs
- Non-randomized Trials of Withdrawal of Fall Risk- Increasing Drugs
- Effects of Multiple Pharmacotherapy-Related Interventions
- Pharmacist-Led Medication Review
- Physician-Led Medication Review
The first step in the medication review process is to determine exactly which medications your elderly patient is taking. In the case of a patient taking a previously well-tolerated medication, an acute illness may also increase the risk of falls.